Keywords
Diagnosis; General Surgery; Immunotherapy; Neoplasms; Pancreas; Pancreatectomy; Population Surveillance; Prognosis; Therapeutics
Abbreviations
FAMMM: familial atypical multiple mole melanoma; Hh: Hedgehog; HNPCC: hereditary non-polyposis colorectal cancer; SHh: sonic Hedgehog
INTRODUCTION
Pancreatic cancer is an aggressive and highly lethal malignant disease. Pancreatic cancer represents about 3% of new cancer cases, but it is responsible for 6% of deaths from malignant disease [1]. Nowadays, pancreatic cancer is the 4th (for females) or the 5th (for males) leading cause of death from cancer in the western world. Recent reports state that 5 year survival for all stages of pancreatic cancer is only 5% (15-20% for localized disease, 8% for pancreatic cancer with regional dissemination, and 2% for patients with distant metastases) [1]. Unfortunately, most pancreatic cancers are diagnosed late in their natural course; indeed, about 80% of pancreatic cancers have metastases at the time of diagnosis, either locoregional (25%) or distant (55%) [1, 2].
There has been little improvement in prognosis over the past 20 years. Radical surgery is the only hope for cure and increases medial overall survival to 13-15 months [2]. However, due to disease dissemination, surgery with therapeutic intent is possible in a minority of patients with pancreatic cancer (10-20%) [3]. Chemotherapy still relies on few drugs (including gemcitabine) and may further prolong survival, but only for a few months [4].
Given the dismal prognosis of pancreatic cancer and the relative inefficacy of currently available therapeutic methods, the need to develop other more effective diagnostic and therapeutic approaches is clear. The rapid development of modern molecular biology during the last two decades uncovered the genetic mechanisms controlling pancreatic carcinogenesis; new diagnostic and therapeutic tools have been developed or are under intense investigation, which hopefully will improve in the future the outcome of patients with pancreatic cancer. The aim of this paper is to summarize and critically evaluate currently available data regarding clinical implications of molecular biology of pancreatic cancer. Problems arising in everyday practice will also be discussed from a practical point of view.
Molecular Biology of Pancreatic Cancer: A Synopsis
An in depth discussion about molecular biology of pancreatic cancer is beyond the scope of this paper and has been presented in detail elsewhere [5, 6, 7]; therefore, only a brief description of our current knowledge regarding the molecular/genetic basis of pancreatic cancer will be presented.
Pancreatic cancer is a disease controlled by inherited and acquired mutations in cancer related genes, which could be classified into three categories:
• Oncogenes (K-ras, BRAF, AKT 2, MYB, and AIBI)
• Tumor-supressor genes (p16/CDKN2A, p53, p21, and SMAD4)
• Genome-maintenance genes (MLH, MSH2, BRCA2 and other Fanconi anemia genes).
Oncogenes
K-ras mutations are very common (>90%) in pancreatic cancer and are usually restricted to codon 12. K-ras mutations impair intrinsic GTPase activity resulting in a protein that is constitutively active in signal transduction, resulting in alterations in cell proliferation, survival, and migration. K-ras mutations are an early genetic event in pancreatic carcinogenesis and are considered as a ‘signature’ for pancreatic cancer. BRAF gene mutations are observed in about 30% of the pancreatic cancers with wild-type (normal) K-ras gene. BRAF and K-ras gene mutations are mutually exclusive, i.e. one of them is not observed in the presence of the other. Other oncogenes amplified in pancreatic cancer include the AKT1 gene, AKT2 gene, and MYB gene; amplification of these genes is observed in 60%, 10-15%, and 10% of pancreatic cancers, respectively. In addition to these genes, a number of amplicons (amplified fragments of DNA) have been identified in pancreatic cancers, including a localized region on long arm of chromosome 8, corresponding to the oncogenic transcription factor CMYC. Probably there are too many other oncogenes which still remain unknown.
