Keywords
Carcinoembryonic Antigen; cytology; Endoscopic
Ultrasound-Guided Fine Needle Aspiration; Pancreatic Neoplasms
Abbreviations
ERCP endoscopic retrograde cholangiopancreatography;
EUS endoscopic ultrasonography; FNA fine needle
aspiration; MP mutation profiling; SPL solid pancreaticobiliary lesion
INTRODUCTION
The current standard diagnostic modality for solid
pancreaticobiliary lesions (SPL) is an endoscopic
ultrasound (EUS) guided fine needle aspiration for
cytological evaluation. A recent meta-analysis has shown
that although cytology has a high sensitivity (85%) and
specificity (98%) for detecting malignancy in SPLs, the
negative predictive value (NPV) is only 65% [1]. It has also
been reported that despite improvement in needle devices
such as introduction of EUS needles capable of taking core
samples, and also, widespread use of on-site rapid cytology
evaluation, in a significant number of patients the cytology samples are reported indeterminate or non-diagnostic
due to limited cellularity [2]. This typically results in
further expensive testing, such as repeat sampling, delayed
diagnosis, missed diagnosis and even inappropriate
surgical intervention for confirmation of diagnosis.
Advances in molecular diagnostics have led to an
increase in available testing options for diagnosing
malignancy in SPLs. Multiple studies have shown that
mutation profiling (MP) for markers such as KRAS, MUC,
p53, p16, S100P, SMAD4 and profiling of microRNAs can
improve diagnostic sensitivity and specificity, especially
in borderline cytological cases of suspected malignancy [3, 4, 5, 6, 7, 8]. These studies examined molecular changes
in normally discarded, cell-free supernatant fluid and/or
micro-dissected cytology slides obtained by standard EUS
FNA and ERCP procedures. However, most of these studies
were exploratory and limited by small sample size, and
importantly, none of these studies demonstrated an impact
of molecular results on clinical decision making. Though
initial results are promising, further studies are needed to
demonstrate the diagnostic capabilities of MP on standard
specimens of SPLs in a larger cohort of patients in nonexploratory
clinical practice.
Our study examined the ability of MP to aid in
the diagnosis of adenocarcinoma in SPLs that were
indeterminate by cytology using standard EUS FNA and
ERCP brushing procedures. MP and indeterminate cytology
results were compared to patient outcomes derived from
surgical pathology or clinical follow-up. The ability of MP
to change clinical management recommendations and the
impact of those changes on patient outcomes were also
examined.
METHODS
Patients
Consecutive patients (>18 years of age) who had
endoscopic ultrasound fine needle aspiration (EUS FNA)
and/or endoscopic retrograde cholangio-pancreatography
(ERCP) evaluation for SPL were included in the study. All
patients included had non-diagnostic cytology results
(benign, accellular, atypical or suspicious) and MP results
at baseline testing. Subjects were excluded if i) a definitive
clinical outcome could not be determined from patient
follow-up records or patients had less than 12 months of
follow-up, ii) patients with a surgical pathology or cytology
diagnoses of neuroendocrine tumor or lymphoma or
iii) MP results were non-assessable due to insufficient
PCR-amplifiable DNA in the specimen. All baseline cytology
and MP data and follow-up patient outcomes data were
obtained from retrospective chart under IRB approval
(Quorum IRB #29760). All clinical data was entered into a
de-identified database for analysis.
Cytology
Baseline indeterminate cytology results were grouped
into two categories based on language reported. The first
category was considered ‘non-malignant’ and included:
i) ‘non-diagnostic’ cytology due to low cellularity and
ii) ‘benign’ cytology due to no or mild atypia but adequate
cells. The second category was considered ‘suspicious’ due
the presence of cells suspicious for malignancy but absence
of cells that were frankly malignant. For analysis purposes,
patients with ‘non-malignant’ cytology were considered
lower risk and patients with ‘suspicious’ cytology were
considered higher risk.
