Sasha Mikhael*, Ivana Vettraino and Maria Lagopoulos
Department of Obstetrics and Gynecology, Providence-Providence Park/Michigan State University College of Human Medicine, Southfield, Michigan, USA
*Corresponding Author:
Sasha Mikhael
Department of Obstetrics and Gynecology
Providence-Providence Park/Michigan State University College of Human Medicine
Southfield, 711 Symes Avenue, Royal Oak MI 48067, Michigan, USA
Tel: 9177047613
E-mail: sasha.mikhael@gmail.com
Received Date: 1 Feb, 2016; Accepted Date: 20 Feb, 2017; Published Date: 22 Feb, 2017
Citation: Mikhael S, Vettraino I, Lagopoulos M. Moyamoya Disease in Pregnancy: A Multidisciplinary Approach, Gynecol Obstet Case Rep. 2017, 3:1. doi: 10.21767/2471-8165.1000045
Important Points
1. As immigration to the United States of America continues, medical conditions more prevalent in foreign countries will be seen more commonly in reproductive age women.
2. In order to optimize the care of a patient with a high risk of mortality in pregnancy, an organized, tightly aligned, hands on multidisciplinary team with clear communication is necessary.
Introduction
Moyamoya disease (MMD) is a rare and potentially devastating stenoocclusive disorder. MMD primarily results from progressive stenosis of the distal portions of the internal carotid artery (ICA) resulting in development of collaterals originating from the lenticulostriate arteries at the base of the brain [1]. These thin collaterals in imaging studies give the appearance of a “puff of smoke” which translates to Moyamoya in Japanese [2,3].
MMD predisposes those affected by the disease to recurrent cerebrovascular accidents (CVA). This medical condition has been predominantly reported in female Korean and Japanese children and young adults and thus can occur in pregnancy [4].
Although limited data exists regarding the severity of MMD during pregnancy and delivery it theorized that the physiologic changes associated with pregnancy including increased blood flow, hypercoagulability, and hyperventilation during delivery, can worsen symptoms of MMD [5]. Due to the lack of standard recommendations for its management, we present a case of MMD in pregnancy managed by a coordinated multidisciplinary team.
Case Report
The patient is a 31-year-old gravida 2 para 1 African American woman who presented to the academic obstetrics and gynecology clinic for her first prenatal visit with no prenatal care to date. Sonographic evaluation showed the patient to have a fetus at approximately 30 2/7weeks of gestation. She reported that she carries a diagnosis of MMD, discovered following the evaluation for a CVA occurring one month after delivery of her first child at 17 years of age. At that time, she presented to the emergency department with complaints of left sided eye and neck pain, dysarthria, word finding difficulties, and memory loss. Computerized tomography of the head showed a left temporooccipital infarct. A follow-up magnetic resonance angiogram (MRA) study demonstrated reconstitution of the middle cerebral artery (MCA) with collateral flow in the basal ganglia vessels, leptomeningeal collaterals, and collaterals at the base of the brain. A comprehensive evaluation, including a thrombophilia assessment, returned negative. She then suffered a second CVA one year following the first stroke. Repeat MRA study showed occlusion of the supraclinoid and bilateral internal carotid arteries with multiple small collaterals through the lenticular striate that reconstituted blood flow in the peripheral MCA and anterior cerebral artery branches. These findings confirmed the diagnosis of MMD at the age of 18 years. She underwent extracranial to intracranial bypass surgery to decrease the risk of future CVAs and was placed on clopidogrel that she discontinued 3 months ago, due to concerns regarding effects of the medication to the fetus. The patient was managed with no other medications. She did admit that she was advised to avoid pregnancy but was not utilizing reliable contraception.
The patient reported no other known medical or obstetrical history. Her family history was significant for both parents dying from CVAs but she had no knowledge of either parent carrying a diagnosis of MMD. Her physical exam was remarkable for morbid obesity with a body mass index of 48 and blood pressures of 140/96 mmHg.
Consultations from neurosurgery, anesthesia, and maternal fetal medicine services were obtained in an effort to assemble a multidisciplinary team to navigate the complexities of pregnancy in this patient. Recommendations included initiation of 325 mg aspirin orally daily and labetalol 100 mg orally every 8 hours for blood pressure control. Neurosurgical recommendations included a goal mean arterial pressure less than 80 mmHg and hemoglobin of greater than 10g/dL and to avoid hyperventilation and to maintain pCO2 levels within normal limits (Figure 1).
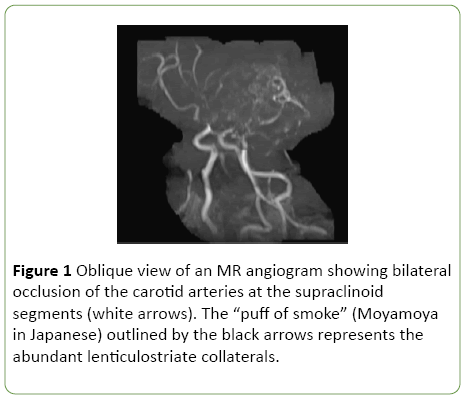
Figure 1: Oblique view of an MR angiogram showing bilateral occlusion of the carotid arteries at the supraclinoid segments (white arrows). The “puff of smoke” (Moyamoya in Japanese) outlined by the black arrows represents the abundant lenticulostriate collaterals.
