Keywords
Carcinoma; Classification; Neuroendocrine Tumors;
Pancreas
Abbreviations
NEC neuroendocrine carcinoma; NENs neuroendocrine
neoplasms; NET neuroendocrine tumors
INTRODUCTION
Neuroendocrine neoplasms (NENs) of the pancreas are
composed of epithelial neoplastic cells with phenotypic
neuroendocrine differentiation. NENs are potentially
malignant tumors including well-differentiated types
(neuroendocrine tumors, NETs) and poorly differentiated
types (neuroendocrine carcinomas, NECs) [1]. These
tumors are relatively rare, but are the second most common
neoplasm of the pancreas, accounting for approximately
1–2% of all pancreatic neoplasms [1, 2]. The incidence of
NETs of the pancreas has increased recently [3, 4].
In this short review updated clinicopathological features
and grading system of the pancreatic NEN are described.
Patients’ Characteristics and Clinical Diagnosis
Patients with NETs are typically from 30 to 60 years
old, and show no significant gender predilection [1, 2, 3, 4]. Because of lacking specific symptoms, non-functional
pancreatic NENs tend to be diagnosed at more advanced
stages of disease compared with functional pancreatic
NENs such as insulinoma and gastrinoma. Approximately
1–2% of patients with these tumors have predisposing
familial syndromes. However, patients with NEC tend
to be older, similar to patients with pancreatic ductal
adenocarcinoma.
In addition to a physical examination, imaging studies
including US, CT and MRI are useful to diagnose as NEN.
In addition, the endoscopic ultrasonography-guided fineneedle
aspiration (EUS-FNA) biopsy has enabled correct
pathological diagnosis and suitable treatment for the
tumors.
Histologic Grading and Classification
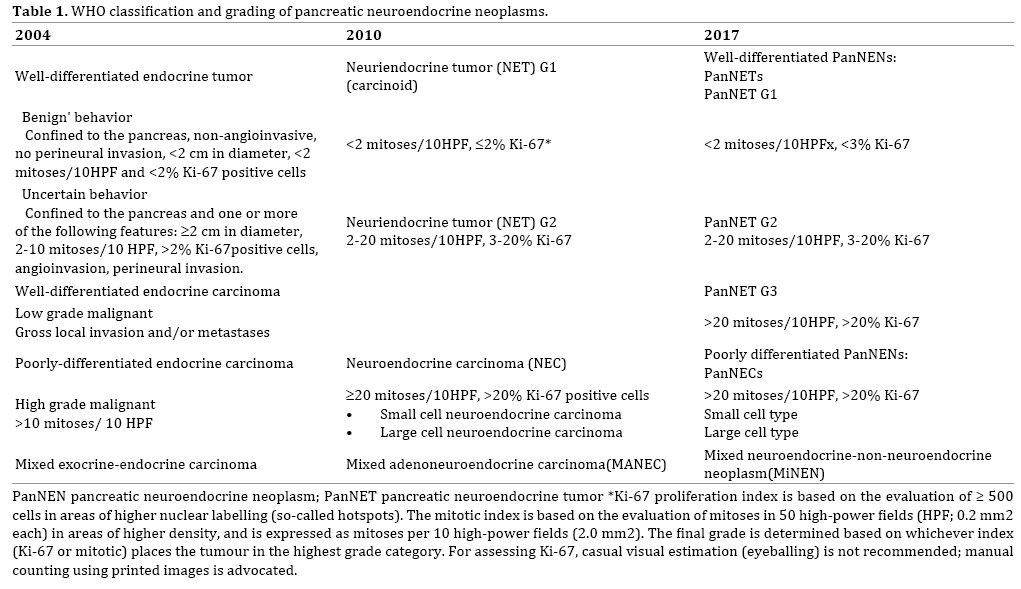
The WHO tumor classification of endocrine organs [5]
published in 2004 divided NENs into well-differentiated
NETs and well- and poorly differentiated neuroendocrine
carcinoma (NEC), and the former NETs were sub-classified
into benign and borderline tumors according to tumor
size, mitotic rate, lymphovascular invasion and perineural
invasion [5]. The 2010 WHO classification included several
major changes in the grading system of neuroendocrine
neoplasms of the digestive system. “Endocrine neoplasm”
was changed to “neuroendocrine neoplasm”, NENs are
now graded according to the number of mitoses and/or
Ki-67 index (using the MIB1 antibody), and this grading
system is applied to NENs arising in any organ of the
digestive system [1]. These changes were based on the Europian Neuroendocrine Tumor Society (ENETS)
consensus guideline [6]. In this classification, NENs were
divided into well-differentiated NETs (NET G1 and G2) and
poorly differentiated NEC. NET G1 was defined as having a
Ki 67 index of ≤2% and <2 mitoses/10 high power fields
(HPF). NET G2 was defined as a Ki-67 index of 3 to 20% or
2 to 20 mitoses/10HPFs. NEC was defined as a Ki-67 index
of >20% and >20 mitoses/10HPFs. The WHO recommends
that for mitotic counts, at least 50 HPFs should be counted,
and for Ki-67 index, a minimum of 500 tumor cells should
be counted in tumor hot spots. For grade-discordant cases
(based on differences in mitotic count and Ki-67 index),
the higher grade should be used.
