Keywords
Neuropsychology; Assessment; Elderly; Nursing home; Cognitive disorder; Mood disorder
Introduction
Senior population in New Brunswick
New Brunswick’s senior population has been steadily growing. According to the 2011 census, 123 630 individual aged 65 and over were living in New Brunswick (representing 16.5% of the population) [1]. In July 2015 that percentage increased to 19.0% making New Brunswick the province with the highest proportion of persons aged 65 and over [2]. Statistics Canada predicts that over the next 20 years the New Brunswick population will age faster than the rest of Canada, and hypothesized that between 2013 and 2030, we will see a growth of over 100,000 people in the senior age group [3]. One explanation for this increment would be the aging of the baby boomer population, in which the eldest of this large generation turned 65 in 2011 [4].
Total of nursing home residents in New Brunswick (2012)
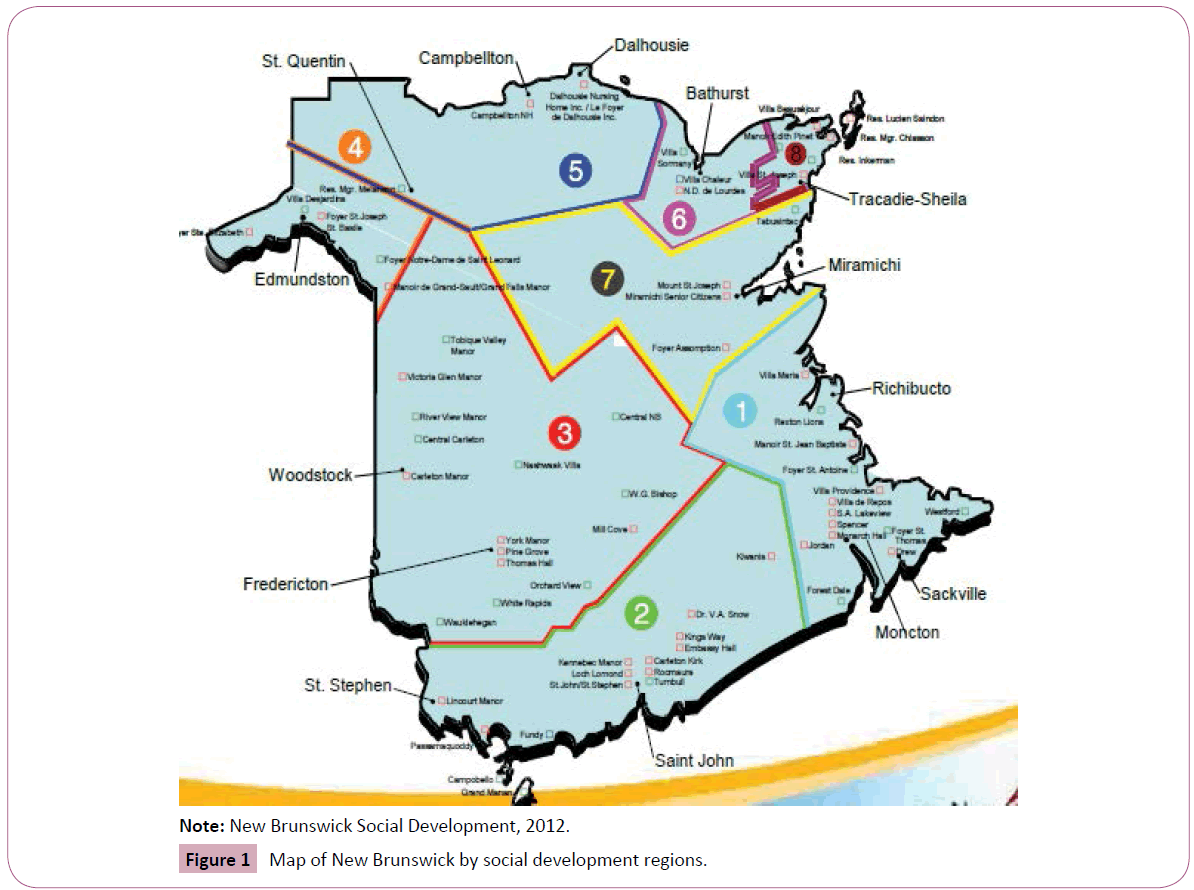
New Brunswick being home to 19.0% of its aging population (65 and over), only around 3% of the people are nursing home residents [3]. The numbers of residents vary by region (Table 1 and Figure 1), with female residents being the majority [5]. In 2012, residents between the ages of 65 and 84 represented 40.3% of the total nursing home population in New Brunswick while residents aged 85 and over represented 50.1% of this population.
