Keywords
Pancreatectomy; Pancreatitis
Abbreviations
IPMT intraductal papillary mucinous tumor; XGI
xanthogranulomatous inflammation; XGP xanthogranulomatous
pancreatitis
INTRODUCTION
Xanthogranulomatous inflammation (XGI) is a rare
pathologic entity with characteristic macroscopic and
microscopic features [1]. XGI is destructive inflammatory
disease affected multiple organs. Most XGIs occur in the
kidney [2] and gallbladder [1, 3, 4], but the other sites such
as the breast [5], intracranium [6], gastrointestinal tract
[7, 8], genital organs [9], bone [10], and skin [11] were
reported. XGI to the pancreas, the xanthogranulomatous
pancreatitis (XGP) is an extremely rare disease. Over
the past decades, only 19 cases of xanthogranulomatous
pancreatitis were reported in the English literature [12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27].
We herein report a case of progressive XGP, where the
inflammation infiltrated into the stomach, transverse
colon and spleen.
CASE REPORT
A Twenty-three-year-old Japanese man was admitted
to our hospital for episodes of acute upper abdominal
pain. He was diagnosed with acute pancreatitis caused by
main pancreatic duct stones. The abdominal computed
tomography (CT) scan on admission showed pancreatic
stones in main pancreatic duct as well as duct dilation and
enlarged pancreas head (Figure 1a). There was no past medical history nor family history of the pancreatic disease.
He denied alcohol use. He was referred to University hospital
for extracorporeal shock wave lithotripsy (ESWL) for stone
removal followed by Endoscopic Retrograde Cholangio-
Pancreatography (ERCP) with pancreatic duct stenting.
He underwent total eight times of ESWL and pancreatic
stones in main pancreatic duct were removed (Figure 1b).
Within next two years from initial treatment, he came back
total three times with pancreatitis by radiological evident
pancreatics stones. ERCPs were performed same manner
and stones were removed (Figures 2a, 2b). However
four months after the last episode of stone pancreatitis,
he developed another pancreatitis without evidence
of stone in the main pancreatic duct. The pancreatic
pseudocysts were evident at that time, and dilation of
pancreatic duct vanished (Figure 3). The serum amylase
and pancreatic-amylase level were high as 615IU/ℓ
(standard value:43-116 IU/ℓ) and 587 IU/ℓ (18-53 IU/ℓ)
respectively. And amylase level in the urine was also
elevated as 8,604 IU/ℓ (<500 IU/ℓ). Complete blood count
(CBC) and Comprehensive metabolic panel with fasting
glucose (CMP) were within normal limits. The mutations
of all pancreatitis-associated gene CPA1 [28] was negative,
and the IgG 4 level was within normal limit. We initiated
medical treatment (pancreatin, camostat mesylate,
trimethadione, bromhexine hydrochloride, esomeprazole
magnesium hydrate) and dietary restrictions (only Elental
480g/day or fast cure). The follow up abdominal CT scan
after four months, however, showed multiple pseudocysts
at the tail of the pancreas that infiltrated into stomach,
colon, and spleen without stone at main pancreatic duct (Figure 4). Meantime his symptom had been on and off.
Six months later, follow up CT scan showed ill-defined
low-density area developed adjacent to pseudocysts
that involved the stomach, transverse colon, and spleen.
The border between pancreas and stomach became unclear (Figure 4). Esophagogastroduodenoscopy (EGD)
showed hypertrophic mucosa with poor distensibility
of the posterior gastric wall suggested inflammation
from pancreatitis, and pancreatic pseudocysts involved
stomach (Figure 5). Further restricted dietary treatment
with total parental nutrition and pain management with
NSAIDs and pentazocine hydrochloride were initiated but
failed shortly after. At that point, we finally decided to
perform a surgical intervention. Initially, our plan was to
perform distal pancreatectomy with possible splenectomy,
since we recognized the lesion was benign and attempted
to preserve as many adjacent organs as possible. However,
the whole lesion that include part of the transverse colon,
spleen and the large portion of stomach was palpate
like a solid mass and only en bloc resection appeared to
be an option. The entire posterior walls of the stomach
and transverse colon as well as spleen were severely
adhered to the pancreas. We ended up to perform distal
pancreatectomy up to superior mesenteric vein with
splenectomy, partial resection of transverse colon with
primary anastomosis and total gastrectomy with Rouxen Y reconstruction (Figure 6). Gross examination of the
specimen revealed the rupture of main pancreatic duct
led to 5.0 cm pancreas pseudocysts with the thick wall
made of dense fibrosis. The pancreas itself and pancreatic
pseudocyst infiltrated to the stomach, spleen and
transverse colon (Figure 7). Histopathologic examination
of the pancreatic tail specimen showed extensive fibrosis
and infiltration of numerous foamy histocytes with
scattered eosinophil, neutrophils, lymphocytes, plasma
cells, indicating XGI (Figure 8). The XGI lesion infiltrated
into not only the pancreas parenchyma but also adjacent
organs such as the stomach, transverse colon, and spleen.
