Keywords
Ampulla of Vater; Neuroendocrine Tumors; Pancreaticoduodenectomy
Abbreviations
ANET: ampullary neuroendocrine tumor
INTRODUCTION
A neuroendocrine tumor is defined as an epithelial neoplasm that shows neuroendocrine differentiation when analyzed by conventional histological, immunohistochemical, ultrastructural and biological evaluation [1]. Ampullary neuroendocrine tumor (ANET) are an extremely uncommon subset of pancreatic cancer that have a distinct clinical and morphological profile. ANET, formerly known as carcinoid tumors, account for only about 0.3 to 1% of all gastrointestinal neuroendocrine tumors, and even less than 2% of all periampullary cancers [2, 3]. To the best of our knowledge, a search of available English language literature revealed only about 139 patients with ANET that have previously been reported [1, 2, 3]. We report four cases of ANET with emphasis on their clinical presentation, pathology, treatment and outcomes.
MATERIAL AND METHODS
A retrospective review of the records of all the patients diagnosed as periampullary cancer at our hospital was performed, over a 6-year period, from January 2005 up to December 2010. A total of 52 patients were identified as having periampullary neoplasms, in whom the initial assessment was done with endoscopic retrograde cholangiopancreatography (ERCP) and final histopathological diagnosis was made from endoscopic biopsy or pancreaticoduodenectomy specimen. Of these, 48 (92.3%) were adenocarcinoma and 4 (7.7%) were neuroendocrine tumors.
Depending upon the stage of the disease at presentation, these periampullary cancers were either taken up for surgery (46 patients, 88.5%) or palliative endoscopic stenting (6 patients, 11.5%). Of the patients who were operated, 30 successfully underwent pancreaticoduodenectomy (65.2%) whereas 16 (34.8%) could only be palliated for their biliary/gastric obstruction.
The indoor records of the 4 patients of ANET were scrutinized for information regarding presentation, histopathology and management.
ETHICS
The informed consent was not taken as the study was retrospective review of the last 6 years, as well as the Declaration of Helsinki/IRB approval are not required in our institute for retrospective review studies.
STATISTICS
Descriptive statistics only were used (absolute and relative frequencies).
RESULTS
Neuroendocrine tumors accounted for 7.7% (4 out 52) of all tumors of ampulla. The details of these patients are tabulated in Table 1. Of these four patients, 2 were men and 2 were women. Although the mean age at presentation was 49 years (range 30-70 years), the female patients presented at a younger age as compared to the males. The common clinical presentation was with progressive jaundice (3 of 4 cases) and in the other, the presentation was with vague abdominal pain. One patient had associated neurofibromatosis. Endoscopic findings were similar in all the cases showing bulky ampulla with minimal mucosal ulceration. The diagnosis of ANET was made pretreatment only in one patient (Case #1). None of the patients had any symptoms/syndromes that could be attributed to hormonal hypersecretion by the ANET.
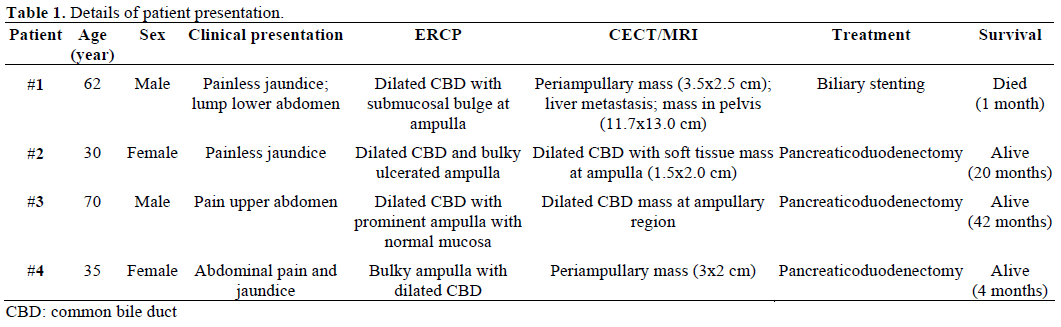
Three patients underwent pancreaticoduodenectomy, but in the fourth, palliative biliary stenting had to be performed since the disease was metastatic. The tumor in resected specimens were in form of bulky ampulla (Figure 1) and measured 1.7-2.5 cm. One out of the two patients with metastatic disease died within a month of stenting, but the other three patients who were operated are doing well on follow-up.
