Yasuhiro Fujino1, Shingo Kanaji1, Kentaro Kawasaki1, Masahiro Tominaga1, Kazuyoshi Kajimoto2
1Department of Gastroenterological Surgery, Hyogo Cancer Center, 13-70 Kitaoji-cho, Akashi 673-6558, Japan
2Department of Gastroenterological Pathology, Hyogo Cancer Center, 13-70 Kitaoji-cho, Akashi 673-6558, Japan
- *Corresponding Author:
- Yasuhiro Fujino
Department of Gastroenterological Surgery
Hyogo Cancer Center
13-70 Kitaoji-cho
Akashi 673-6558, Japan
Phone +81-78-929-1151
Fax +81-78-929-2380
E-mail yasu120@hp.pref.hyogo.jp
Received March 04th, 2015-Accepted April 8th, 2015
Keywords
Pancreatitis; Cystadenocarcinoma
INTRODUCTION
Mucinous cystic neoplasms (MCNs) occur in the pancreas, ovarium, appendix, and other organs of the abdomen, and are generally diagnosed by ovarian like stroma [1-5]. MCNs are often associated with pseudomyxoma peritonei when they rupture [4]. As MCNs are suspected to be malignant, they are usually resected when diagnosed [1-4]. The malignancy of pancreatic MCNs is reported as 17.3 % [5]. Here, we report a male with multiple MCNs, in whom there was no finding of oncological association.
CASE REPORT
A 63-year-old male with abdominal distension was referred to our hospital. He had no symptoms including bowel habits and no other comorbidities. Physical examination showed no remarkable findings. Laboratory data, including the liver and pancreatic functions, were normal. Tumor markers, including carcinoembryonic antigen and carbohydrate antigen 19-9, were also within the normal limits. Ultrasonographic scans of the abdomen revealed two aechogenic lesions of the spleen and stomach. Computed tomography (CT) also showed a 72 mm cystic tumor of the spleen and a 58 mm cystic tumor of the stomach (Figure 1). Magnetic resonance imaging (MRI) of the abdomen revealed a 70 mm tumor of the spleen and a 52 mm tumor, which were high intensity in T1-weighted and low intensity in T2-weighted images. Endoscopy showed that the cystic tumor of the spleen compressed the stomach. These images did not show any solid components. The preoperative diagnosis was lymphangiomatosis of the abdomen, because of multiple cystic lesions. However, we performed surgery because malignant cystic tumors could not be ruled out.
Figure 1. Computed tomography revealed a 72 mm cystic tumor of the spleen (a), and a 58 mm cystic tumor of the stomach (b)
On laparotomy, an exploration of the abdomen did not reveal any metastasis. There were also no abnormal findings involving the appendix or mesentery. One was an 86-mm cystic lesion at the antrum of the stomach, and it was resected with the distal stomach (Figure 1a). The other was an 88-mm cystic lesion of the spleen, and it was resected with the spleen (Figure 2a). The excision margins were tumor-free, and the regional lymph nodes were uninvolved.
Figure 2. Magnetic resonance imaging of the abdomen revealed a 70 mm tumor of the spleen which was high intensity in T1-weighted (a) and low intensity in T2-
weighted images (b), and a 52 mm tumor which was also high intensity in T1-weighted (c) and low intensity in T2-weighted images (b).
The patient followed an uneventful postoperative course and was doing well 64 months after the operation.
Pathological Findings
Pathological examination demonstrated mucinous cystadenoma associated with ectopic pancreatic tissue of the stomach (Figure 3) and mucinous cystadenocarcinoma of the spleen (Figure 4). Mucinous cystadenocarcinoma of the spleen invaded the splenic parenchyma with nuclear atypia. The walls of both tumors were composed of thick, collagenous, fibrous tissue, and were lined with epithelial cells and partially with papillary configuration. Neither tumor had an ovarian-like stroma (OLS) or estrogen receptor-positive cells. In addition, there was no anatomical association between the two lesions.
Figure 3. Mucinous cystadenoma associated with ectopic pancreatic tissue of the stomach: a) macroscopic, b) loupe, c) microscopic findings (X4), d) microscopic
findings (X10).
Figure 4. Mucinous cystadenocarcinoma of the spleen a) macroscopic, b) loupe. c) microscopic findings (X4), d) microscopic findings (X10).
