Sreelatha Reddy*
GenenPlus, 640 E Ryan Rd, Oak Creek WI, USA
*Corresponding Author:
Sreelatha Reddy
GenenPlus, 640 E Ryan Rd
Oak Creek WI, USA
Tel: +414-418-2085
E-mail: contact@genenplus.com
Received date: October 25, 2015; Accepted date: November 09, 2015; Published date: November 20, 2015
Citation: Reddy S. MyTREC® RealTime qPCR Assay Reagent Kit for Quantification of Human T-Cell Receptor Excision Circles (TRECs). J Clin Epigenet. 2016, 1:1. DOI: 10.21767/2472-1158.100004
Copyright: © 2016 Reddy S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
MyTREC® RealTime qPCR Assay Reagent Kit
MyTREC® is a RealTime qPCR Assay Reagent Kit for quantification of Human T-Cell Receptor Excision Circles (TRECs).
Features of MyTREC® kit
1. All-In-One, Ready-To-Use RealTime qPCR Assay Reagent Kit
2. TaqMan® Probes for sensitive and accurate detection
3. Standard qPCR cycling conditions
4. Broad dynamic range of the calibrators for reliable testing of precious samples
5. qPCR Master Mix is available with (high/low ROX™) or without ROX™ to make it compatible for use with most of the RealTime PCR Instruments.
What is TREC?
TREC is a specific marker of T cells of thymic origin and thymic function can be determined by quantitative analysis of TRECs. TRECs are extra chromosomal DNA byproducts of T-Cell Receptor (TCR) rearrangement and “TCR delta deletion TREC” has been shown to be the most accurate TREC for measuring thymic output. MyTREC® Assay specifically measures “TCR delta deletion TREC” using quantitative, RealTime PCR [1-3].
Applications of TREC Assay
Quantitative TREC analysis has a demonstrated clinical validity in:
6. Detection of Severe Combined Immunodeficiency (SCID) in newborns. SCID is the most severe and fatal variant of Primary Immunodeficiency diseases [4]. TREC Assay is also referred to as SCID Assay / test.
7. Detection of T cell lymphopenia [4].
8. Determination of thymic output/immune reconstitution following. Hematopoietic Stem Cell Transplantation (HSCT), antiretroviral therapy/cancer vaccines, thymic transplants [1,5,6].
9. Evaluating immune competence in patients with primary immunodeficiencies, idiopathic T cell deficiencies [7].
Description
GenenPlus introduces the MyTREC® RealTime qPCR Assay Reagent Kit for highly sensitive and accurate quantification of TRECs in a blood volume as little as 1 μl. The proprietary Calibrators have been optimized to provide exceptional efficiency and sensitivity with TaqMan® dual-labeled fluorescent probes. The TRECs and β-Actin (Reference Gene) are assayed in a singleplex format on any RealTime Instrument compatible with FAM™ and VIC® reporter dyes. The Kit is provided with PCR Master Mix, containing low/high/no ROX™ dye to enable RealTime PCR Instrument compatibility. GenenPlus is also developing RNAseP as an alternative reference gene calibrator, as some end users prefer RNAseP over β-Actin.
Specification
MyTREC® Assay detects 10 genome equivalent copies per reaction (Calibrator DNA dilution).
Specimen
Dried Blood Spot (DBS) or Whole Blood EDTA.
DNA is extracted from specimens prior to conducting the PCR.
Kit Contents
Calibrators (spanning a dynamic range of 6-log10 magnitude), Primers, TaqMan® Probes (FAM™/TREC, VIC®/β-Actin), PCR Master Mix (Table 1), Positive Control, BSA, Nuclease-Free Water.
| Component |
One Rxn |
100 Rxns |
| PCR Master Mix |
10 μl |
1000 μl |
| Primer/Probe |
1 μl |
100 μl |
| BSA |
1 μl |
100 μl |
| Nuclease-Free Water |
4 μl |
400 μl |
| Volume of Rxn Mix |
16 μl |
1600 μl |
Table 1: Preparation of the reaction mix.