Mutation Profiling
A clinically validated panel (PancraGen™, Interpace
Diagnostic, Parsippany, NJ) was used for MP, which
included assessment for KRAS oncogene point mutations
and the presence of allelic imbalance, measured by loss
of heterozygosity mutation (LOH), at 10 genomic loci
linked to tumor suppressor genes (TSG) associated with
pancreaticobiliary cancer: 1p (CMM1, Lmyc), 3p (VHL, OGG1), 5q (MCC, APC), 9p (CDKN2A, CDKN2B), 10q (PTEN, MXI1), 17p (TP53), 17q (NME1, RNF34), 18q (DCC), 21q
(TFF1, PSEN2), and 22q (NF2) [9]. MP was performed on
specimens obtained by standard clinical EUS FNA and ERCP
procedures. Specimens analyzed included cytology slides
and cell-free supernatant fluid that is normally discarded
after cytocentrifugation of cells for cytology cell block preparation. For analysis purposes MP diagnoses were
categorized as low risk (Benign or Statistically Indolent) or
‘high risk’ (Statistically Higher Risk or Aggressive) based
on diagnostic language provided in the MP clinical report
for each patient that underwent MP testing as part of their
standard of care.
Patient Outcomes
Patient outcomes were determined from surgical
pathology, follow-up cytology indicating definitive
malignancy, or clinical follow-up (oncology records,
imaging records, clinic notes, communication with the
patients’ oncologist and/or primary care physician, or
death records). For analysis, patient outcomes were
dichotomized as ‘malignant’ or ‘benign’. Malignant
outcomes included any of the following: i) surgical
pathology results of adenocarcinoma and/or high-grade
dysplasia, ii) cytology diagnosis of malignant cells and/
or adenocarcinoma at a follow-up procedure, or iii)
pancreaticobiliary cancer diagnosis, cancer treatment, or
cancer as a cause of death in follow-up records. Benign
outcomes included any of the following: i) surgical
pathology results of negative for malignancy or dysplasia,
low-grade dysplasia, and/or intermediate-grade dysplasia
or ii) clinical follow-up without indication of malignant
diagnosis for at least 12 months after baseline testing.
Clinical Utility Assessment
All patients from the retrospective chart review
were included in a clinical utility assessment by two
clinical gastroenterologists who specialize in EUS and
ERCP procedures. Clinicians were blinded to patient
outcomes through de-identification of clinical files that
were prepared for each patient. Initially, the clinical files
contained clinical, imaging and cytology reports; MP
diagnoses and final outcomes were not included. Each
investigator separately reviewed the files of the each
patient and answered questions regarding treatment
recommendations. Two categorical questions were asked:
i) “What management course would you recommend” with
options including “No surveillance or treatment for cancer”,
“Active surveillance”, or “Treatment for cancer” and ii)
“How confident are you with this recommendation” with
options including “Very confident”, “Somewhat confident”,
or “Not at all confident”. After a one month re-blinding
period, the MP report but not patient outcomes were
included in the same clinical files, and the clinicians were
again asked to answer the same questions. For analysis,
management recommendations were categorized as
conservative (i.e. “No surveillance or treatment for cancer”
or “Active surveillance”) or aggressive (i.e. “Treatment for
cancer”). The level of confidence in each recommendation
was categorized as confident (i.e. “Somewhat confident”
or “Very confident”) or not confident (i.e. “Not at all
confident”). Management recommendations and the level
of certainty in those management recommendations were
compared before and after MP results were included in
clinical files.
Statistics
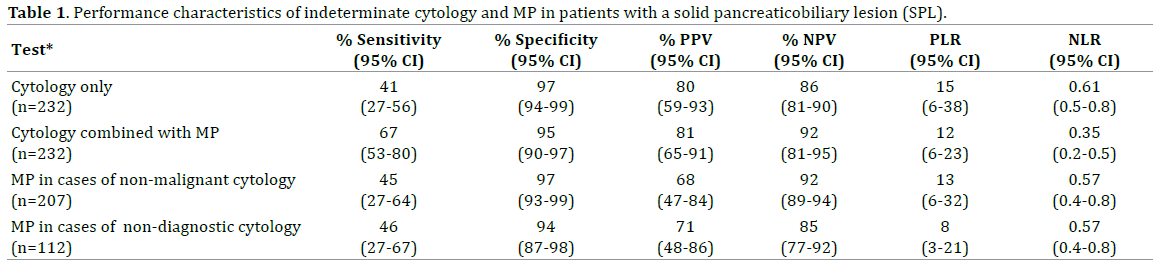
The performance characteristics of indeterminate
cytology (categorized as non-malignant or suspicious),
MP (categorized as low or high risk) and the combination
of cytology and MP (categorized as high risk if cytology
was suspicious and/or MP was high risk and low risk if
both cytology was non-malignant and MP was low risk)
were examined by 2×2 contingency table analysis. Statistical
differences in sensitivity and negative predictive value were
calculated using McNemar’s test and a weighted generalized
scoring statistic, respectively. Logistic regression analysis
was used to identify predictors of benign outcomes.