DISCUSSION
Concerning the clinical and pathologic findings, our case showed independent tumors. To our knowledge, this is the first reported case of MCN with independent primary cystic lesions of the abdomen. MCNs make up a family of morphologically similar tumors arising in the pancreas, ovarium, appendix, hepatobiliary tract, and more rarely in the retroperitoneum, testis, spleen, bowel, and mesentery, and outside abdomen including lung and breast which were rare [1-6]
MCNs occur exclusively in younger females, and involve ovarian tissues or pancreas [3, 7, 8]. The rate of male in pancreatic MCNs was 1.9% [5]. On the other hand, there are a few reports of MCNs that originated at other sites [3-7]. Neoplasms derived from ectopic pancreas were sometimes reported [1, 2, 9]. Cárdenas CM et al. reviewed six cases of splenic tumor derived from ectopic pancreas [9]. Ectopic pancreas is one site of extra-ovarian MCNs, although there was no case derived from an ectopic pancreas of the stomach.
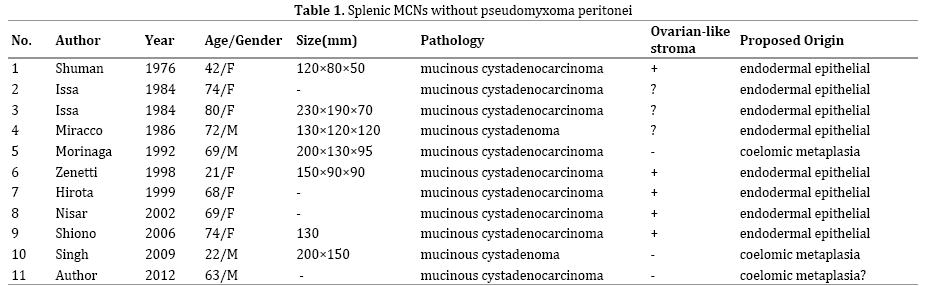
On the other hand, MCNs of the spleen not associated with pseudomyxoma peritonei were rare [4, 10]. Eleven cases of splenic MCNs without pseudomyxoma peritonei have been reported, and they are summarized in Table 1 [5, 11, 12-17]. Eight cases originated from endodermal epithelial tissues, and three from coelomic metaplasia. Eight of nine cases were malignant. Therefore, an early diagnosis of MCNs of the spleen is important because of their malignant potential [6].
Some theories have been proposed to explain the pathogenesis of extra-ovarian MCNs [7, 18, 19]. Extraovarian MCNs can arise from ectopic ovarian tissues, endodermal epithelial tissues including the pancreas and intestine, or coelomic metaplasia. In our case, the origin of the mucinous cystadenoma of the stomach was suspected to be an ectopic pancreas, while the origin of the mucinous cystadenocarcinoma of the spleen was unknown.
It has been reported that estrogen receptors are positive in stromal cells, and this is usually considered a diagnostic criterion for MCNs of the pancreas [8]. Shiono et al. also reported that extra-ovarian MCNs should be grouped together with OLS [6]. However, our patient was male, without residual ovarian tissues or OLS.
In the origin of endodermal epithelial tissues, MCNs occur from an ectopic pancreas or intestinal tissues. In our case, mucinous cystadenoma of the stomach was associated with an ectopic pancreas, while mucinous cystadenocarcinoma of the spleen did not show endodermal epithelial tissues. The origin of extra-ovarian MCNs was recently proposed to be from coelomic metaplasia of epithelial cells or an invaginated peritoneum that undergoes mucinous metaplasia with cyst formation [3, 11]. Pathological findings are compatible with mucinous cystadenocarcinoma of the spleen in our case. The pathogenesis of the two cystic tumors in our case could not be unitarily explained.
CONCLUSION
We surgically treated a male patient with mucinous cystadenoma associated with ectopic pancreatic tissues of the stomach and mucinous cystadenocarcinoma of the spleen, with no finding of oncological association between the two lesions.