His postoperative course was uneventful, and he was
discharged on the 22nd post-operative day. After 3 years
of follow up, he is in good health without any symptom.
Figure 1: (a). Abdominal CT at first visit to our hospital showed pancreatic stone at main pancreatic duct, main pancreatic duct (MPD) dilation, and moderate enlarged pancreas head. Asterisks indicate MPD stone, arrows indicate MPD dilation. (b). He underwent ESWL 8 times; Left panel; MPD stone obstructed MPD. Right panel; after ESWLs 8 times, pancreatic stones at MPD were completely removed.
Figure 2: (a). He has relapsed into pancreatitis after ten months of initial treatment. Left panel; MPD stones were appeared. Right panel; MPD stones were removed again. (b). After 8 months, he had a recurrence of pancreatitis. MPD stones were removed and drainage of MPD was performed. Arrows indicate MPD stone.
Figure 3: Abdominal CT after four months of treatment third pancreatitis revealed that the pancreas pseudocysts at the pancreatic tail, around of stomach and spleen without the pancreatic stone at main pancreatic duct. Dilation of pancreatic duct vanished. Asterisks indicate pseudocyst, arrows indicate.
Figure 4: (a). Follow up abdominal CT after one month showed multiple pseudocysts at the tail of the pancreas that are extended into stomach, colon, and spleen. (b, c). Ill-defined low-density area developed around pancreas and pseudocysts involved the stomach, transverse colon, and spleen. The borders between the lesion and the pancreas, stomach, transverse colon and spleen were unclear. Sharps indicate stomach. Asterisks indicate transverse colon. Arrows indicate pseudocyst.
Figure 5: Esophagogastroduodenoscopy showed hypertrophic mucosa and poor distensibility of the posterior gastric wall caused by pancreatitis and pancreatic pseudocyst.
Figure 6: Surgical figures: Pancreas firmly adhered to spleen, stomach, transverse colon and omentum. Due to extensive infiltration, we had to performed radical resection include distal pancreatectomy up to superior mesenteric vein with splenectomy, total gastrectomy with Roux-en Y reconstruction and partial resection of transverse colon with primary anastomosis.
Figure 7: Gross examination of the specimen revealed that the rupture of main pancreatic duct led to 5.0 cm pancreas pseudocysts with the thick wall made of extensive fibrosis. The pancreas and pancreatic pseudocyst adhered firmly to the stomach and transverse colon.
Figure 8: Microscopic examination revealed extensive fibrosis and infiltration of numerous foamy cells along with scattered lymphocytes and plasma cells are noted. (a). Hematoxylin and Eosin stain (HE) ×20, (b). ×100, (c). ×600. high-power view of foamy histocytes with clear lipid-containing cytoplasm. (d). Schmorl stain; Pale blue cells are foamy cells. Blue immediate iron.
DISCUSSION
We reported a twenty-three-year-old man who was
found to have an extremely rare entity, XGP complicated
by pancreas pseudocysts infiltrated into spleen, stomach,
transverse colon and omentum. Originally Goodman et al. reported that XGI is characterized by chronic mixed
inflammatory process that contains varying amounts of
foamy histiocytes, inflammatory cells, fibrous reaction and
sometimes accompanied by multinucleated giant cells [1].