The patient subsequently did well until 37 weeks of gestation at which time she underwent a scheduled primary cesarean section and bilateral tubal ligation as recommended by the above multidisciplinary team to allow for more optimal control of parameters such as blood pressure as well as to provide a controlled environment to optimize the patient and neonatal outcomes.
On the day of the scheduled cesarean delivery, the patient presented to labor and delivery in early labor. All consulted teams were notified and evaluated the patient. All participating care givers agreed on the plan to transport the patient to the main operating room, place an arterial line for optimal blood pressure assessment, and perform the cesarean section under general anesthesia to attempt to avoid recurrent embolic or ischemic event. The patient and family members were explained the concerns and rationale for the recommendations and also agreed. The patient underwent a rather uneventful cesarean section and Parkland tubal ligation. A live born male infant weighing 6 pounds and 6 ounces with Apgar scores of 5 and 9 at 1 and 5 minutes respectively was delivered without complication. An evaluation for superimposed postpartum preeclampsia took place on postoperative day 6 due to elevations in her blood pressure, which returned unremarkable. She followed up post-operatively in the clinic for continued evaluation of blood pressure and any signs of CVA but continue to do well with no complication.
Discussion
Physiologic changes associated with pregnancy include increased blood volume and hypercoagulation resulting in vasospasm that may cause consequential neurologic sequelae in patients with MMD [6]. Though a limited number of studies report the incidence of cerebrovascular accidents associated with MMD in pregnancy, there are reported cases from Japan and Korea that indicate that the rate of CVE’s is higher, with a much poorer prognosis, in those lacking appropriate care, especially if diagnosed in pregnancy when compared with patients who have pre-existing MMD prior to gestation [6,7]. Prognosis is reportedly much improved when blood pressures are tightly controlled.
One of the greatest concerns of MMD in pregnancy is the risk of intracranial haemorrhage with most cases reported in the third trimester, suggesting the possibility of it being related to gestational age. This has been correlated to increased blood volume and vascular resistance that significantly increases in the third trimester. This is why, some studies suggested cesarean delivery, to allow tighter control of blood pressure and mean arterial pressure [7,8]. Vaginal delivery results in hyperventilation and increased blood pressure which may trigger an intracranial haemorrhage or ischemia. However, in one small retrospective study by Fukushima et al. vaginal delivery was reported to be safe when using epidural anesthesia [8].
A point of reference in our case is the race of the patient. Most case reports and articles reference the Japanese and Korean populations as this is where MMD is mostly seen. Our patient is African American and this may have contributed to her diagnosis being delayed in her youth.
Due to safety concerns and the patient’s history of CVAs, her pregnancy and delivery were managed in a multidisciplinary approach including maternal fetal medicine, neurosurgery and anaesthesiology teams. Although the rate of complications is lower in previously diagnosed MMD prior to pregnancy, close monitoring is required in order to minimize the potential for a stroke. Though no specific recommendations have been concluded through the limited studies available, mode of delivery and form of anesthesia should be carefully selected based on an individual’s risk for cerebrovascular accidents during the peripartum and postpartum period. This can be optimized using a multidisciplinary approach.
References
- Akamatsu Y, Fujimura M, Uenohara H, Shimizu H, Tominaga T (2014) Development of Moyamoya disease in pregnancy and puerperium: A case report. Neurology Med Chir (Tokyo) 54: 824-826.
- Takahashi JC, Ikeda T, Iihara K, Miyamoto S (2012) Pregnancy and delivery in moyamoya disease: Results of a nationwide survey in Japan. Neurol Med Chir (Tokyo) 52: 304-310.
- Goto Y, Yonekawa Y (1992) Worldwide distribution of moyamoya disease. Neurol Med Chir (Tokyo) 32: 883-886.
- Jung Y, Kim M, Kwon J, Lee HR, Cho HY, et al. (2015) Pregnancy outcomes in women with moyamoya disease: Experiences at a single center in Korea. Younsei Med J 56: 793-797.
- Kim TS, Lee TH, Kim IY, Lee JK, Jung S, et al. (2004) Moyamoya disease with repeated intracranial haemorrhage in two consecutive pregnancies. J Cli Neurosci11(5): 525-527.
- Fujimura M, Akagi K, Uenohara H, Tominaga T (2013) Moyamoya disease: A single institute experience. Neural Med Chir (Tokyo) 53(8): 561-564.
- Takahashi JC, Ikeda T,Iihara K, Miyamoto S (2012) Pregnancy and delivery in moyamoya disease: Results of a nationwide survey in Japan. Neurol Med Chir (Tokyo) 52(5):304-310.
- Fukushima K, Yumoto Y, Kondo Y, Fujita Y, Morokuma S, et al. (2012) A retrospective chart review of the perinatal period in 22 pregnancies of 16 women with Moyamoya disease. Clin Neurosci19(10):1358-1362.