These changes simplified the classification scheme,
however several issues remain. NECs of the pancreas are
defined by cell proliferation criteria only, however NENs
meeting the WHO criteria for NEC (described above)
with a well-differentiated morphology and an “organoid
pattern” have been identified [7, 8]. Other lesions have
components of a well differentiated NET with a low
proliferative rate, and are admixed with a high-grade
NEN within the specimen from the same patient. These
cases have been interpreted as high-grade progression
of a well differentiated NEN [9]. Heterogeneity within the
neoplasm should be noted, especially in FNA samples. The
revised version of the “WHO Classification of Tumours
of Endocrine Organs”, published in 2017, divided high
grade NENs into neuroendocrine tumor, Grade 3 (PanNET
G3) and neuroendocrine carcinomas, Grade 3 (PanNEC
G3) according to their histo-morphologic characteristics (Table 1) [10]. Tumors in the NET G3 category are associated
with a better prognosis and do not significantly respond to
cisplatin-based chemotherapy. Rb and KRAS are promising predictors of response to platinum-based chemotherapy for
NEN G3 tumors, and Rb for PanNEC (G3) [8].
The Japanese classification of pancreatic cancer, 7th
edition, was released by Japan Pancreas Society (JPS) in
July 2016 and English version of it was in 2017 [11]. In this
book, 2010 WHO grading system of NENs was adopted and
concerning to so-called “NET G3-issue” they commented
on it as “… some NETs with organoid structures may also
demonstrate a high proliferative potential (Ki67 index
>20%, mitotic count >20 per HPF). These are sometimes
called well differentiated NECs or NET G3.”
ENETS first proposed a staging system for NETs, and
this was accepted in the 7th edition of the American Joint
Committee on Cancer (AJCC)/ Union for International
Cancer Control (UICC) TNM staging manual [12]. Recently
revised AJCC/UICC system divided it each organ such as
stomach, duodenum/ampullary, jejunum/ileum, appendix,
colon and rectum [13].
Unlike in the case of digestive organ, the ENETS
recommendations and WHO 2015 classifications of lung
and thymus NENs take into account the grade of necrosis in
addition to Ki-67, and define three distinct subgroups: typical
carcinoid, atypical carcinoid (that would correspond to NET
G1 and G2, respectively) and large- and small-cell NECs [14].
Gross Findings
Grossly, NETs (well-differentiated NENs) are usually
solitary, well circumscribed, tan to pink, and relatively
homogeneous soft tumors, however they may be hard
(sclerotic) with gray-white nodules (Figure 1a), yellowish
nodules (Figure 1b) or cystic tumors. NECs (poorly
differentiated NENs) are usually tan-red or yellowish, solid masses and frequently have hemorrhagic and/or necrotic
areas.
Figure 1:Macroscopic features of pancreatic neuroendocrine tumors (NETs). (a). Gray-white and well-demarcated nodule. (b). The tumor is yellowish with a well-demarcated border.
HISTOLOGY
Well-Differentiated and Low Grade NENs (Nets G1 and
G2)
Well-differentiated NENs usually have an organoid
architecture including solid nests, trabeculae, ribbon-like,
glandular, acinar, and rosette formations, lacking necrosis, and are composed of monotonous epithelial cells with a
fair amount of cytoplasm and regular round nuclei with a
so-called “salt and pepper” appearance (Figures 2a and
2b). Most tumors have rich vascular networks. NETs in this
category have a Ki-67 index of ≤20% and ≤20 mitoses/10
HPF (Figure 2c). Vascular invasion is often found, even in
these low grade tumors (Figure 2d).