Figure 1. Clinical photograph showing submucosal lesion in
periampullary region (Case #3).
Histological diagnosis of neuroendocrine tumors was made on basis of typical neuroendocrine morphology seen on hematoxylin-eosin staining (H&E, Figure 2). Immunohistochemical staining was further used for establishing the diagnosis of ANET in these tumors; a positive stain for chromogranin A was seen in all our patients (Figure 3). Two patients had poorly differentiated (high grade) (neuro)endocrine carcinoma and two had well differentiated (one low grade and one intermediate grade) (neuro)endocrine carcinoma as per the WHO classification system (Table 2).
Figure 2. Photomicrograph showing nests of uniform looking tumor cells in the submucosa (Case #4; H&E x100).
Figure 3. Photomicrograph showing nest of tumor cells positive for
chromogranin A (Case #4; x200).

DISCUSSION
ANET are extremely rare tumors, accounting for less then 1% of all gastrointestinal neuroendocrine tumors and less than 2% of all tumors of ampullary region [3, 4]. To the best of our knowledge, only 139 cases have been documented in available English language literature till date, and only about 20% of these reported patients are of African or Asian Pacific origin [3].
Earlier, all neuroendocrine tumors arising in the gastrointestinal tract were called carcinoid tumors, but today, this terminology has been abandoned, and they are preferentially called neuroendocrine tumors (however, the term carcinoid is still used for low grade tumors). Histologically, although ANET are similar to neuroendocrine tumors arising from other parts of gastrointestinal tract, they have distinct ultrastructural and immunohistochemical behavior. Immunohistochemical staining is the main diagnostic method for these tumors, and ANET stain positively with chromogranin A and synaptophysin in 92-100% cases [4, 5].
According to the International Classification of Diseases of Oncology, published by the World Health Organization (WHO), the ampulla has been designated a site specific code “241” and neuroendocrine tumors are given specific codes: neuroendocrine not otherwise specified (8246); small cell neuroendocrine carcinoma (8041); and large cell neuroendocrine carcinoma (8013) [5]. The earlier system of identifying these tumors on the basis of hormones secreted or the clinical syndrome produced is no longer recommended, since the majority of these are not functional, and the prognosis of such tumors is based on their histological grade.
Various systems of nomenclature, grading and staging neuroendocrine tumors are prevalent which cause much confusion. But the majority of nomenclature system including WHO, European Neuroendocrine Tumor Society (ENETS) and TNM reflect differentiation and grading features of neuroendocrine tumors [6]. Essentially, in all systems, these tumors are categorized as well or poorly differentiated on the basis of their proliferative rates assessed by amount of necrosis, mitotic figures/HPF or Ki67 labeling index [6, 7, 8].
ANET do not show any sex predilection, and are seen equally among males and females. The Surveillance, Epidemiology, and End Results (SEER) database reported 76 males and 63 females out of a total of 139 cases of ANET, with an average age of 61 years for carcinoids (low grade ANET) and 62 years for high grade neuroendocrine tumors [3]. Again, although we also had an equal incidence in males and females, the age of presentation was much younger in the female patients.
Owing to its location at the ampulla, ANET mostly present with obstructive jaundice (53%), non specific upper abdominal pain (24%), pancreatitis (6.0%) or weight loss (3.6%) [9, 10]. Jaundice was the common presentation in our patients also, and the other patient who presented with non specific abdominal pain without jaundice was diagnosed on ERCP that was performed for dilated extrahepatic biliary system seen on ultrasound examination. At times, the presence of neurofibromas in such patients may indicate the possibility of ANET, since neurofibromatosis type 1 has a well documented association with gastrointestinal tumors such as neurofibromas, gastrointestinal stromal tumors (GIST) and periampullary carcinoids, and these may be seen in up to 25% of patients with neurofibromatosis [11, 12]. In a recent review, 76 patients with neurofibromatosis type 1 were found to have periampullary or duodenal neoplasms. Of these, 31% were found to arise from the ampulla, and somatostatinoma (40%) was the commonest tumor type [12]. Less than 3% patients with neuroendocrine tumor of ampulla have hormonal hypersecretion syndrome [13].