Bayes theorem was used to calculate the projected
absolute risk of malignancy based on MP results at
variable baseline probabilities of malignancy using the
performance of MP in the study cohort. Projected risk of
malignancy was examined in a hypothetical cohort of 1000
patients for each baseline probability. The absolute risk of
malignancy imparted by MP results were compared to the
baseline probability of malignancy [10]. All calculations
assumed conservation of intrinsic parameter performance
in distinct test populations. Statistical significance in the
relative risk of malignancy based on MP results compared
to baseline probability of malignancy was assessed using
Pearson’s chi-square test.
McNemar’s test was used to evaluate significant
changes in management choices (i.e. conservative vs.
aggressive treatment) and confidence level of management
recommendations (i.e. not confident vs. confident) before
and after MP results were reviewed. Logistic regression
analysis was used to assess the significant impact of MP
results on changes in management choices.
RESULTS
A total of 232 patients (44% men) with indeterminate
cytology results (i.e. non-diagnostic, benign, atypical or
suspicious) were included in the study cohort (mean age
66.9 years, SE, 0.9). Sixteen patients were excluded due to
i) non-definitive clinical outcome or less than 12 months
of follow-up (n=9), ii) neuroendocrine tumor or lymphoma
(n=2), or iii) non-assessable MP results (n=5).
The mean size of SPLs was 2.2 cm (SD, 1.1 cm). Features
of chronic pancreatitis were present upon EUS in 41 (17.7%)
patients. In 157 (67%) patients the mass was in the head
of the pancreas. Dilated main pancreatic duct in relation
to the mass was present in 47 (20%) patients, cystic solid
component in 68 (29%) patients, obstructive jaundice in 26
(11%), and abdominal pain with weight loss in 168 (73%).
Forty-nine patients (21%) had confirmed pancreaticobiliary
malignancy at a median follow-up time of 17.2 months.
At baseline testing, non-malignant cytology results
were reported in 207 (89%) patients, including 112
with non-diagnostic (i.e. accellular) cytology and 95 with
benign or atypical cells. Cytology was suspicious in only
25 patients at baseline testing. Eventually, malignancy was
confirmed in 14% of patients with non-malignant cytology (86% NPV, Table 1), occurring in 23% of those with nondiagnostic
cytology and 3% of those with benign or atypical
cells. Malignancy was confirmed in 80% of patients with
suspicious cytology (80% PPV, Table 1).
MP was performed on specimens from 218 (94%)
patients that had EUS FNA and 14 (6%) patients that
had ERCP bile duct brushings. High risk MP results were
present in 42/232 patients, including 23/25 patients that
had suspicious cytology and 19/207 patients that had
non-malignant cytology results. Low risk MP results were
present in 190/232 patients. KRAS mutation was detected
in 28/49 malignancies and TSG LOH mutation in 19/49.
Sixteen malignancies had KRAS mutation but not TSG LOH
mutation, and 7 malignancies had TSG LOH mutation but
not KRAS.
When cytology was non-malignant, MP detected 45%
of malignancies with high specificity. MP detected 46% in
the subset of non-diagnostic (i.e. accellular) cytology cases
(Table 1). Compared to use of cytology alone, the presence
of either suspicious cytology or high risk MP results
improved sensitivity (41% vs. 67%, p<0.001) and the
absence of both improved negative predictive value (86%
to 92%, p<0.05). In a logistic regression (LR) model low
risk MP results were a strong predictor of benign outcome
(29 OR, p<0.0001, Table 2).