Figure 2: Histologic features of pancreatic neuroendocrine tumors (NETs). (a). The tumor has a so-called “organoid structure” including ribbonlike and pseudo- rosette patterns. (b). The tumor has a so-called “organoid structure” including trabeculae with a thin vascular network. (c). Ki-67 immunohistochemistry (WHO NET G2). (d). Vascular invasion.
Several functioning NETs show characteristic histologic
findings [2]. Stromal amyloid deposition is frequently seen in insulinomas. Glandular formation with psammomatous
calcification is sometimes noted in somatostatin-producing
tumors (Figure 3a). Approximately 10% of NETs are
accompanied with dense stromal fibrosis (Figure 3b).
These NETs are often serotonin positive and sometimes
show duct involvement.
Figure 3: Histologic variants of pancreatic neuroendocrine tumors (NETs). (a). Glandular formation with psammomatous calcification. (b). Pancreatic NET with dense stromal fibrosis. (c). Clear cell pancreatic NET. (d). Oncocytic pancreatic NET.
There are also many histo-morphologic variants
including clear cell/lipid rich, oncocytic, pleomorphic,
rhabdoid, glandular, and others. NETs with morphologically
abundant clear cytoplasm (“lipid-rich”) (Figure 3c),
grossly mimic adrenal cortical neoplasms, and are seen
especially in patients with VHL syndrome [15], but
sporadic cases have also been reported [16]. “Pigmented
black” pancreatic neuroendocrine tumors are composed
of intracytoplasmic lipofuscin and mimic metastatic
melanoma [17]. Oncocytic NETs are characterized by cells
with abundant granular eosinophilic cytoplasm because
of accumulation of mitochondria (Figure 3d) [18].
Some NETs show marked nuclear atypia/pleomorphism
throughout the tumor. Although these NETs have the
possibility of being undifferentiated carcinomas or poorly
differentiated ductal carcinomas, no elevated mitotic
rate or aggressive biology is seen [19]. Some NETs have
abundant ductal components with obvious benign cytology
[2, 19]. It is sometimes debatable whether those ductules are neoplastic glandular components of NETs or entrapped
proliferating non-neoplastic ductules. If the ductular
components have apparent histologic atypia, mixed
ductal-neuroendocrine carcinoma should be considered.
However these are exceedingly uncommon [19].
Well-Differentiated and High Grade NENs, (NET G3)
Pancreatic NET G3 lesions are defined by a Ki-
67 proliferation index >20% and/or a mitotic index
>20/10HPF and also have organoid structures as
described above (Figures 4a and 4b) [10]. The upper
limit for the proliferation index has not been defined,
however the Ki-67 index is usually less than 55%. Only
low immunohistochemical expression of p53 or loss of
Rb is observed. Due to their morphological similarity,
it is necessary to differentiate them from acinar cell
carcinomas by immunohistochemistry (Figures 4c and
4d).
Figure 4: Histologic features of pancreatic neuroendocrine tumors (NETs)(WHO PanNET G3). (a). The tumor has a glandular or acinar-like structure. (b). Ki-67 immunohistochemistry (>20%/HPF). (c). Tumor cells are partially positive for chromogranin A. (d). Tumor cells are diffusely positive for
synaptophysin.
Poorly Differentiated and High Grade NENs (NEC G3)
Poorly differentiated NECs (NEC G3) are defined by
a Ki-67 proliferation index >20% and/or a mitotic index
>20/10HPF with no differentiated morphology (organoid
structures) [10]. NECs G3 are divided into small cell NEC
and large cell NEC. Small cell NEC of the pancreas share a
similar morphology with small cell carcinoma of the lung, and it is important to rule out metastases to the pancreas
before establishing the diagnosis. NEC G3 tumors typically
have sheets or nests of carcinoma cells with pleomorphic,
hyperchromatic nuclei and abundant mitotic figures (Figure 5). The so-called "salt and pepper" chromatin
pattern is lost. Necrosis is often present in these solid
nests. Mixed tumors with exocrine differentiation are
aggressive lesions that behave more like exocrine than
endocrine carcinomas.
Figure 5: Histologic features of pancreatic neuroendocrine carcinoma (NEC)(WHO PanNEC G3).
