Couder F1, Golfier F1, Traverse-Glehen A2, Devouassoux-Shisheboran M3 and Raudrant D1*
1Department of Gynecological and Oncological Surgery, University Lyon I, Lyon South Hospital Center, Hospices Civils de Lyon, Pierre Bénite, France
2Department of Anatomopathology, University Lyon 1, Lyon South Hospital Center, Hospices Civiles de Lyon, Pierre Bénite, France
3Department of Anatomopathology, University Lyon 1, Croix-Rousse Hospital Center, Hospices Civiles de Lyon, France
*Corresponding Author:
Daniel Raudrant
Centre Hospitalier Lyon Sud, Department of Gynecological and Oncological Surgery, 165 chemin du Grand Revoyet, 69495 Pierre-Bénite cedex, France
Tel: 0033(0)478866558
Fax: 0033(0)478861576
E-mail: daniel.raudrant@chu-lyon.fr
Received date: December 07, 2015; Accepted date: February 26, 2016; Published date: February 29, 2016
Keywords
Mayer-Rokitansky-Kuster-Hauser syndrome; Adenocarcinoma; Sigmoid vaginoplasty; Neovagina
Introduction
Mayer-Rokitansky-Küster-Hauser syndrome (MRKH), defined by a complete vaginal agenesis associated with uterine agenesis or hypoplasia, is uncommon with an incidence of 1/5000 female births. Patients usually present during the early teenage years with primary amenorrhoea and possible cyclic abdominal pain or mass due to endometrial shedding without a patent drainage pathway. The cause of the syndrome remains unclear, and failure of canalisation of the mülerian ducts during the 6th week of embryonic development is thought to be the main cause.
The best treatment for MRKH is still a matter of controversy. Surgical vaginoplasty is recommended only as second-line treatment after vaginal dilatation has failed or been refused. The use of a sigmoid vaginoplasty has been shown to provide good anatomical results [1,2].
The following is a report of the case of a patient who developed an adenocarcinoma arising from a sigmoid vaginoplasty. To our knowledge this is the 2nd case described in the literature.
Case Report
A 41-year-old female patient, suffering from MRKH, consulted for the first time at our hospital in 2003. A complete vaginal agenesis and a rudimentary uterus had been detected when she was 18 years old. The karyotype was normal. After a psychosexual assessment, we accepted her late request for a neovagina. The surgery by laparotomy consisted in using a segment of the sigmoid colon, vascularized by the last sigmoidal artery, as a neovagina. One month after the surgery, the patient was able to have satisfactory sexual intercourse.
She consulted in 2004 for a 20 mm prolapse of the sigmoid transplant that first required a promontory fixation by laparoscopy, and then a vaginal resection.
Seven years after the surgery, the patient presented vaginal bleeding especially after sexual intercourse. An endoscopy of the sigmoid transplant showed remodeling of the tissue. Multiple biopsy sampling revealed a liberkühnien adenocarcinoma. The size of the lesion was 55 mm long and 40 mm wide on magnetic resonance imaging (MRI), with an infiltration of the lymph nodes and the sigmoid fascia (Figure 1).
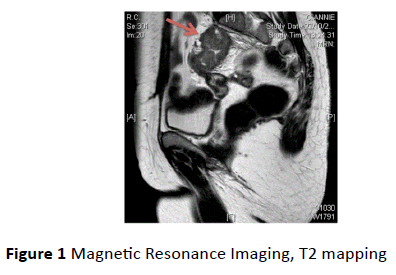
Figure 1 Magnetic Resonance Imaging, T2 mapping
Because of promontory fixation, the tumor had superficially invaded the cortical of the first sacral vertebra (Figure 2). A hepatic lesion was also suspected, on computed tomography scanning (CT). Otherwise colon endoscopy did not reveal another tumor. The patient underwent neoadjuvant chemotherapy with FOLFOX-ERBITUX, then radiochemotherapy with Xeloda and radiofrequency treatment on the hepatic lesion. In 2011 a resection of the transplant, a left hemicolectomy, an ovariectomy, a cholecystectomy and a segment-V liver segmentectomy were performed. The histology showed a mucinous adenocarcinoma that had penetrated the muscular layer, with no invasion of the lymph nodes or the adipose tissue (Figure 3). HPV DNA was not detected. There was only necrosis in segment V, and the resection was complete. The tumor was classified as ypT2N0M0. The patient had adjuvant chemotherapy with FOLFOX-ERBITUX.