Prior to second-line DNA analysis, first-line cytology
and imaging results triage patients into subgroups with
variable cancer probabilities. We performed sensitivity
analysis to better understand the predictive value of MP in
such scenarios using the sensitivity and specificity of MP
observed in our study cohort (Table 1). MP was useful in
distinguishing patients at higher risk of malignancy from
those at lower risk over a range of cancer probabilities
(Figure 1). Compared to the risk of malignancy
associated with non-malignant cytology (3-23%), patients
reclassified as high risk by MP were at 4-10 fold higher
risk of malignancy (30-80%, both p<0.001). Patients
reclassified as low risk by MP were at 0.4 fold lower risk
of malignancy relative to patients with non-diagnostic
cytology (9% vs. 23% risk, p=0.012) (Figure 1). Compared
to risk associated with suspicious cytology (80%), patients
reclassified as high risk by MP were at fold 1.2 fold higher
risk (98%, p<0.001) and patients reclassified as low risk
by MP were at 0.7 fold lower risk (58%, p=0.001).
Figure 1. Sensitivity analysis showing the adjusted absolute risk of malignancy given low or high risk MP results over a range of cancer probabilities.
Absolute risk of malignancy was calculated using Bayes theorem incorporating the performance characteristics of MP in all solid pancreaticobiliary lesions
(SPLs) with indeterminate cytology from the study cohort (n=232). MP mutation profile.
As part of the study we evaluated the ability of MP
to change clinician management recommendations. We
also examined the impact of those recommendations on
patient outcomes. Management recommendations made
based on cytology and imaging results for the 232 patients
in the study cohort were compared to recommendations
made based on cytology, imaging and the addition of
MP results. After viewing MP results, clinicians changed
their initial management recommendation from more
aggressive treatment for cancer to more conservative
surveillance in 10% of cases (p<0.04). Furthermore,
clinicians more frequently reported higher confidence in their recommendations after viewing MP results (98%)
compared to before (91%) (p<0.017). Mutual agreement in
management recommendations among the clinicians also
improved after viewing MP results (0.71 kappa) compared
to before (0.56 kappa).
Importantly, the average rate of benign disease
in patients recommended for more conservative
management increased from 84% to 92% after viewing MP
results (p<0.05). The average rate of malignant disease in
patients recommended for more aggressive management
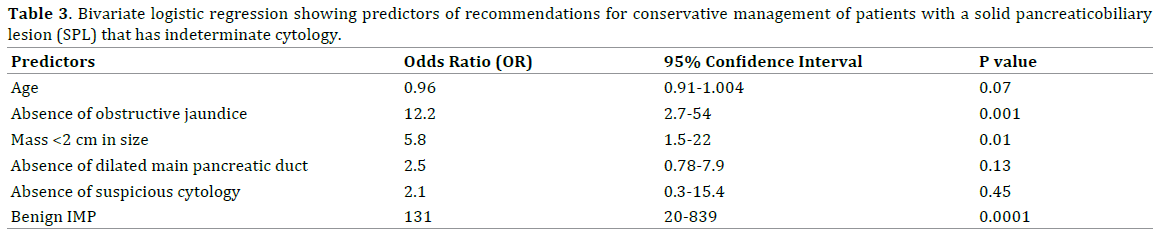
increased from 53% to 71% (p<0.05). In logistic regression
analysis, low risk MP results were strongly predictive of
recommendations for conservative management (130 OR,
p<0.0001, Table 3). The absence of obstructive jaundice
or small lesion size (<2 cm) were the only other significant
predictors of conservative management.
DISCUSSION
For solid pancreatic lesions (SPLs), early and
definitive cytological diagnosis is crucial and EUS
guided FNA has become the most common method of
obtaining a tissue diagnosis. However despite significant
advances in needle devices including the ability to take
core biopsy samples, and also, availability of ancillary
imaging technology such as contrast-enhanced EUS and
elastography, indeterminate cytology remains a common
problem. Most of the reports of high diagnostic accuracy
of EUS FNA are currently from centers of excellence,
performed by expert endosonographers and interpreted
by expert cytopathologists. However, the proportion of
indeterminate cytology samples is likely increased in
community based centers, which often do not have the
requisite expertise. Consistently, a recent review reported
that the false negative diagnostic rate for EUS FNA can
be as high as 45% in SPLs [11]. Furthermore, while fine
needle core biopsy has the ability to obtain a histological
specimen to study tissue architecture, it per se does not
improve the diagnostic yield of malignancy compared to
FNA [11, 12]. Some of the inherent biological limitations
such as paucicellular samples in a desmoplastic
stroma typically seen in pancreatic adenocarcinoma,
topographic morphological variability in a neoplastic
cellular population, and the reactive cellular atypia seen
with inflammatory lesions will always limit cytological
diagnostic accuracy. Accessibility of the lesion, the
endoscopist’s expertise in procuring a representative,
adequate sample, technician’s skill in making an optimal
smear, availability of on-site cytological assessment
and significant inter-observer disagreement between
cytopathologists are other factors that often lead to
indeterminate cytology [13].