IMMUNOHISTOCHEMISTRY
Diagnostic Markers
Well differentiated-NENs are defined by the existence
of cytoplasmic neuroendocrine granules, and the
currently accepted reliable markers are synaptophysin
and chromogranin A. Well-differentiated NENs tend
to show stronger and more diffuse staining with these
neuroendocrine markers than poorly differentiated NENs. CD56 antibody, against neural cell adhesion molecules, is
less specific as a neuroendocrine marker.
Approximately 45% of sporadic well differentiated-
NENs show loss of expression of DAXX and ATRX
immunohistochemically, which correlates with
mutations in the DAXX and ATRX genes [20, 21].
Immunohistochemically detected peptides do not imply
that the patient has clinical symptoms, and the opposite
situation may occur, probably due to the rapid release and
dispersal of the hormone product without intracytoplasmic
accumulation [2].
Prognostic or Therapy Related Markers
The mitotic count and the Ki-67/MIB-1-labeling
index are the most reliable prognostic markers for NENs.
Cytokeratin 19 (CK 19) is usually regarded as a marker
of ductal epithelial cells and is expressed not only by
poorly differentiated but also by well-differentiated NENs.
Several studies reported that CK 19 is a marker of more
aggressive behavior [22, 23, 24]. c-Kit has also reported
as a worse prognostic marker [22, 24]. There are several
other prognostic markers which were previously reported
such as CD99, CD44, p27, epidermal growth factor (EGF),
hepatocyte growth factor receptors (HGFR), E-cadherin,
CEACAM1, HER-2 and c-MET. However, they have not been
validated in clinical use [22, 25, 26, 27, 28].
Somatostatin, which binds to a family of five G-proteincoupled
receptors, was identified as an important inhibitory
hormone. The expression of somatostatin receptors
(SSTRs) in NETs, as shown by octreotide scintigraphy
and immunocytochemistry, led to the application of this
inhibitor in the treatment of patients with NETs [29]. The
development of long-acting somatostatin analogs allowed
for clinical use because the native somatostatin has a very
short half-life of only 2 minutes. SSTR2 is expressed by most
pancreatic NETs and shows high affinity for somatostatin
analogs. It has been used as a target for molecular imaging
and treatment of NETs [29]. Immunohistochemistry for
SSTR2A is widely performed.
Differential Diagnosis
The histologic differential diagnosis of pancreatic NETs
includes pancreatic neoplasms showing solid or diffuse
cellular proliferation as well as metastatic neoplasms.
Furthermore, it is not always easy to distinguish a NET
G3 from NEC G3 tumors by morphology only. Tang et al.
proposed a diagnostic algorithm for high-grade NENs using
a combination of histology and immunohistochemistry for7
DAXX/ATRX, Rb and p53 [5].
In primary pancreatic neoplasms, acinar cell carcinoma
(ACC) should first be ruled out because their radiologic/
macroscopic and microscopic morphology resembles
NETs. It is practically difficult to differentiate between a
high-grade NET (NET G3) and ACC only by morphology.
A panel of immunohistochemical stains including both
neuroendocrine and acinar cell markers (trypsin and
BCL10) can help to distinguish these lesions.
Solid pseudopapillary neoplasms (SPNs), showing solid
sheet-like, nest and sometimes a rosette-like appearance,
also resemble NETs. Immunohistochemical nuclear
staining of beta-catenin is very useful to diagnose it as a
SPN. Distinguishing from a mixed acinar-neuroendocrine
carcinoma may be challenging.
Metastatic clear cell carcinomas, known as one of the
most frequent tumors to metastasize only to the pancreas,
resemble the clear cell or lipid-rich variant of NET. The
oncocytic variant of NET may resemble hepatocellular
carcinoma.
Prognosis
Surgical complete resection of the tumor is an only
curative treatment for low grade NETs (NET G1 or G2).
If untreated, most pancreatic NETs grow and eventually
metastasize to the liver. Recently, several treatment options
in the setting of metastatic disease have been developed,
which include systemic treatment with somatostatin
analogs (SSAs), interferon-α (INF-α), peptide receptor
radiotargeted therapy (PRRT), cytotoxic chemotherapy or
molecular target agents such as everolimus and sunitinib
[30, 31].
Most PNETs are indolent but have malignant potential.
Overall 10-year survival of the patients with low grade
NENs (NET G1 or G2) is 60-70%, and with both low grade
(G1) and low stage (T1N0M0) is more than 95% [19].