Tumor Suppressor Genes
Inactivation of the p16 gene is observed in 80-95% of sporadic pancreatic cancers. The combination of p16 and K-ras mutations is uncommon in other human tumors and is considered as a molecular ‘signature’ for pancreatic cancer. p16 gene inactivation is observed at a later stage in pancreatic carcinogenesis compared to K-ras mutations (Figure 1). p53 gene inactivation is observed in 55-75% of pancreatic cancers and is a late event in pancreatic tumorigenesis. p21 gene inactivation is an early event in the development of pancreatic carcinoma, appearing at a progressively higher frequency during the progression from normal ducts (9%) to Pan IN to invasive pancreatic cancer (>85%). MTAP gene function is completely lost in about one third of infiltrating pancreatic cancers, but concurrent (by chance) deletion during inactivation (again by deletion) of the p16 gene. SMAD4 gene plays a critical role in signaling through the TGF-beta pathway. SMAD4 gene inactivation occurs in about 55% of pancreatic cancers. BRCA1 and BRCA2 genes are mutated in most advanced PanIN lesions, whereas a germline mutation in either gene represents the earliest risk factor in many familial pancreatic cancer cases. BRCA2 (her-2/neu) gene mutation carriers have an increased (10-fold) risk of developing pancreatic cancer than the general population. There are too many others tumor-suppressor genes involved in pancreatic carcinogenesis, including STKII/LKBI, MKK4, TGFbeta- RI (ALK5), TGF-beta-R2, ACVRI-beta (ALK 4), ACVR2, FBXW7 (CDC4) and EP300.
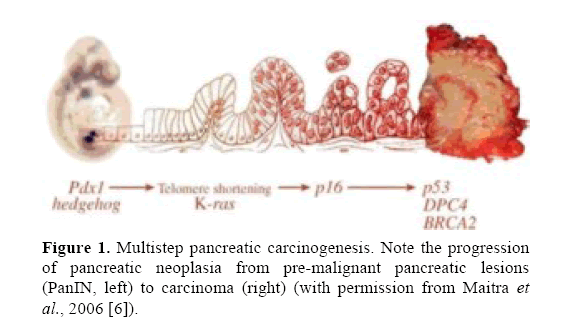
Figure 1. Multistep pancreatic carcinogenesis. Note the progression of pancreatic neoplasia from pre-malignant pancreatic lesions (PanIN, left) to carcinoma (right) (with permission from Maitra et al., 2006 [6]).
Genome Maintenance Genes
These genes are responsible for the identification and repair of damage to DNA. As a result of inactivation of such a gene, the damaged DNA is not repaired efficiently and DNA damages remain accumulating, thereby contributing in carcinogenesis. This group of genes includes MLH1 and MSH2 and the Falconi anemia genes (FANCC, FANCG, etc.), which are targeted in a small percentage of patients with pancreatic cancer (<10%).
Other Genetic Mechanisms Involved in Pancreatic Carcinogenesis
Telomere shortening, expression of specific proteins, upregulation and overexpression of growth factors and/or their receptors (such as EGFR, TGF-beta, etc.), altered expression of angiogenetic factors and their receptors (VEGF-A, VEGFR1 and VEGF2, PEDF, etc.) are also mechanisms involved in the process of pancreatic carcinogenesis. Derangements of developmental signaling pathways (mainly the Hedgehog (Hh) signaling pathway) are also observed in pancreatic cancer, as observed by the expression of the sonic Hh (SHh) protein in 70% of human pancreatic cancer.
Currently, pancreatic carcinogenesis is considered to be a multistep phenomenon, characterized by specific genetic mutations that take place during the evolution of a pre-invasive pancreatic lesion to pancreatic cancer; of note, these genetic alterations occur in an ordered sequence rather than a random fashion (Figure 1).
Applying Molecular Biology in Clinical Practice: Where Are We Today Regarding Pancreatic Cancer?
Evolution of molecular biology has been impressive during the last two decades. Sequencing of the human genome is now possible and a huge number of genetic markers can be identified in a single patient. From a clinical point of view, however, the real challenge remains to determine how these impressive progresses could improve clinical management of cancer patients. Nowadays, potential clinical implications include genetic counseling for individuals at high-risk for developing pancreatic cancer, early detection of pancreatic cancer, determination of prognosis, and mechanism-based therapies for pancreatic cancer.