| Region |
Male (n) |
% |
Female (n) |
% |
Total (n) |
| 1 |
361 |
34% |
705 |
66% |
1066 |
| 2 |
240 |
23% |
813 |
77% |
1053 |
| 3 |
260 |
30% |
596 |
70% |
856 |
| 4 |
109 |
31% |
247 |
69% |
356 |
| 5 |
67 |
36% |
120 |
64% |
187 |
| 6 |
62 |
35% |
113 |
65% |
175 |
| 7 |
91 |
31% |
198 |
69% |
289 |
| 8 |
113 |
34% |
223 |
66% |
336 |
| Total/province |
1303 |
|
3015 |
|
4318 |
Table 1: Total of nursing home residents in New Brunswick by region.
Note: New Brunswick Social Development, 2012.
Figure 1: Map of New Brunswick by social development regions.
Nursing home residents and cognitive health
The average nursing home resident in Canada can be faced with many challenges including multiple chronic diseases and problems with mobility, incontinence, and memory impairment [6]. Evidence suggests that cognitive and emotional problems can overlap with the natural aging process, making them difficult to detect [7,8]. In fact, memory loss, grief and physical decline are among factors that can blur the line between normal aging and serious psychopathology. Early evaluations of persons who are at a high risk for Mild Cognitive Impairment (MCI) and progression to dementia could be beneficial to alleviate anxiety and to identify treatable conditions that can be addressed [8] and help the advancement of treatment planning in long-term care facilities.
Mild Cognitive Impairment (MCI)
According to Gauthier et al. [9], MCI is a syndrome defined as cognitive decline greater than expected for an individual’s age/ education level, but does not interfere with daily life activities. The MCI symptoms have been classified within two categories based on a person’s thinking skill: 1) Amnestic MCI: Person starts to forget important information that they could previously easily recall (e.g., appointments, conversations, etc.), and 2) Nonamnestic MCI: Person starts to lose the ability to make a sound judgement, to complete complex tasks, etc. [10].
Epidemiological studies have shown 3% to 19% populationbased prevalence for MCI in adults older than 65 years old. Other studies have determined that more than half of people affected by MCI progress to dementia within 5 years [11,12], and that co-occurrence of affective disorder with MCI can be a risk condition for later dementia development [13]; thus, making the prodromal stage accompanied by cognitive impairment a risk state for dementia. Early detection could lead to secondary prevention by controlling risk factors [9]. Risk factors for MCI are very similar to those for dementia, which includes age, genetics, cardiovascular/cerebrovascular factors, lack of physical exercise and a poor diet [10].
People with MCI usually have problems with memory, language, thinking and judgement (notably the executive functioning deficit) [14], and this fact has been several times shown in tasks specific to assessment of memory, language, planning, organization, divided attention, and visual spatial tasks. However, people with MCI perform better at these tasks than people with dementia [15]. Of note, number of studies to date reporting on the profile of residents of long-term care facilities is limited, which warrants further documentation.
Study Goals
Our aim was to screen Mild Cognitive Impairment (MCI) in an elderly care facility in order to facilitate early identification of MCI with subsequent better management of these patients. In turn, amplify slow progression to dementia for those identified individuals. Consequently, this would allow, from a clinical perspective, to better prepare treatment and tailored protocols for nursing home residents. Thus, the objective of this study is to establish a baseline data, demographic of the included nursing home patients, in order to help looking in progression of AD in long-term care facilities.
Material and Methods
Our selection criteria consisted of: A) Residing nursing home adults with age of 65 and over, B) Capable of consenting (by reading and signing the consent) to neuropsychological assessment, and C) Willing to participate in a longitudinal study. We excluded patients with hearing and eyesight difficulties (e.g., deaf or blind individuals were excluded).