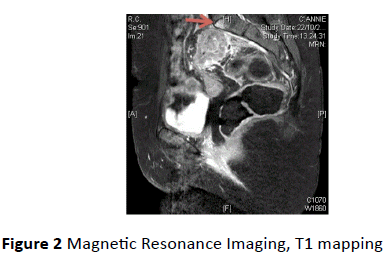
Figure 2 Magnetic Resonance Imaging, T1 mapping
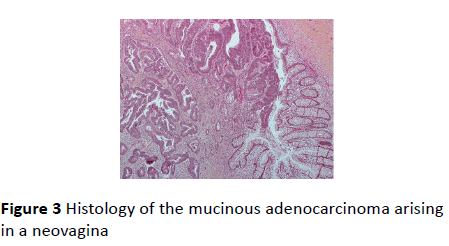
Figure 3 Histology of the mucinous adenocarcinoma arising in a neovagina
The patient came in for an emergency consultation, in April 2014, as she was suffering from sciatica, without motricity or sensory deficit. An isolated bone metastasis was diagnosed in the first sacral vertebra. She had radiotherapy and chemotherapy with FOLFOX-ERBITUX. The MRI performed in June revealed a reduction of the size of the metastasis, and the patient showed significant improvement.
Discussion
The different ways of handling the creation of a neovagina in women with MRKH are innumerable, probably because none is perfect [3]. Non-surgical vaginal dilatation, Franck’s method, must be proposed as a first-line treatement, because success rates are high and associated risks are low [4,5].
Surgical vaginoplasty is recommended only as a second-line treatment after vaginal dilatation has failed or been refused [3,6]:
• The laparoscopic Vechietti procedure is an accelerated Franck’s method, which requires special equipement [7].
• The Davydov procedure consists of a dissection, by laparoscopy, of the rectovesical space which is covered by the peritoneum [8].
• The McIndoe procedure is a perineal approach which involves creating a space between the rectum and the urethra followed by the use of a skin graft to form the epithelium of the neovagina [9].
• In the present case the sigmoid was used for the neovagina. Sigmoid vaginoplasty is a complex procedure, but it appears to be an attractive alternative with quick and satisfactory anatomical and sexual results [1]. Indeed, this operation allows an adequate vaginal length, the lack of shrinkage and the natural lubrification provided by the mucous production, which decreases the risk of dyspareunia [2].
Cancers of the neovagina are considered as a rare malignancy. To our knowledge this is the 24th case of carcinoma arising in the neovagina of patients who present vaginal agenesis, and the 2nd case in a sigmoid vaginoplasty [10,11].
In the literature there is at least one case of cancer from each most common method of surgical vaginoplasty. Liebrich C reported a case of squamous cell carcinoma in a neovagina which was constructed by Vecchietti procedure 28 years earlier [12]. Similarly, there are cancers described in Davydov and McIndoe procedures [13,14].
Hiroi reported a case of mucinous adenocarcinoma arising in a neovagina using the sigmoid colon, 20 years after surgery [11]. Just as in our case, the patient had complained of vaginal bleeding. Total resection of the neovagina and adjuvent radiotherapy were performed.
There is also a case of a primary vaginal cancer in a patient with MRKH syndrome who presented a bleeding from a blind vaginal pouch [15]. It is a reminder that a cancer can also arise in patients who did not have surgery, or just vaginal dilatation by Franck’s method. Therefore, it is crucial not to overlook the gynecological examinations of patients with MRKH, even if they did not have a surgical vaginoplasty.
Schober JM has published a review of the world literature to evaluate the different potential causes for the development of a cancer in a neovagina [16]. It must be borne in mind that tissue dysplasia may occur because the exogenous tissue, used for a neovagina, is suddenly subjected to new contacts or stresses. It can be, for instance, recurrent dilatation to keep the vagina open, microabrasion and trauma from sexual intercourse, reaction to semen and urine exposure, and reaction from stool if a fistula occurs. Human papillomavirus infection, which is sexually transmitted, is also known to increase the risk of developing a cancer, such as cervical or anal dysplasia. And yet it was not detected in the histology of our patient, neither in the other case of a tumor arising from a sigmoid vaginoplasty [11]. For this kind of surgery, chronic inflammation and ulcerative colitis can be a risk factor for a neovaginal carcinoma, even if in the present case the patient did not have such symptoms.