Conflicting Interest
The authors had no conflicts of interest
References
- Nopajaroonsri C. Mucus retention in heterotopic pancreas of the gastric antrum a lesion mimicking mucinous carcinoma. Am J Surg Pathol 1994; 18:953-957. [PMID: 8067516]
- Barbe L, Levy P, Bougaran J, Just J, Mal F, Ruszniewski P, et al. Cystic and mucinous lesion in an antral ectopic pancreas. Gastroenterol Clin Biol 1998; 22:824-826. [PMID: 9854208]
- Metaxas G, Tangalos A, Pappa P, Papageorgiou I. Mucinous cystic neoplasms of the mesentery: a case report and review of the literature. World J Surg Oncol 2009; 7:47-54. [PMID: 19454018]
- Du Piessis DG, Louw JA, Wranz PA. Mucinous epithelial cysts of the spleen associated with pseudomyomaperitonei. Histopathology 1999; 35:551-557. [PMID: 10583579]
- Yamao K, Yanagisawa A, Takahashi K, Kimura W, Doi R, Fukushima N, et al. Clinicopathological features and prognosis of mucinous cystic neoplasm with ovarian-type stroma: a multi-institutional study of the Japan pancreas society. Pancreas 2011; 40:67-71. [PMID: 20924309]
- Shiono S, Suda K, Nobukawa B, Arakawa A , Yamasaki S ,Sasahara N, et al. Pancreatic, hepatic, splenic, and mesenteric mucinous cystic neoplasms (MCN) are lumped together as extra ovarian MCN. Pathol Int 2006; 56:71-77. [PMID: 16445818]
- Benkirane A, Mikou A, Jahid A, Zouaidia F, Laraqui L, Bernoussi Z, et al. Primary retroperitoneal mucinous cystadenoma with borderline malignancy in a male patient. A case report. Cases J 2009; 2: 1-5. [PMID: 20062675]
- Adsay NV: Cystic neoplasia of the pancreas pathology and biology. J Gastrointest Surg 2008; 12:401-404. [PMID: 17957438]
- Cárdenas CM, Domínguez I, Campuzano M, Bezaury P, Iñiguez-Rodríguez M, Gamboa-Domínguez A, et al. Malignant insulinoma arising from intrasplenic heterotopic pancreas. JOP 2009; 10:321-323. [PMID: 19454827]
- Ohe C, Sakaida N, Yanagimoto Y, Toyokawa H, Satoi S, Kwon AH, et al. A case of splenic low-grade mucinous cystadenocarcinoma resulting in pseudomyxomaperitoni. Med Mol Morphol 2011; 43:235-240. [PMID: 21267701]
- Morinaga S, Ohyama R, Koizumi J. Low-grade mucinous cystadenocarcinoma in the spleen. Am J Surg Pathol 1992; 16:903-908. [PMID: 1415909]
- Shuman RL, Bouterie RL: Cystadenocarcinoma of the pancreas presenting as a splenic cyst. Surgery 1976; 80:652-654. [PMID: 982285]
- Issa M, Buemi A, Holderbach LJ, Ratignier A, Laediein-Greilsammer D, Sengler J. Enteroid cyst of the spleen: a new entity? Apropos of 2 cases.J Chir 1984; 121:425-429. [PMID: 6480722]
- Miracco C, Martino AD, Lio R, Botta G, Volterrani L, Luzi P. Splenic cyst lined with mucous-secreting epithelium. Evidence of an intestinal origin. Arch Anat Cytol Pathol 1986; 34:304-306. [PMID: 3606226]
- Zanetti G, Riccioni L, Gallo C, Salfi N, Martinelli GN. Splenic mucinous cystadenocarcinoma arising in heterotopic pancreatic tissue.Tumori 1998; 84:606-610. [PMID: 9862526]
- HirotaM, Hayashi N, Tomioka T, Murakami S, Ohshima H, Yamasaki K, et al. Mucinous cystadenocarcinoma of the spleen presenting a point mutation of the Kirsten-ras oncogene at codon. Dig Dis Sci 1999; 44:768-774. [PMID: 10219836]
- Nisar PJ, Zaitoun AM, lobo DN, Rowlands BJ. Heterotopic pancreas in the spleen: malignant degeneration to mucinous cystadenocarcinoma. Eur Gastroenterol Hepatol 2002; 14:793-796. [PMID: 12169992]
- Banerjee R, Gough J. Cystic mucinous tumpurs of the mesentery and retroperitoneum: report of three cases. Histopathology 1988; 12:527-532. [PMID: 3397046]
- Yang DM, Jung DH, Kim H, Kang JH, Kim SH, Kim JH, et al. Retroperitoneal cystic masses: CT, clinical, and pathologic findings and literature review. Radiographics 2004; 24:1353-1365. [PMID: 15371613]