A total of 35 individuals aged 65 and over residing at York Care Centre in Fredericton and private patients of the affiliated physicians with Horizon Network were recruited to participate in this longitudinal study for an ongoing data tracking.
Subsequent to an information session, all participants signed the consent form prior to data collection and testing. The paper and pencil neuropsychological testing included the Mini Mental State Examination (MMSE) [16], the Montreal Cognitive Assessment (MoCA) [17], the Wechsler’s Digit Symbol subscale (WAIS-R, Digit symbol) [18,19], the Bell's Test [20], the Trail Making Test A and B [18,21,22], and the Geriatric Depression Scale-30 items (GDS-30) [23] to profile cognitive diagnosis, and depressive mood presentation. In addition to baseline assessment, followup assessments were conducted every 6 months for 3 years for a total of 6 assessment sessions. The duration of each assessment session was approximately 45 min and each assessment included neurocognitive testing and a chart review.
The extensively used Mini Mental State Examination (MMSE) and the Montreal Cognitive Assessment (MoCA) scales, each totalling 30 points, were used to assess the severity of global cognitive impairment. The Wechsler Adult Intelligence Scale subscale, Digit Symbol, a sensitive test for dementia differential and for objectively examining learning and memory, was used, where the total score based on the number of correct responses within the allocated time was calculated. A score of 27 or over is considered normal. The Bell's cancelation test with distractor was used to assess the extent of visuospatial inattention, where we tabulated the total number of correct responses [24]. The test requires identifying 35 bell symbols distributed on a field of other symbols and omitting of more than five bells indicate visual neglect according to the author of the test [25]; thus, a cut-off score of 32 or higher was considered as normal. The Trail Making Test A and B, tests of visual attention and task switching ability, were used to assess speed of information processing and mental flexibility by measuring task completion time [26]. The GDS-30, a well validated and extensively studied self-report depression screening scale for elderly individuals, was used to capture the extent of depressive symptoms, where higher score signify higher number of depressive symptoms [23]. Noteworthy that the choice of tools for this study is consistent with other larger scale epidemiological studies [27-29].
A qualified research assistant carried out the testing and chart review at the York Care Centre. Subsequently, the tests were scored and the data were entered into the computer software Statistical Package for Social Science (SPSS) for statistical descriptive and group comparison analysis. All data were stored electronically in a secure computer with a password-protected account. The electronic folders were password-protected and were coded in order to preserve the anonymity of the study participants. With regards to paper copies of the data, they were stored in a locked cabinet in the Cognitive Neuropsychology Laboratory of the Université de Moncton.
The current study had no intervention component; however, based on cognitive testing scores, should the participants require additional support; their family physician referred them to appropriate referral services and/or local community agencies. The family physician may have decided to refer participants to a geriatrician or another health care professional, as they deemed necessary as part of the participants ongoing care. However, these additional services were not affiliated with the current study.
Results
Our study included 35 residents of the York Care Centre (25 females and 10 males). The mean age of the sample was 84.89 years (SD=8.36), where mean age for women was 84.84 years (SD=8.36) and for men was 85 years (SD=5.25). There were 4 women out of the 35 patients who were considered to be mildly depressed. Medication types, cognitive diagnoses, and chronic diseases varied within the sample (Table 2). Length of stay at the nursing home for nearly 50% of the participant was under 12 months, where 30% were under 24 months, and the remaining were residents for over 2 years.