ERCP is commonly used to diagnose ampullary tumors as well as to obtain tissue for histopathology. ANET characteristically proliferate under an intact mucosa [14]. The finding of a submucosal bulge at the ampulla on endoscopic examination should raise the clinical suspicion of ANET; this is the reason that the rate of preoperative diagnosis on endoscopic biopsy is as low as 14% [4, 9]. Endoscopic ultrasound is helpful in detecting the depth of invasion and the presence of lymph node metastasis, but the facility may not be available at all the places. Computed tomogram scan and octreotide scan are helpful in a metastatic workup once the diagnosis of ANET is established [4, 15]. However, there are no specific features on imaging that can help in distinguishing ANET from the more common adenocarcinoma.
Tumor size has been regarded as a prognostic marker for adenocarcinoma of periampullary region. Singhal et al. in their comparison of adenocarcinoma and carcinoids of periampullary region observed that average size of carcinoid tumor was 5 cm and adenocarcinomas above 5 cm were seldom resectable [16]. However, tumor size does not predict the metastatic potential in ANET, and although a tumor size of more than 2 cm was found to be associated with lymph node metastasis, there are several reports of ANET up to 5 cm size without evidence of any metastasis [2, 17, 18].
Grossly neuroendocrine tumors of ampulla are small, solitary, polypoid and are covered with flattened mucosa. Microscopically the tumor is arranged in nests, microglandular, trabecular and rarely insular pattern. The tumor cells are small, uniform with scanty granular cytoplasm. The nuclei are regular, normochromic with scanty mitosis. Obvious evidences of malignant behavior are vascular invasion, gross local invasion or metastasis [3, 6].
The treatment protocol for ANET remains controversial, as they are rare tumors with an unpredictable biological behavior and prognosis [6]. Since tumor size has not been clearly established to correlate with lymph nodal positivity status, pancreaticoduodenectomy is often recommended as the treatment of choice for tumors of any size with no distant spread [10, 19, 20]. Although less invasive procedures like local excision and endoscopic resections have also been successfully attempted, especially for ANET less than 2 cm size or in high risk surgical candidates [13, 14, 21], extensive debulking surgery should be considered in patients with hormonal hypersecretion, even in the presence of advanced disease (extensive local or distant metastasis) since it offers survival rates of up to 80% at 5 years [6].
Tumor characteristics (grade) and distant metastasis are the most important prognostic factors in determining survival in ANET. Other tumor properties, like nodal involvement, tumor size and resection margins, appear to be of lesser significance in the long term survival [1, 22, 23, 24]. Low grade tumors show a 5- and 10-year survival rate to the tune of 80% and 71%, respectively, whereas high grade neuroendocrine tumors have dismal 5- and 10-year survival rates (15%) [3, 25].
Financial disclosure
None
Conflict of interest
The authors have no potential conflict of interest
References
- Selvakumar E, Rajendran S, BalachandarTG,KannanDG,Jeswanth S, Ravicahndran S. Neuroendocrine carcinoma of theampulla of Vater :a clinicopathogic evaluation. HepatobiliaryPancreat Dis Int 2008;7:422-425.
- Mavroudis N, Rafailadis S, Syemeonidis N, Aimoniotou E,Antonopoulos E, Evgenidis N etal Carcinoid of Ampulla of vater – areport of two cases.ActChirBelg 2005;105:213-216.
- Albores- Saavedra J, Hart A, Chable- Montero F, Henson DE.Carcinoid and high grade Neuroendocrine Carcinoma of the Ampullaof Vater- A camparitive analysis of 139 caese from Surveillance ,Epidemiology , and End Results Program- A population basedStudy.ArchPathol Lab Med 2010;134:1692-1696.
- JaoudeWA,Lau C, Sugiyama G, Duncan A. Management ofAmpullary Carcinoid tumor with Pancreaticoduodenectomy.JSCR2010;8:4.
- Beasley MB, Thunnissen FB, Hasleton P .Carcinoid tumor. InTravis WD, Brambilla E, Muller –Hermelink KH, Harris CC.Pathology and Genetics of Tumors of the lung , Thymus , Heart .Lyon, France :IARC Press; 2004:59-62.World Health OrganisationClassification of Tumors ; vol 10.