Genetic Counseling
The identification of individuals with an increased risk for the development of pancreatic cancer is obviously of particular clinical importance. Hereditary pancreatic cancer represents about 5-15% of pancreatic cancers and is directly attributable to genetic alterations [8, 9]. There are three groups of patients characterized by an inherited predisposition for pancreatic cancer development [7, 8, 9, 10, 11]: i) patients with familial cancer syndromes associated with an increased risk of pancreatic cancer (i.e., familial atypical multiple mole melanoma (FAMMM) syndrome, Peutz-Jeghers syndrome, and hereditary non-polyposis colorectal cancer (HNPCC) syndrome); ii) individuals belonging to families with a history of familial pancreatic cancer. The risk of developing pancreatic cancer among firstdegree relatives of an individual belonging to such families increases with the number of affected family members (18-fold with two; 57-fold with three affected members); iii) patients with benign diseases associated with inherited pancreatic cancer, such as chronic hereditary pancreatitis, cystic fibrosis, ataxia telangiectasia, etc.
As above noted, germline p16 gene mutations are associated with the FAMMM syndrome (which is characterized by an increased incidence of melanoma and pancreatic cancer (from 20 to 34-fold)). Based on this, it has been suggested that patients with a family history of melanoma, multiple atypical nevi, and a family history of pancreatic cancer can obtain genetic testing for germline p16/CDKN2A gene mutations. Those found to carry a germline mutation would benefit from increased surveillance for skin cancer and, as tests for pancreatic cancer become available, for screening for early pancreatic neoplasia [6].
BRCA2 gene mutation carriers have an increased (10- fold) risk of developing pancreatic cancer compared to general population (see above), as well as an increased risk of developing breast, prostate, and ovarian cancer. Moreover, germline (inherited) mutations in BRCA2 can cause the familial aggregation of pancreatic cancer [12]. Individuals with a family history of cancer can be screened for a germline BRCA2 mutation to establish cancer risk profiles; management options should then discussed with the patient (for example, intensive surveillance, chemoprevention, or prophylactic mastectomy to prevent breast cancer or intensive surveillance for early detection of pancreatic cancer or preferentially preinvasive disease) [6, 13].
In addition to p16 and BRCA2, genetic analysis for individuals with a family history of pancreatic cancer with or without other cancers could include genetic testing for inherited (germline) mutation in other genes known to predispose to familial pancreatic cancer, such as STKII, PRSSI, BRCA1 and MLH1.
Practically, individuals found to carry specific gene mutations responsible for the aggregation of cancer in their family should follow a program of intense surveillance, aiming to detect pancreatic and extrapancreatic neoplasms at an early stage, ideally before the development of invasive cancer and before the development of clinical manifestations; at this early stage of pancreatic neoplasia radical surgical resection is still possible and cure can be achieved [14]. This surveillance program should include periodic examination of the patients using modern imaging methods, such as endoscopic ultrasonography and multidetector computed tomography. Molecular tests to detect genetic alterations found specifically in early pancreatic neoplasia could also be used.
From a clinical point of view, it should be noted that the concept of “prophylactic pancreatectomy” is currently considered by many as a too aggressive and basically unjustified approach, in contrast to prophylactic thyroidectomy or prophylactic mastectomy in individuals found to carry specific genetic alterations. This could be explained by the significantly higher surgical morbidity and mortality of a major pancreatectomy compared to total thyroidectomy or mastectomy. However, this strategy has been applied in clinical practice; Canto et al. at Johns Hopkins screened 38 asymptomatic patients with a strong history of family pancreatic cancer, while one had Peutz-Jeghers syndrome, using endoscopic ultrasonography (EUS); six pancreatic masses were found in this group of patients [15]. The same group found that noninvasive precursor lesions are more common in patients with a strong familial history of pancreatic cancer than in patients with sporadic disease; precursor lesions were of a higher grade in patients with a strong family history of pancreatic cancer [16]. Once detected, by using a combination of multi-detector CT scan and EUS, resection of these preinvasive lesions could achieve cure from a highly lethal disease (i.e., invasive pancreatic cancer). However, until now the target group of individuals which should be included in intensive surveillance programs remains undefined; moreover, the diagnostic strategy which is indicated during the follow-up of these individuals remains controversial and somehow ambiguous; therefore clear and robust recommendations are not possible at this time [17, 18].