| |
Mildly depressive |
Non-depressive |
Total % |
| Medication types |
| SSRI |
2 |
11 |
38.2% |
| Antipsychotic |
3 |
4 |
20.6% |
| Mood stabilizer |
1 |
0 |
2.9% |
| Benzodiazepine |
1 |
4 |
14.7% |
| Alzheimer Medication |
0 |
6 |
17.6% |
| Cholinesterase inhibitor |
0 |
7 |
20.6% |
| Memantine (Ebixa) |
0 |
1 |
2.9% |
| Diagnostics |
| Alzheimer |
0 |
6 |
17.6% |
| Mixed dementia |
0 |
2 |
5.9% |
| Other dementia |
1 |
1 |
5.9% |
| Unspecified dementia |
0 |
7 |
20.6% |
| MCI |
0 |
5 |
14.7% |
| Chronic diseases |
| Diabetes mellitus |
3 |
7 |
29.4% |
| Hypertension |
2 |
13 |
44.1% |
| Arthritis |
2 |
17 |
55.9% |
| Osteoporosis |
1 |
11 |
35.3% |
| Hypothyroidism |
1 |
8 |
26.5% |
| Allergies |
3 |
10 |
38.2% |
| Gastrointestinal disease |
0 |
11 |
32.4% |
| MCI: Mild Cognitive Impairment; SSRI: Serotonin Selective Reuptake Inhibitor |
Table 2: Patients’ medication, cognitive diagnosis, and chronic disease profile.
Table 2 shows that a large proportion of individuals in our study were taking SSRI medications (38.2%), followed by antipsychotics and explicitly cholinesterase inhibitors (20.6%), and third, unspecified Alzheimer’s disease medication (17.6%). Of note, in comparison to mildly depressed, a large portion of non-depressive were taking SSRIs (2 vs. 11); this trend was also observed for cholinesterase inhibitors (0 vs. 7), Alzheimer medication (0 vs. 6), benzodiazepine (1 vs. 4), and antipsychotic (3 vs. 4). Our assessment shows that, based on cognitive performance, majority of individuals suffered from Alzheimer’s disease (17.6%) followed by MCI (14.7%), yet 20.6% of individuals were reported to have an unspecified dementia. Within the chronic disease category, majority of individuals reported to have arthritis (55.9%), followed by hypertension (44.1%), and allergies (38.2%).
Table 3 shows the cognitive and affective presentation of the sample. For global cognition, total mean score, or by sex, for both MMSE and MoCA was below normal cut-off score (<26 for MoCA, and <23 for MMSE) for the sample [30,31]. With both MMSE and MoCA we have observed individuals with mean global cognitive total score within the moderate to severe dementia state, and individuals with near flawless to perfect global cognitive score. The mean total digit symbol scores for both sex and total sample were below normal (<27) suggesting memory and encoding deficit, in other words, learning insufficiency consistent with cognitive impairment. The average score of the participants on Bell’s test was lower than the cut-off score we have set, thus suggesting of visual perception deficit. On Digit symbol, both male and female participants underperformed compared to agematched norms, on matching symbols [18]. Overall, there seem to be a trend for males to score higher than females on cognitive tests, with exception to Trail making test B. Also, there seem to be no significant difference between sexes on test of Trail making A (Table 3).
| |
Total MMSE |
Total MoCA |
Total Digit Symbol |
Score Bell’s Test |
TM A (s) |
TM B (s) |
Total GDS-30 |
| Women (n=25) |
Mean
S.D.
Max
Min |
24.94
4.26
30
15 |
18.74
6.0
29
5 |
16.64
9.72
37
0 |
25.24
9.05
35
3 |
155.28
100.58
391
38 |
371.33
254.66
1133
0 |
5.97
3.53
18
0 |
| Men (n=10) |
Mean
S.D.
Max
Min |
23.7
4.72
30
15 |
17.5
4.93
23
7 |
13.67
9.39
33
2 |
21.0
12.14
33
3 |
159.4
101.25
390
40 |
433.5
195.61
797
174 |
4.7
2.21
8
1 |
| Total participants (n=35) |
Mean
S.D.
Max
Min |
24.94
4.26
30
15 |
18.74
6.0
29
5 |
16.64
9.72
37
0 |
25.24
9.05
35
3 |
156.46
99.29
391
38 |
- |
5.97
3.53
18
0 |
| Cohen’s d (groups) |
0.28 |
0.23 |
0.31 |
0.39 |
0.04 |
0.27 |
0.43 |
| GDS: Geriatric Depression Scale; Min: Minimum; Max: Maximum; MMSE: Mini Mental State Examination; MoCA: The Montreal Cognitive Assessment Scale; SD: Standard Deviation; TM: Trailmaking Test |
Table 3: Cognitive assessment scores divided by sex and global score.