The characteristic processes of XGP include destruction
and effacement of the normal structures of the affected
organ and often mimic the neoplastic process. XGI itself
is also a rare condition which has been well documented
mainly in the gallbladder [1, 3, 4] and kidney [2]. XGI
occurs in the pancreas is so rare that only 19 cases have
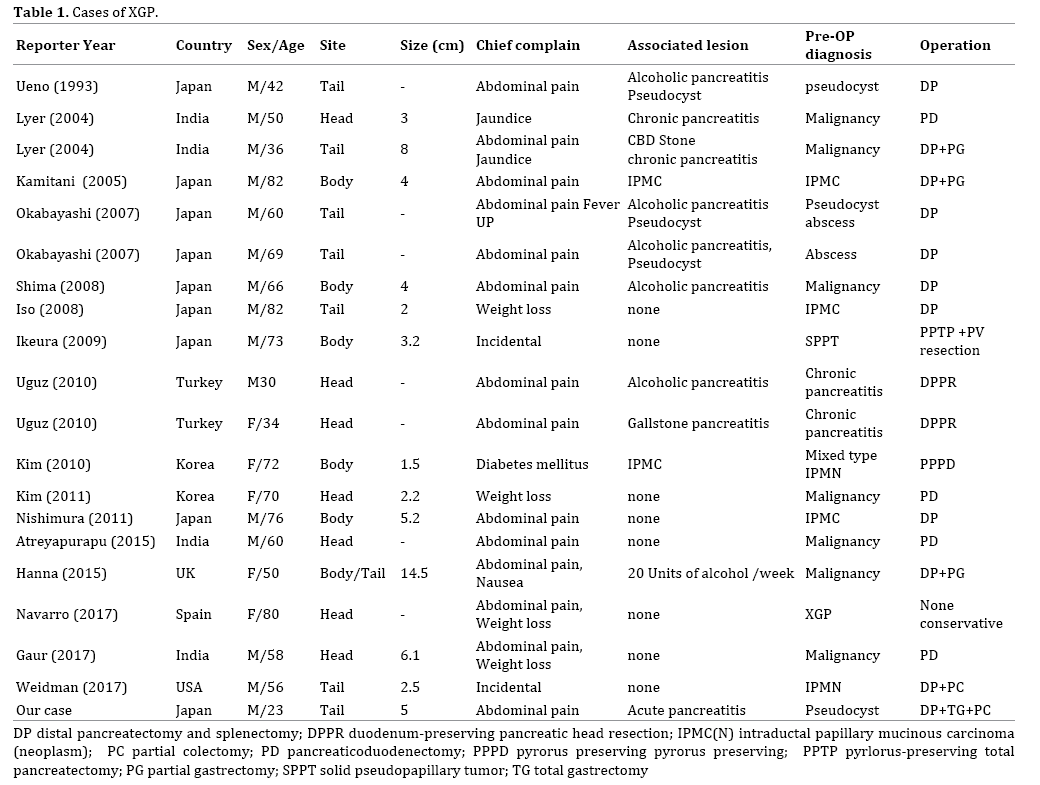
been reported in the English literature since Ueno et al. reported the first case of XGP in 1993 [12]. According to
20 case reports include our case (Table 1) [12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27], their median
age was 60 year (23-82), XGP occurs mainly in male
patients (M:F; 15:5), the locations were evenly distributed
in the pancreas (head: body: tail; 7: 6: 8). In most cases,
patients presented with symptoms such as abdominal pain
(14 cases, 68%) and weight loss (4 cases). Only 2 cases
were diagnosed by accidental findings. The majority of
cases (13/20; 65%) were misdiagnosed as a neoplasm by
preoperative imaging (13/20; 65%).
The exact etiology of XGP is unknown; duct
obstruction, infection and hemorrhage trigger such as
XGI of gallbladder and kidney. Kim et al. reported mucin produced by intraductal papillary mucinous tumor (IPMT)
increased the intraductal and intracystic pressure and
that a leakage of mucin into the pancreatic parenchyma
produced the xanthogranulomatous changes [20]. Iyer et al. suggested that obstruction to pancreatic ducts by
stones followed by secondary bacterial infection initiated
the xanthogranulomatous pancreatitis without cystic
lesion [13]. Ueno et al. reported that a pseudocyst formed
by acute alcoholic pancreatitis and, after relapse attacks,
infection and hemorrhage occurred in the pseudocyst.
That elevated intracystic pressure and caused secondary
xanthogranulomatous change to the pancreatic cyst
wall [12]. In our case, extensive pancreatic stones
caused pancreatic duct obstruction and the subsequent
development of longstanding pancreatitis, which might
cause xanthogranulomatous change in the pancreas.