Newer developments in sequencing technology have
led to the ability of high volume sequencing from only
small amounts of DNA. Combining MP with cytological
assessment may easily obviate the limitation of cytological
assessment and help improve its diagnostic accuracy.
Considerable published information is available on the
diagnostic utility of MP of cells from microdissected slides
and cell-free DNA from cytocentrifugation supernatant
fluid of EUS FNA and ERCP brushing procedures [7, 14].
However, these studies have been limited by small sample
size and have not examined the specific impact of these
ancillary diagnostic tests on clinical decision making.
In the current study, the combination of cytology and
MP increased overall diagnostic accuracy for malignancy
in patients with SPLs with indeterminate cytology results.
Compared to use of cytology alone, the presence of
suspicious cytology and/or high risk MP results improved
sensitivity and the absence of both improved negative
predictive value. MP was useful in distinguishing patients
at higher risk of malignancy from those at lower risk over a
range of cancer probabilities anticipated for indeterminate
cytology. However, although high risk MP results were
able to help confirm the presence of malignancy in cases in
which cytology indicated a high suspicion of malignancy,
low risk results could not effectively exclude the possibility
of malignancy in such cases.
In our study, two clinicians initially blinded to MP
results changed their management recommendation
to a more conservative plan in 10% of patients, and
these recommendations were made with a higher
level of confidence. Importantly, use of MP to aid in
decisions increased the rate of benign disease in patients
recommended for conservative management and the
rate of malignant disease in patients recommended for
aggressive management. Such improvements to patient
outcomes were obtainable from one initial diagnostic
procedure, which can lead to more general cost-effective
care.
Interestingly, availability of MP results also led to more
concordant management recommendations. Furthermore,
low risk MP results decreased the relative uncertainty
associated with conservative management. These results
are very relevant given that a recent consensus statement
by a group of expert pancreatic surgeons has reported that
up to 15% of patients undergo unnecessary pancreatic
surgery even in centers of excellence [15]. This proportion
is likely to be much higher in community practices. Given
our results, incorporation of MP testing into clinical
decision making is expected to increase a clinician’s level
of confidence in recommending conservative management
rather than aggressive and expensive surgical procedures
to compensate for clinical uncertainty.
CONCLUSION
Our study is limited by its retrospective nature. The
performance of MP in combination with cytology and its
impact on clinical decision making was based on clinical
record review of patients who had MP testing as part of
their clinical standard of care. However, the performance
of MP in combination with cytology was consistent with
that reported by others in a prospective study of solid
pancreaticobiliary lesions in which the combination of
cytology and MP also had superior diagnostic accuracy
compared to use of cytology alone [8].
Many studies have shown that pre-malignant pancreatic
lesions, such as Pan-INs, MCNs, and IPMNs, can harbor gene
mutations, including those examined by MP. However, not
all lesions are malignant. By contrast, we show that in
the context of SPLs, the mutations examined by MP were
highly specific for cancer. MP identified malignancies that
were otherwise not detected by cytology. When used in
combination, the presence of suspicious cytology and/or
high risk MP results improved sensitivity for malignancy
and the absence of both improved negative predictive
value. Furthermore, MP results significantly impacted
clinical decision making. Low risk MP results led to more
confident recommendations for conservative surveillance
with higher inter-rater agreement between clinicians. Use
of MP in combination with indeterminate cytology results
may help to more confidently and appropriately avoid unnecessary aggressive interventions, such as surgery, in
patients with SPLs.
Conflict of Interest/Funding
Interpace Diagnostic Corporation provided research
grant support to Ananya Das, MD, Arizona Center for
Digestive Health for this research study.
SAJ, NAT, JLS, CMN, SDF are employees of Interpace
Diagnostics Corporation. No other authors have conflicts
of interest to declare.
Author Contributions
Study concept and design: SAJ, NAT, JLS, SDF, CMN, AD
Acquisition of Data: All authors
Drafting of the article: AD, SAJ
Critical revision for important intellectual content: All
authors
Final approval of the article: All authors
References
- Hewitt MJ, McPhail MJ, Possamai L, Dhar A, Vlavianos P, Monahan
KJ. EUS-guided FNA for diagnosis of solid pancreatic neoplasms: a metaanalysis.