The total mean GDS score for the sample as well as by sex was within the normal range (0 to 9). However, there were individuals presenting with elevated depressive symptoms (e.g., 18 out of 30) and those that did not present with any depressive symptom [23]. Also, the mean total score for the sample and by sex for individuals aged between 65 and up, with dementia or without, were below the demographically corrected norms (<6.00, SD 4) [32].
Discussion
Findings
We found that our nursing home sample (n=35) was relatively older (mean age: 84.89, SD: 8.36), had more female, had mild to moderate cognitive impairment consistent with dementia, and that patients were stabilized for mood symptoms. The fact that we did not see much depressive symptoms, to our surprise, could be of multiple folds: A) We used an objective measure to capture depressive symptoms, and patients with dementia may have had anosognosia (that we did not control for) [33], thus limiting recognition and eventual reporting of depressive symptoms; B) In contrast to what is reported in the literature for resident of nursing homes in the first year of stay showing high prevalence for depressive symptoms [34], these patients did not because they were better treated for mood related symptoms; C) The duration of stay at our residence was variously reported. However, our result is consistent with other studies reporting baseline data [35,36] and specifically on chronic illness (e.g., arthritis) [37].
Of note, it is important to acknowledge our sample size limitation; however, this sample inform us on a unique population because participants come mainly from rural settings that is different from larger urban settings, and that we examine nursing home placement in a specific health service delivery system through primary care, with limited resources. Indeed, this baseline data set gives a better overview of the needs of frail elderly from rural settings and helps to develop better treatment plans. In addition, this type of information is important for planning purposes of health service delivery systems in rural settings.
Additional shortcoming of our study includes the lack of examination for neurophysiological factors, such as chronic neurological disease or respiratory trouble prevalent to old age, and that we did not control for the correlation between environmental factors, physical activity, and sleep, where a recent study have shown promising results [27].
Our study is unique in that we are reporting results from a battery of neuropsychological tests that is more than just using the MMSE or MoCA screeners’ scores. Other important findings are specific to treatment, as they tend to affect cognitive profile, something that we did not control for at this stage of the study. Majority of our participants were taking antidepressant or medication for Alzheimer symptoms. Additionally, our participants reported to have chronic illness including arthritis, hypertension, and allergies. This finding seems to be consistent with the evidence showing the synergistic relationship between depression and chronic physical health conditions in community sample leading to disability [38]; although our sample were treated for mood symptoms, chronic illness whether resulting from depressive mood or due to other reasons, were present at large.
Limitations
We did not control for the level of education and age of the individuals on the objective neurocognitive measures. Also, we did not examine for gender differences, whether by scales sensitivity or within our sample. However, the Bell test is sex and age insensitive [20]; yet, we observed a slight difference between sexes on mean depressive symptoms. However, these limitations are normal given the small sample size we had.
We did not examine for group differences between mildly depressive and non-depressive in terms of medication type, diagnosis, or chronic disease frequency. Also, we did not examine the difference between mildly depressive and non-depressive or within sexes in terms of neurocognitive and depressive symptoms. Additionally, another factor that we did not consider was the effect of depressive symptoms on neurocognitive performance. It is possible that those showing with elevated depressive symptoms beyond GDS’s cut-off score (although few) may have performed sub-optimally on cognitive tests and thus skewed our results, or that they had higher level of anosognosia. Future studies, incorporating collateral information from proxy on depressive and neuropsychiatric symptoms would be required.
We can’t say whether the Bell’s test utility was justified here, as it was originally developed for stroke patients; but further assessment of the accuracy of this test in differentiating patients with cerebrovascular versus those without would have added strength to our study, something that we have missed. Nonetheless, this could be indicative of specific function.
Future Direction
With regards to medication categorization, further expansion of categories would have been interesting, which was omitted in this study. Breaking down the SSRI category or any of the medication categories would have helped in an improved understanding of depressive symptoms presentation and management within neurocognitive deficit; however, this was not possible given the low sample size.
A thorough examination of the cognitive diagnosis would be essential in future studies, or as we follow the trajectory of these patients, to better classify individuals within diagnostic categories, since we did not control for AD subtypes (probable and possible), which could have been confounded with other dementia subtypes.