GenenPlus’ MyTREC® Kit versus Perkin Elmer’s Enlite™ Neonatal TREC Kit
MyTREC® Kit is a stand-alone Reagent Kit that can be used with any RealTime PCR Instrument compatible with FAM™ and VIC® dyes. Enlite™ TREC Kit requires the purchase of an Instrument (Fluorometer), WorkStation and Software along with the reagents to run the assay.
Mix gently, spin down briefly and transfer 16 μl to the well.
Add 4 μl of Calibrator DNA or Test Sample DNA, mix, seal and spin.
Always run Negative Control (Non-Template Control) and Positive Control (Positive Control DNA is provided with the Kit).
Instrumentation Compatibility
MyTREC® Assay can be performed on all RealTime PCR Instruments that are compatible with FAM™, VIC® reporter dyes.
PCR Program
The Instrument is programmed as follows (Graph 1) before setting up the qPCR reactions and run according to Instrument operator’s manual.
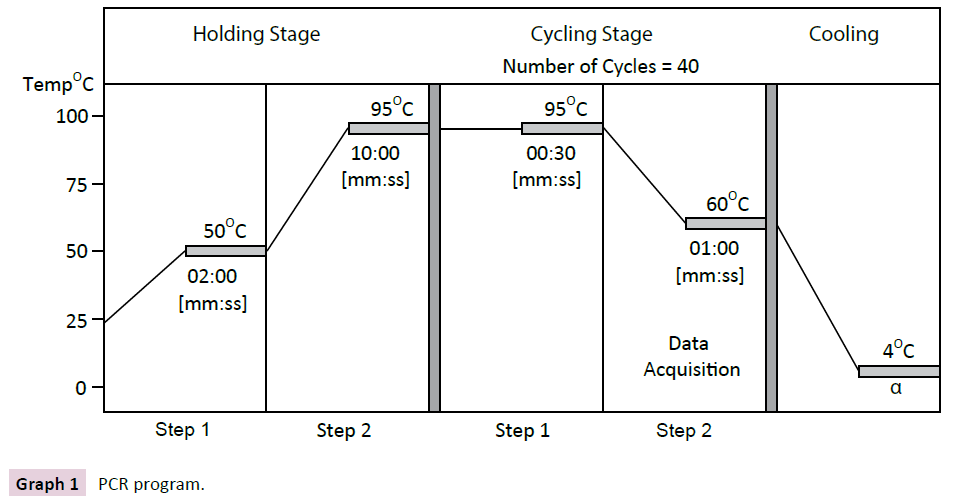
Graph 1 PCR program.
Reading and Analyzing the Results (Table 2, Graph 2 and Chart 1)
View results in the FAM™ channel (510 nm) for TREC and VIC® channel for β-Actin (β-Actin data is not shown here). Perform data analysis as described in the Instrument operator’s manual.
| Test Sample |
Positive Control |
Non-Template Control |
Result |
| No Amplification |
CT<37 |
Negative |
TREC Negative |
| Amplification CT<37 |
CT<37 |
Negative |
TREC Positive |
| No Amplification |
Not Detectable |
Negative |
PCR Failure |
| Amplification Signal |
Amplification Signal |
Positive |
PCR Contamination |
Table 2: Analyzing the data.
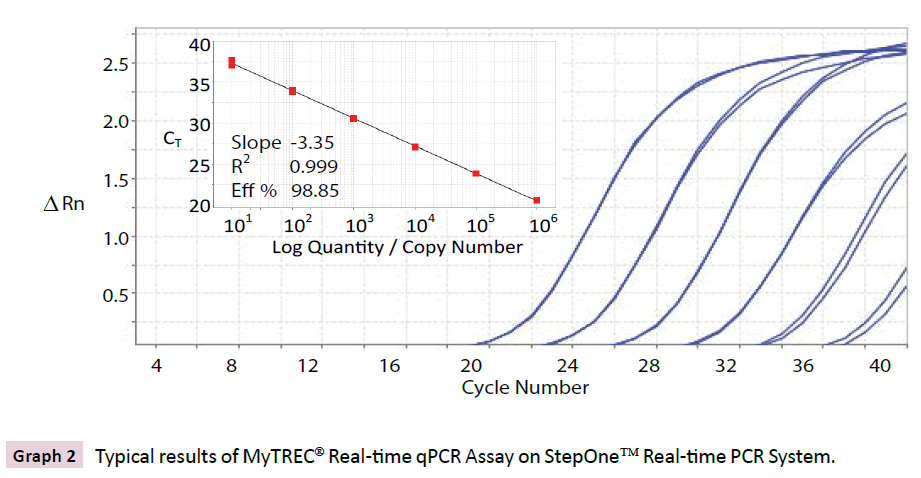
Graph 2 Typical results of MyTREC® Real-time qPCR Assay on StepOne™ Real-time PCR System.