Conclusion
In almost every case of cancer arising of the neovagina, patients complain about vaginal bleeding. This underlines how important gynecological examination is on patients with MRKH, in particular patients who have undergone neovaginal construction. Indeed every patient with chronic vaginal bleeding has to undergo an endoscopic exploration with potential biopsy.
References
- Cai B, Zhang J, Xi X, Yan Q, Wan X (2007) Laparoscopically assisted sigmoid colon vaginoplasty in women with Mayer-Rokitansky-Kuster- Hauser syndrome: feasibility and short-term results. BJOG 114: 1486-1492.
- Carrard C, Chevret-Measson M, Lunel A, Raudrant D (2012) Sexuality after sigmoid vaginoplasty in patients with Mayer-Rokitansky-Küster-Hauser syndrome. Fertil Steril 97: 691-696.
- Nakhal RS, Creighton SM (2012) Management of vaginal agenesis. J Pediatr Adolesc Gynecol 25: 352-357.
- Ida S, Ismail-Pratt, Maligaye Bikoo, Lih-Mei Liao, Gerard S, et al. (2007) Normalization of the vagina by dilator treatment alone in Complete Androgen Insensitivity Syndrome and Mayer-Rokitansky-Kuster-Hauser Syndrome. Human Reproduction 7: 2020-2024.
- Frank RT (1938) The formation of artificial vagina without operation. Am J Obstet Gynecol 35: 1053-1055.
- Michala L, Cutner A, Creighton S (2007) Surgical approaches to treating vaginal agenesis 114: 1455-1459.
- Borruto F, Camoglioa FS, Zampieria N, Fedeled L (2007) The laparoscopic Vecchietti technique for vaginal agenesis. International Journal of Gynecology and Obstetrics 98: 15-19.
- Dargent D, Marchiolè P, Giannesi A, Benchaïb M, Chevret-Méasson M, et al. (2004) Laparoscopic Davydov or laparoscopic transposition of the peritoneal colpopoeisis described by Davydov for the treatment of congenital vaginal agenesis: the technique and its evolution. Gyne´cologie Obste´trique & Fertilite´ 32: 1023-1030.
- Klingele CJ, Gebhart JB, Croak AJ, DiMarco CS, Lesnick TG, et al. (2003) McIndoe procedure for vaginal agenesis: Long-term outcome and effect on quality of life. Am J Obstet Gynecol 189: 1569-1573.
- Kokcu A, Tosun M, Alper T, Sakinci M (2011) Primary carcinoma of the neovagina: a case report. Eur J Gynaecol Oncol 32: 588-9.
- Hiroi H, Yasugi T, Matsumoto K, Fujii T, Watanabe T, et al. (2001) Mucinous adenocarcinoma arising in a neovagina using the sigmoid colon thirty years after operation: a case report. Journal of Surgical Oncology 77: 61-64.
- Liebrich C, Reinecke-Lüthge A, Kühnle H, Petry KU (2006) Squamous cell carcinoma in neovagina at Mayer-Rokitansky-Küster-Hauser-syndrome. Zentralbl Gynakol 128: 271-274.
- Balik E, Maral I, Sözen U, Bezircioglu I, Tugsel Z, et al. (1992) Carcinoma arising in a Davydov neovagina. Geburtsh Fauenheilk 52: 68-69.
- Idrees MT, Deligdisch L, Altchek A (2009) Squamous papilloma with hyperpigmentation in the skin graft of the neovagina in Rokitansky syndrome: literature review of benign and malignant lesions of the neovagina. J Pediatr Adolesc Gynecol 22: e148-55.
- Tewari DS, McHale MT, Kuo JV, Monk BJ, Burger RA (2002) Primary invasive vaginal cancer in the setting of the Mayer-Rokitansky-Kuster-Hauser Syndrome. Gynecologic oncology 85: 384-387.
- Schober J (2007) Cancer of the neovagina. Journal of pediatric urology 3: 167-170.