Classification of chronic disease to categories would be essential in future studies in order to better understand the possible underlying correlation between dementia and metabolic/ immune-related or neuroinflammatory conditions (e.g., diabetes mellitus, osteoporosis, allergies) or vascular in nature (e.g., hypertension).
Examination of neuropsychiatric symptoms, which we did not do here, would be essential in the future studies. This assessment would have disentangled intake of medication for other than psychiatric preseasons. Also, this would have raised further information about the putative synergistic effect of multiple conditions including dementia, depression, and diabetes on cognitive functioning and disease progression [39].
A limitation, not specific to our study design, was that we could not control for mortality rate at this stage of the project; which should be taken into account at later stages.
Conclusion
Our study suggests that prevention or slowing of cognitive decline at nursing home is possible; although, not without difficulty. Our study at this stage has certain limitations, such that we did not control for the effect of demographic factor on test scores, and that we did not examine for group differences between mildly depressive and non-depressive. However, our study is not without strength, in that we have included a battery of neuropsychological tests as opposed to a screening tool for the assessment of global cognitive functioning. In future studies, and follow-up to this stage, we must take into consideration: A) The mortality rate, B) The effect of medication on cognitive performance and affect and their impact at early prevention or slowing of dementia, and C) Consistent with the McKhann et al. for dementia criteria [40], the effect of chronic illness and neuropsychiatric syndromes on dementia presentation and progression. These factors would help in better understanding and care delivery to nursing home residents. Additionally, the amalgam resulting from this study would allow development of policy for better service delivery, optimal and potentially individualized treatment leading to an eventual increase in quality of life in elderly residing in nursing homes.
Acknowledgment
This research has been funded by the New-Brunswick Health Research Foundation (NBHRF). AAS was supported by the CCNA/ ASC for his postdoctoral training. Authors thank York Manor Centre in Fredericton for the support to this project and declare no potential conflict of interest.
References
- https://www12.statcan.gc.ca/census-recensement/2011/as-sa/fogs-spg/index-eng.cfm
- https://www.statcan.gc.ca/daily-quotidien/150929/dq150929b-eng.htm
- https://www2.gnb.ca/content/gnb/en/news/news_release.2012.12.1203.html
- https://www2.gnb.ca/content/gnb/en/departments/post-secondary_education_training_and_labour/promo/PopulationGrowthStrategy.html
- https://www2.gnb.ca/content/dam/gnb/Departments/sd-ds/pdf/StatisticalReports/NursingHomes/NursingHomes11-e.pdf
- Canadian Institute for Health Information (2013) When a nursing home is home: how do Canadian nursing homes measure up on quality? Canadian Institute for Health Information (CIHI) p: 34.
- Leyhe T, Reynolds CF, Melcher T, Linnemann C, Kloppel S, et al. (2016) A common challenge in older adults: Classification, overlap, and therapy of depression and dementia. Alzheimers Dement 13: 59-71.
- DiLoreto DA, Rao NA (2001) Solitary nonreactive choroidal tuberculoma in a patient with acquired immune deficiency syndrome. Am J Ophthalmol 131: 138-140.
- Gauthier S, Reisberg B, Zaudig M, Petersen RC, Ritchie K, et al. (2006) International Psychogeriatric Association Expert Conference on mild cognitive impairment. Lancet 367: 1262-1270.
- https://www.alz.org/dementia/mild-cognitive-impairment-mci.asp
- Gunnarsson MD, Ingelsson M, Blennow K, Basun H, Lannfelt L, et al. (2016) High tau levels in cerebrospinal fluid predict nursing home placement and rapid progression in Alzheimer's disease. Alzheimers Res Ther 8: 22.
- Kantarci K, Weigand SD, Przybelski SA, Shiung MM, Whitwell JL, et al. (2009) Risk of dementia in MCI: combined effect of cerebrovascular disease, volumetric MRI, and 1H MRS. Neurology 72: 1519-1525.
- Richard E, Reitz C, Honig LH, Schupf N, Tang MX, et al. (2013) Late-life depression, mild cognitive impairment, and dementia. JAMA Neurol 70: 374-382.