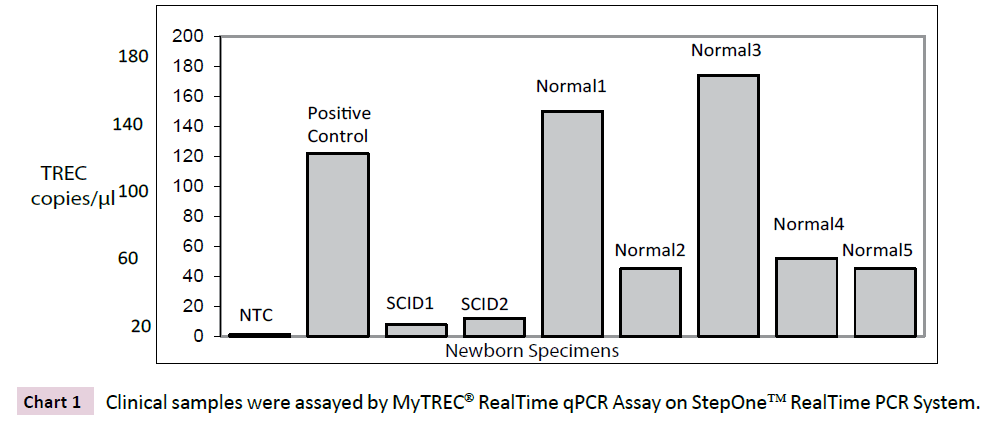
Chart 1 Clinical samples were assayed by MyTREC® RealTime qPCR Assay on StepOne™ RealTime PCR System.
MyTREC® real-time assay (Graph 2)
The Calibrators (range of 6-log10 magnitude) were amplified, in duplicate reactions with primers and TaqMan® FAM™ probe on StepOne™ RealTime PCR Instrument and data was analyzed using StepOne™ Software v2.3. Standard curve plot and linear regression statistics are shown in the inset along with the amplification plot.
Testing clinical samples using MyTREC® realtime assay (Chart 1)
De-identified newborn Dried Blood Spot specimens were processed for DNA extraction [4]. The samples were then tested in singlicate measurements on StepOne™ RealTime PCR Instrument and data was analyzed using StepOne™ Software v2.3. The SCID samples were successfully identified as SCID presumptive positive.
Disclaimer
For Research Use Only (RUO). Not intended for human therapeutic or diagnostic.
References
- Douek DC, McFarland RD, Keiser PH, et al (1998) Changes in thymic function with age andduring the treatment of HIV infection. Nature 396:690-694.
- Hazenberg MD, Verschuren MC, Hamann D, et al (2001)T cell receptor excision circles as markers for recent thymic emigrants: basic aspects, technical approach, and guidelines for interpretation. J Mol Med79:631-640.
- Spits H (2002) Development of ab T cells in the human thymus. Nat Rev Immunol 2:760-772.
- Baker MW, Grossman WJ, Laessig RH, et al (2009) Development of a routine newborn screening protocol for severe combined immunodeficiency. J Allergy ClinImmunol124:522-527.
- Borghans JA, Bredius RG, Hazenberg MD, et al (2006) Early determinants of long-term T cell reconstitution after hematopoietic stem cell transplantation for severe combined immunodeficiency. Blood108:763-769.
- Markert ML, Sarzotti M, Ozaki DA, et al (2003)Thymus transplantation in complete DiGeorge syndrome: immunologic and safety evaluations in 12 patients. Blood102:1121-1130.
- Guazzi V, Aiuti F, Mezzaroma I, et al (2002)Assessment of thymic output in common variable immunodeficiency patients by evaluation of T cell receptor excision circles: Clin Exp Immunol129:346-353.