Weidman et al. reported that the peculiarity of the
imaging of XGP is very helpful for proper preoperative
diagnosis [27]. Of note, all cases except one underwent
surgery due to either preoperative diagnosis as malignant
or failure of medical treatment. Although the ill-defined
lesions appeared around pseudocysts by the follow up
CT scan, we kept treating the lesion as the benign due to
the fact the patient presented as pancreatic stone induced
pancreatitis. Thus, we did not pursue further diagnostic imaging nor biopsy but we might have done endoscopic
ultrasound guided biopsy for confirmation that the lesion
was benign. Six cases included our case (6/20; 30%)
underwent surgery despite the fact that preoperative
diagnosis was benign [12, 15, 19]. In these cases of XGP, they
had had intractable abdominal pain for a long period of time
(Average 17.8 M; 1-36 M) and persisted through medical
management such as low-fat diet and pharmaceutical
management. Navarro et al. avoided surgery by making the
diagnosis through biopsy and reported the effectiveness of
medical therapy and pharmaceutical intervention [25]. In
our case, it is demonstrated that his disease overall resisted
for all various treatments such as dietary treatment
(low-fat diet), pharmacotherapy (antibiotic, proteinase
inhibitor, NSAIDs and pentazocine hydrochloride) and
endoscopic therapy (remove pancreatic calculus exploited
ESWL and drainage of the MPD) for total two years four
months period. Only surgical intervention can cut off a
chain reaction of inflammation of XGP for pancreas and
its adjacent organs. However, due to the fact that both XGI
and XGP are not neoplastic entities, there is always room
for debate regarding surgical intervention. In our case, the
intention to avoid pancreatectomy for two years four months
allows XGP to progress and end up with radical resection
include total gastrectomy. Fortunately, our case has been
making good progress after the surgery, and his lifestyle has
been improved. He drinks alcohol occasionally post operation
but no recurrence of pancreatitis for almost three years.
CONCLUSION
In summary, we report a 23-year-old man who was
found to have XGP complicated by pancreas pseudocysts
infiltrated into spleen, stomach, transverse colon and
omentum. Although we applied multidisciplinary
approach, only radical resection of the involved area
reached remission of the disease. Further knowledge is
warranted to establish the treatment strategy for this rare,
complicated pancreatitis.
Conflict of Interests
The authors declare that they have no competing
interests.
References
- Goodman ZD, Ishak KG. Xanthogranulomatous cholecystitis. Am J
Surg Pathol 1981; 5:653-9. [PMID: 7337158]
- Addison B, Zargar H, Lilic N, Merrilees D, Rice M. Analysis of 35 cases of Xanthogranulomatous pyelonephritis. ANZ J Surg 2015; 85:150-3.
[PMID: 24661744]
- Guzmán-Valdivia G. Xanthogranulomatous cholecystitis: 15 years'
experience. World J Surg 2004; 28:254-7. [PMID: 14961199]
- Han SH, Chen YL. Diagnosis and treatment of xanthogranulomatous
cholecystitis: a report of 39 cases. Cell Biochem Biophys 2012; 64:131-5.
[PMID:22707297]
- Hussain T, Elahi B, Long E, Mahapatra T, McManus PL, Kneeshaw PJ.
Xanthogranulomatous inflammation involving latissimus dorsi donor
site and implant breast reconstruction: case report and literature review.
World J Surg Oncol 2012; 10:166. [PMID: 22906098]
- Yamada H, Kurata H, Nomura K, Utsunomiya K, Shimizu M, Isogai
Y. Adult xanthogranulomatous intracranial lesion involving familial
hypercholesterolemia. Jpn J Med 1989; 28:757-61. [PMID: 2699337]
- Kubosawa H, Yano K, Oda K, Shiobara M, Ando K, Nunomura M, et al.
Xanthogranulomatousgastritis with pseudosarcomatous changes. Pathol
Int. 2007; 57:291-5. [PMID: 17493178]
- Yoon JS, Jeon YC, Kim TY, Han DS, Sohn JH, Nam KW, et al.