- Klimstra D, Modlin IR, Coppola D, Loyd R, Suster S. Thepathologic classification of neuroendocrine tumors, A review ofnomenclature, grading and staging systems. Pancreas 2010;39:707-12.
- BosmanF,CarneiroF,HrubanR,Theise N, eds.WHOClassificationof Tumors of The Digestive System.Lyon,France:IARC Press;2010.
- RindiG, KloppelG,Couvelard A.TNM staging of midgut andhindgut (neuro)endocrine tumors :a consensus proposal including agrading system.Virchow Arch.2007;451:757-62.
- Hartel M, Wente MN, Sido Bernd, Friess H, Buchler MW.Carcinoid of the ampulla of vater. Journal of Gastroenterology andHepatology 2005;20:676-681.
- Carter JT, Grenert JP, Rubenstein L, Stewart L, Way LW.Neuroendocine tumors of the Ampulla of vater. Biological behaviourand surgical management. Arch Surg 2009;144:527-531.
- Klein A, Clemens J, Cameron J. Periampullary neoplasms in vonRecklinghausen disease. Surgery 1989;106:815-9.
- Relles D, Back J, Witkiewicz A, Yeo CJ. Periampullary andDuodenal neoplasms in neurofibromatosis type I :two cases anupdated 20-year review of the literature yielding 76 cases. JGastrointestSurg 2010;14:1052-61.
- Gilani N, Ramirez FC. Endoscopic resection of an ampullarycarcinoid presenting with upper gastrointestinal bleeding : A casereport and review of literature.World J Gastroenterol 2007;13:168-70.
- Senda E, Fujimoto K, Ohnishi K, Higashida A, Ashida C,Okutani T etal. Minute ampullary carcinoid tumor with lymph nodemetastasis : a case report and review of literature. World Journal OfSurgical Oncology2009;7:9.
- Singhal D, Vasdev N, Soin A, Gupta S, Nundy S. Distinguishingbetween periampullary carcinoid and carcinomas: is this possiblepreoperatively.Indian J Gastroenterol 2006;25:206-7.
- KaratzasG,KouraklisG,KarayiannakisA,PatapisP,GivalosN,Kaperonis E. Ampullary and jejunal stromal tumor associated withVion Recklinghausen’s disease presenting as gastrointestinalbleeding and jaundice. Eur J SurgOncol 200;26:428-429.
- Hatzitheoklitos E, Büchler MW, Friess H, Poch B, Ebert M,Mohr W etal. Carcinoid of the ampulla of vater , clinicalcharacterstics and morphological features. Cancer1994 ;73:1580-1588.
- Makhlouf HR, Burke AP, SobinLH.Carcinoid of the ampulla ofvater : a comparison with duodenal carcinoid tumors .Cancer1999;85;1241-1249
- Norton JA, KivlenM , Li M, Scheider D, Chuter T, Jensen RT.Morbidity and mortality of aggressive resection in patients withadvanced neuroendocrine tumors. Arch Surg 2003;138;859- 866.
- PoultidesGA,Frederick WA. Carconoid of the ampulla of vater :Morphologic features and clinical implications. World JGastroenterol.2006;12:7058-60.
- Hwang S, Lee SG, Lee YJ, Han DJ, Kim SC, Kwon SH etal.Radical surgical resection for carcinoid tumors of the ampulla. JGastrointestSurg 2008;12:713-7.
- Pyun DK, Moon G, Han J, Kim MH, Lee SS, Seo DW.Acarcinoid tumor of the ampulla of vater treated by endoscopic snarepapillectomy. The Korean Journal of Internal Medicine 2004;19;257-260.
- Sakka N, Smith RA, Whelan P, Ghaneh P, Sutton R, Raraty Metal. A preoperative score for resected pancreatic and periampullaryneuroendocrine tumors.Pancreatology 2009;9;670-676.
- Jarufe NP, Coldham C, Orug T, Mayer AD, Mirza DF, BuckelsJA etal. Neuroendocrine tumors of the pancreas: predictors ofsurvival after surgical treatment. Dig Surg 2005; 22:157-162.
- Hochwald SN, Zee S, Conlon KC, Colleoni R, Louie O, BrennanMF etal. Prognostic factors in pancreatic endocrine neoplasms: ananalysis of 136 cases with a proposal for low-grade and intermediategrade groups. J ClinOncol 2002; 20:2633-2642.