Gastrointest Endosc 2012; 75:319-331. [PMID: 22248600]
- Fisher L, Segarajasingam DS, Stewart C, Deboer WB, Yusoff IF.
Endoscopic ultrasound guided fine needle aspiration of solid pancreatic
lesions: Performance and outcomes. J Gastroenterol Hepatol 2009; 24:90-
96. [PMID: 22248600]
- Bournet B, Gayral M, Torrisani J, Selves J, Cordelier P, Buscail L. Role
of endoscopic ultrasound in the molecular diagnosis of pancreatic cancer.
World J Gastroenterol 2014; 20:10758-10768. [PMID: 25152579]
- Ryozawa S, Iwano H, Taba K, Sen-yo M, Uekitani T. Genetic diagnosis
of pancreatic cancer using specimens obtained by EUS-FNA. Dig Endosc
2011; 23 Suppl 1:43-45. [PMID: 21535200]
- Khalid A, Nodit L, Zahid M, Bauer K, Brody D, Finkelstein SD, et al.
Endoscopic ultrasound fine needle aspirate DNA analysis to differentiate
malignant and benign pancreatic masses. Am J Gastroenterol 2006;
101:2493-2500. [PMID: 17029619]
- Wang X, Gao J, Ren Y, Gu J, Du Y, Chen J, et al. Detection of KRAS gene
mutations in endoscopic ultrasound-guided fine-needle aspiration biopsy
for improving pancreatic cancer diagnosis. Am J Gastroenterol 2011;
106:2104-2111. [PMID: 21876563]
- Deftereos G, Finkelstein SD, Jackson SA, Ellsworth EM, Krishnamurti
U, Liu Y, et al. The value of mutational profiling of the cytocentrifugation
supernatant fluid from fine-needle aspiration of pancreatic solid mass
lesions. Mod Pathol 2014; 27:594-601. [PMID: 24051700]
- Gonda TA, Viterbo D, Gausman V, Kipp C, Sethi A, Poneros JM, et al.
Mutation Profile and Fluorescence In Situ Hybridization Analyses Increase
Detection of Malignancies in Biliary Strictures. Clin Gastroenterol Hepatol
2017; 15:913-919 e911. [PMID: 28017843]
- Khalid A, Zahid M, Finkelstein SD, LeBlanc JK, Kaushik N, Ahmad N,
et al. Pancreatic cyst fluid DNA analysis in evaluating pancreatic cysts:
a report of the PANDA study. Gastrointest Endosc 2009; 69:1095-1102.
[PMID: 19152896]
- Marton KI, Rudd P, Sox HC, Jr. Diagnosing pancreatic cancer-
-an analysis of several strategies. West J Med 1980; 133:19-25.
[PMID: 7222644]
- Fujii LL, Levy MJ. Pitfalls in EUS FNA. Gastrointest Endosc Clin N Am
2014; 24:125-142. [PMID: 24215764]
- Wani S, Muthusamy VR, Komanduri S. EUS-guided tissue acquisition:
an evidence-based approach (with videos). Gastrointest Endosc 2014;
80:939-959 e937. [PMID: 25434654]
- Mounzer R, Yen R, Marshall C, Sams S, Mehrotra S, Said MS, et al.
Interobserver agreement among cytopathologists in the evaluation of
pancreatic endoscopic ultrasound-guided fine needle aspiration cytology
specimens. Endosc Int Open 2016; 4:E812-819. [PMID: 27556103]
- Krishnamurti U, Sasatomi E, Swalsky PA, Finkelstein SD, Ohori NP.
Analysis of loss of heterozygosity in atypical and negative bile duct
brushing cytology specimens with malignant outcome: are "falsenegative"
cytologic findings a representation of morphologically
subtle molecular alterations? Arch Pathol Lab Med 2007; 131:74-80.
[PMID: 17227126]
- Asbun HJ, Conlon K, Fernandez-Cruz L, Friess H, Shrikhande SV, Adham
M, et al. When to perform a pancreatoduodenectomy in the absence of
positive histology? A consensus statement by the International Study Group
of Pancreatic Surgery. Surgery 2014; 155:887-892. [PMID: 24661765]