Overall 5-year survival of the patients with NET G2, G3 and
NEC G3 is 61%, 22%, and 17%, respectively [19].
CONCLUSION
The WHO classification published in 2010 had a
significant impact on the classification and grading of
pancreatic NENs. However, a number of issues remain.
The revised version of the WHO classification published
in 2017 proposed grading criteria based on both
cell proliferation and morphology. Better strategies,
depending on appropriate pathological evaluation, to treat
and improve the outcomes of the patients with pancreatic
NENs are required.
Acknowledgements
We thank Professor Alan Lefor, The Center for Graduate
Medical Education, Jichi Medical University, for comments
that greatly improved the manuscript.
Conflict of Interest
All authors declare having no conflict of interests.
References
- Bosman FT, Carneiro F, Hruban RH, Theise ND (eds): WHO Classification of Tumours of the Digestive System (Eds:) 4th Edition, IARC Press, Lyons France, 2010.
- Hruban RH, Pitman MB, Klimstra DS. Tumors of the Pancreas (Afip Atlas of Tumor Pathology; 4th Series Fascicle 6) American Registry of Pathology2007.
- Ito T, Igarashi H, Nakamura K, Sasano H, Okusaka T, Takano K, et al.Epidemiological trends of pancreatic and gastrointestinal neuroendocrine tumors in Japan: a nationwide survey analysis. J Gastroenterol 2015; 50:58-64. [PMID: 24499825].
- Boyar Cetinkaya R, Aagnes B, Thiis-Evensen E, Tretli S, Bergestuen DS, Hansen S. Trends in Incidence of Neuroendocrine Neoplasms in Norway: A Report of 16,075 Cases from 1993 through 2010; Neuroendocrinology 2017;104:1-10. [PMID: 26562558].
- DeLellis RA, Lloyd RV, Heitz PU, Eng C (eds): WHO Classification of Tumours; Pathology and Genetics of Tumours of Endocrine Organs. 3rd edition, IARC Press, Lyons France, 2004.
- Klöppel G, Couvelard A, Perren A, Komminoth P, McNicol AM, Nilsson O, et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: towards a standardized approach to the diagnosis of gastroenteropancreatic neuroendocrine tumors and their prognostic stratification. Neuroendocrinology 2009;90:162-6. [PMID: 19060454].
- Tang LH, Basturk O, Sue JJ, Klimstra DS. A Practical Approach to the Classification of WHO Grade 3 (G3) Well-differentiated Neuroendocrine Tumor (WD-NET) and Poorly Differentiated Neuroendocrine Carcinoma (PD-NEC) of the Pancreas. Am J Surg Pathol 2016;40:1192-202. [PMID: 27259015].
- Hijioka S, Hosoda W, Matsuo K, Ueno M, Furukawa M, Yoshitomi H, et al. Rb Loss and KRAS Mutation Are Predictors of the Response to Platinum-Based Chemotherapy in Pancreatic Neuroendocrine Neoplasm with Grade 3: A Japanese Multicenter Pancreatic NEN-G3 Study. Clin Cancer Res 2017; 23:4625-4632. [PMID: 28455360].
- Rindi G, Klöppel G, Alhman H, Caplin M, Couvelard A, de Herder WW, et al. TNM staging of foregut (neuro)endocrine tumors: a consensus proposal including a grading system. Virchows Arch 2006; 449:395-401. [PMID: 16967267].
- Lloyd RV, Osamura RY, Kloppel G, Rosai j (eds): WHO Classification of Tumours of Endocrine Organs (World Health Organization Classification of Tumors) 4th Edition, IARC Press, Lyons France, 2017.
- Japan Pancreas Society: Classification of Pancreatic Carcinoma 4th English Edition, Kanehara, Tokyo, 2017.
- Leslie H. Sobin, Mary K. Gospodarowicz, Christian Wittekind (eds): TNM Classification of Malignant Tumours, 7th Edition, Wiley-Blackwell, 2011.
- James D. Brierley, Mary K. Gospodarowicz, Christian Wittekind TNM Classification of Malignant Tumours, 8th Edition, Wiley-Blackwell, 2017.
- Travis WD, Brambilla E, Burke AP, Marx A, Nicholson AG (eds): WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart, 4th Edition, IARC, 2015.