- https://www.alzheimer.ca/en/About-dementia/Dementias/Mild-Cognitive-Impairment
- Farias ST, Mungas D, Reed BR, Harvey D, Cahn-Weiner D, et al. (2006) MCI is associated with deficits in everyday functioning. Alzheimer Dis Assoc Disord 20: 217-223.
- Folstein MF, Folstein SE, McHugh PR (1975) "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12: 189-198.
- Nasreddine ZS, Phillips NA, Bedirian V, Charbonneau S, Whitehead V, et al. (2005) The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 53: 695-699.
- Lezak MD, Howieson DB, Bigler ED, Tranel D (2012) Neuropsychological assessment (5th edn.).
- Ashendorf L, Swenson R, Libon D (2013) The Boston process approach to neuropsychological assessment. A Practitioner's Guide.
- Gauthier L, Dehaut F, Joanette Y (1989) The Bells test: A quantitative and qualitative test for visual neglect. Int J Clin Neuropsychol 11: 49-54.
- Reitan RM (1958) Validity of the Trail Making Test as an indicator of organic brain damage. Perceptual and Motor Skills 8: 271-276.
- Corrigan JD, Hinkeldey NS (1987) Relationships between Parts A and B of the Trail Making Test. J Clin Psychol 43: 402-409.
- Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, et al. (1982) Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res 17: 37-49.
- Oliveira DC, Luara DF, Karina C, Rochele P (2016) Use of Bells Test in the evaluation of the hemineglect post unilateral stroke. J Neurol Neurosci 7: 1-8.
- Rorden C, Karnath HO (2010) A simple measure of neglect severity. Neuropsychologia 48: 2758-2763.
- Strauss E, Sherman EMS, Spreen O (2006) A compendium of neuropsychological tests: administration, norms, and commentary (3rd edn.). Oxford University, NY, USA.
- Sosso FAE, Raouafi S (2016) Appropriate sleep duration and physical activity modulate cognitive improvement. J Sleep Disor Treat Care 5: 1-5.
- Sosso FAE, Raouaf S (2016) Brain disorders: correlation between cognitive impairment and complex combination. Ment Health Fam Med 12: 215-222.
- Sosso FAE (2017) Neurocognitive game between risk factors, sleep and suicidal behaviour. Sleep Sci 10: 41-46.
- Nasreddine ZS, Phillips N, Chertkow H (2012) Normative data for the Montreal cognitive assessment (MoCA) in a population-based sample. Neurology 78: 765-766.
- Mungas D (1991) In-office mental status testing: a practical guide. Geriatrics 46: 54-58.
- Tuokko H, Hadjistavropoulos T (1998) An assessment guide to geriatric neuropsychology. Mahwah, NJ, USA.
- Davison TE, McCabe MP, Mellor D, Ski C, George K, et al. (2007) The prevalence and recognition of major depression among low-level aged care residents with and without cognitive impairment. Aging Ment Health 11: 82-88.
- Hoover DR, Siegel M, Lucas J, Kalay E, Gaboda D, et al. (2010) Depression in the first year of stay for elderly long-term nursing home residents in the USA. Int Psychogeriatr 22: 1161-1171.
- Estabrooks CA, Poss JW, Squires JE, Teare GF, Morgan DG, et al. (2013) A profile of residents in prairie nursing homes. Can J Aging 32: 223-231.
- Erber JT, Dye CJ (1982) A profile of the newly-admitted nursing home resident. Int J Aging Hum Dev 15: 307-313.
- Davison TE, McCabe MP, Knight T, Mellor D (2012) Biopsychosocial factors related to depression in aged care residents. J Affect Disord 142: 290-296.
- Deschenes SS, Burns RJ, Schmitz N (2015) Associations between depression, chronic physical health conditions, and disability in a community sample: A focus on the persistence of depression. J Affect Disord 179: 6-13.
- JuaÃŒÂÂÂÂrez-Cedillo T, Sanchez-Arenas R, Hsiung GYR, Sepehry AA, Beattie BL, et al. (2014) Effects of diabetes and depression on cognitive function in patients with dementia due to Alzheimer’s disease, vascular disease or mixed dementia (3D study). J Alzheimers Dis Parkinsonism.
- McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR, et al. (2011) The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 7: 263-269.