Xanthogranulomatous inflammation in terminal ileum presenting as an
appendiceal mass: case report and review of the literature. Clin Endosc
2013; 46:193-6. [PMID: 23614133]
- Murhekar K, Majhi U, Senthilkumar AC, Sundersingh S, Sridevi V. A
rare case of xanthogranulomatous oopharitis. J Cancer Res Ther 2014;
10:209-10. [PMID: 24762518]
- Vankalakunti M, Saikia UN, Mathew M, Kang M. Xanthogranulomatous
osteomyelitis of ulna mimicking neoplasm. World J Surg Oncol 2007 30;
5:46. [PMID: 17470270]
- Satter EK, Gendernalik SB, Galeckas KJ. Diffuse
xanthogranulomatousdermatitis and systemic Langerhans cell
histiocytosis: A novel case that demonstrates bridging between non-
Langerhans cell histiocytosis and Langerhans cell histiocytosis. J Am Acad
Dermatol 2009; 60:841-8. [PMID: 19022530]
- Ueno T, Hamanaka Y, Nishihara K, Nishida M, Nishikawa M, Kawabata
A, et al. Xanthogranulomatous change appearing in the pancreas cyst
wall. Pancreas 1993; 8:649-51. [PMID: 8302803]
- Iyer VK, Aggarwal S, Mathur M. Xanthogranulomatous pancreatitis:
mass lesion of the pancreas simulating pancreatic carcinoma--a report of
two cases. Indian J Pathol Microbiol 2004; 47:36-8. [PMID: 15471123]
- Kamitani T, Nishimiya M, Takahashi N, Shida Y, Hasuo K, Koizuka
H. Xanthogranulomatous inflammation in terminal ileum presenting as
an appendiceal mass: case report and review of the literature. AJR Am J
Roentgenol 2005; 185:704-7. [PMID: 16120922]
- Okabayashi T, Nishimori I, Kobayashi M, Sugimoto T, Kohsaki T,
Okamoto K, et al. Xanthogranulomatous pancreatic abscess secondary
to acute pancreatitis: two case reports. Hepatogastroenterology 2007;
54:1648-51. [PMID: 18019685]
- Shima Y, Saisaka Y, Furukita Y, Nishimura T, Horimi T, Nakamura T, et
al. Resected xanthogranulomatous pancreatitis. J Hepatobiliary Pancreat
Surg 2008; 15:240-2. [PMID: 18392724]
- Iso Y, Tagaya N, Kita J, Sawada T, Kubota K. Xanthogranulomatous
lesion of the pancreas mimickingpancreatic cancer. Med Sci Monit 2008;
14:CS130-3. [PMID: 18971878]
- Ikeura T, Takaoka M, Shimatani M, Koyabu M, Kusuda T, Suzuki R,
et al. Xanthogranulomatous inflammation of the peripancreatic region
mimicking pancreatic cystic neoplasm. Intern Med 2009; 48:1881-4.
[PMID: 19881238]
- Uguz A, Yakan S, Gurcu B, Yilmaz F, Ilter T, Coker A.
Xanthogranulomatous pancreatitis treated by duodenum-preserving
pancreatic head resection. Hepatobiliary Pancreat Dis Int 2010; 9:216-8.
[PMID: 20382597]
- Kim YN, Park SY, Kim YK, Moon WS. Xanthogranulomatous
pancreatitis combined with intraductal papillary mucinouscarcinoma in
situ. J Korean Med Sci 2010; 25:1814-7. [PMID: 21165301]
- Kim HS, Joo M, Chang SH, Song HY, Song TJ, Seo JW, et al.
Xanthogranulomatous pancreatitis presents as a solid tumor mass: a case
report. J Korean Med Sci 2011; 26:583-6. [PMID: 21468270]
- Nishimura M, Nishihira T, Hirose T, Ishikawa Y, Yamaoka R, Inoue
H, et al. Xanthogranulomatous pancreatitis mimicking a malignant cystic
tumor of the pancreas: report of a case. Surg Today 2011; 41:1310-3.
[PMID: 21874438]
- Atreyapurapu V, Keshwani A, Lingadakai R, Pai K.
Xanthogranulomatous pancreatitis mimicking a malignant solid tumour.
BMJ Case Rep. 2016; 30. [PMID: 27030447]
- Hanna T, Abdul-Rahman Z, Greenhalf W, Farooq A, Neoptolemos JP.
Xanthogranulomatous pancreatitis associated with a mucinous cystic
neoplam. Pathol Int 2016; 66:174-176. [PMID: 26560435]
- Navarro Navarro B, Sáez González E, Ortuño JA. Xanthogranulomatous
pancreatitis: a lesion that mimics pancreatic cancer. Rev Esp Enferm Dig
2017; 109:234. [PMID: 28190364]
- Gaur K, Mandal S, Mahajan N, Saluja S, Godhi S. Xanthogranulomatous
Pancreatitis - A Rare Case Defying Clinical, Radiological and Tumor
Marker Diagnostics with a Review of Literature. Turk Patoloji Derg 2017;
01385. [PMID: 28272682]
- Becker-Weidman D, Floré B, Mortelé KJ. Xanthogranulomatous
pancreatitis: A review of the imaging characteristics of this rare and
often misdiagnosed lesion of the pancreas. Clin Imaging 2017; 45:12-17.
[PMID: 28554050]
- Witt H, Beer S, Rosendahl J, Chen JM, Chandak GR, Masamune A, et
al. Variants in CPA1 are strongly associated with early onset chronic
pancreatitis. Nat Genet 2013; 45:1216-20. [PMID: 23955596]