- Chetty R, Kennedy M, Ezzat S, Asa SL. Pancreatic endocrine pathology in von Hippel-Lindau disease: an expanding spectrum of lesions. Endocr Pathol 2004; 15:141-8. [PMID: 15299200].
- Nunobe S, Fukushima N, Yachida S, Shimada K, Kosuge T, Sakamoto M. Clear cell endocrine tumor of the pancreas which is not associated with von Hippel-Lindau disease: report of a case. Surg Today 2003;33:470-4.[PMID: 12768377].
- Smith AE, Levi AW, Nadasdy T, Campbell KA, Fishman EK, Hruban RH. The pigmented "black" neuroendocrine tumor of the pancreas: a question of origin. Cancer 2001;92:1984-91. [PMID: 11745274].
- Volante M, La Rosa S, Castellano I, Finzi G, Capella C, Bussolati G. Clinico-pathological features of a series of 11 oncocytic endocrine tumours of the pancreas. Virchows Arch 2006;448:545-51.[PMID: 16491376].
- Reid MD, Balci S, Saka B, Adsay NV. Neuroendocrine tumors of the pancreas: current concepts and controversies. Endocr Pathol 2014;25:65-79. [PMID: 24430597].
- Jiao Y, Shi C, Edil BH, de Wilde RF, Klimstra DS, Maitra A, et al. DAXX/ATRX, MEN1, and mTOR pathway genes are frequently altered in pancreatic neuroendocrine tumors. Science 2011;331:1199-203. [PMID: 21252315].
- Marinoni I, Kurrer AS, Vassella E, Dettmer M, Rudolph T, Banz V, et al. Loss of DAXX and ATRX are associated with chromosome instability and reduced survival of patients with pancreatic neuroendocrine tumors. Gastroenterology 2014;146:453-60 [PMID: 24148618].
- Ali A, Serra S, Asa SL, Chetty R. The predictive value of CK19 and CD99 in pancreatic endocrine tumors. Am J Surg Pathol 2006;30:1588-94. [PMID: 17122516].
- Deshpande V, Fernandez-del Castillo C, Muzikansky A, Deshpande A, Zukerberg L, Warshaw AL, et al. Cytokeratin 19 is a powerful predictor of survival in pancreatic endocrine tumors. Am J Surg Pathol 2004;28:1145-53. [PMID: 15316313].
- Han X, Zhao J, Ji Y, Xu X, Lou W. Expression of CK19 and KIT in resectable pancreatic neuroendocrine tumors. Tumour Biol 2013;34:2881-9. [PMID: 23686805].
- Peghini PL, Iwamoto M, Raffeld M, Chen YJ, Goebel SU, Serrano J, et al. Overexpression of epidermal growth factor and hepatocyte growth factor receptors in a proportion of gastrinomas correlates with aggressive growth and lower curability. Clin Cancer Res 2002;8:2273-85. [PMID: 12114431].
- Chetty R, Serra S, Asa SL. Loss of membrane localization and aberrant nuclear E-cadherin expression correlates with invasion in pancreatic endocrine tumors. Am J Surg Pathol 2008;32:413-9. [PMID: 18300809].
- Serra S, Asa SL, Bamberger AM, Wagener C, Chetty R. CEACAM1 expression in pancreatic endocrine tumors. Appl Immunohistochem Mol Morphol 2009;17:286-93. [PMID: 19349857].
- Modali SD, Parekh VI, Kebebew E, Agarwal SK. Epigenetic regulation of the lncRNA MEG3 and its target c-MET in pancreatic neuroendocrine tumors. Mol Endocrinol 2015;29:224-37. [PMID: 25565142].
- Hasegawa S, Kobayashi N, Tokuhisa M, Goto A, Takano S, Takada Y, et al. Clinical Usefulness of Somatostatin Receptor Scintigraphy in Japanese Patients with Gastroenteropancreatic Neuroendocrine Tumors. Digestion 2017;96:13-20. [PMID: 28609761].
- Raj N, Reidy-Lagunes D.: Current Clinical Trials of Targeted Agents for Well-Differentiated Neuroendocrine Tumors. Pancreas 2014;43:1185-9 [PMID: 25333401].
- Berardi R, Rinaldi S, Torniai M, Morgese F, Partelli S, Caramanti M, et al. Gastrointestinal neuroendocrine tumors: Searching the optimal treatment strategy--A literature review. Crit Rev Oncol Hematol 2016;98:264-74. [PMID: 26643525].