To further emphasize the clinical applicability of the concept of prophylactic pancreatectomy, is should be noted that pancreatectomy in patients with noninvasive cystic pancreatic neoplasms (such as noninvasive mucinous cystic neoplasms or noninvasive intraductal papillary mucinous neoplasms) is essentially prophylactic, i.e. is performed when the disease is at the stage of preinvasive neoplasia to prevent the highly possible development of invasive disease. In this case, the risk associated with a major pancreatic resection is accepted and pancreatectomy is indicated [19, 20]. For the same reasons, prophylactic pancreatectomy aiming to resect preinvasive pancreatic lesions (such as PanIN) in individuals with specific mutation carriers is also justified; it appears that the concept of prophylactic pancreatectomy will be more appealing in the future. Needless to say that such a surgical procedure should be performed in hospitals and by surgeons with significant experience and interest in pancreatic surgery to minimize surgical morbidity and mortality rates.
Diagnosis
Given the dismal prognosis of pancreatic cancer, even in patients with resectable disease, early diagnosis at an early (preclinical) and potentially curable stage is required to improve therapeutic results. Molecular changes occurring early during tumor progression are preferred to diagnose pancreatic neoplasia at a stage where there is committal to invasive pancreatic cancer, but where the lesion is still treatable. The clinical impact of diagnosing preinvasive or even early pancreatic cancer could be tremendous; indeed, there is some evidence suggesting that resection of small (<1 cm) pancreatic cancers can achieve a 100% 5-year survival [21]. Molecular analysis could be performed on samples of biologic material, such as serum or plasma, duodenal fluid or (preferentially) pure pancreatic juice, pancreatic cells obtained by fineneedle aspiration (FNA) or cytological brushings, bile and stools, or at tissue level (on surgical specimens). ERCP allows collection of pure pancreatic juice for genetic analysis, brush cytology and biopsy [22]. Detection of K-ras mutations in this material has been proposed for the early diagnosis of pancreatic cancer [23, 24, 25]. Localization of K-ras mutations to a single codon (codon 12) in the vast majority of pancreatic cancers greatly facilitates genetic testing to detect specifically these mutations rather than to examine the entire gene [6]. However, K-ras mutations in the pure pancreatic juice are also observed in patients with benign diseases (albeit at a much lower frequency), such as chronic pancreatitis (up to 40% of patients) or even biliary tract stones, thereby substantially diminishing the specificity of this genetic test [23, 24, 26].
Expression of mesothelin, as detected by immunolabeling, can be used in the interpretation of difficult biopsies of the pancreas [27]. Mesothelin can also be detected in the serum [6]. Quantitative determination of p16INK4a promoter CpG island methylation has been examined as a screening modality for pancreatic cancer, with a reported specificity and sensitivity of about 90% and greater than 60%, respectively [22, 28]. Immunocytology can detect mutant p53 indirectly as a result of accumulation of mutant p53 protein within cells [29]. Mutations of p53 genes have also been detected in pancreatic juice; these mutations could be used to differentiate pancreatic cancer from chronic pancreatitis [29]. Increased telomerase activity in pure pancreatic juice has been observed in a high percentage of patients with pancreatic cancer (about 80%), but in none of patients with chronic pancreatitis or normal pancreas [30]. Immunohistochemical labeling for the SMAD4 protein in biopsies and resected tissues could be used in the interpretation of histological findings in difficult cases [6, 31]. Loss of SMAD4 expression strongly supports the diagnosis of pancreatic cancer, while intact SMAD4 expression supports the diagnosis of a non-pancreatic malignancy. This could be useful in the evaluation of metastatic lesions (from the pancreas to other organs and conversely). Microsatellite instability in patients with pancreatic cancers has been associated with a risk of developing other cancers (as a part of multi-organ cancer syndromes, such as HNPCC); this association should be taken into consideration when treating patients with pancreatic cancer and microsatellite instability in order to plan a management strategy to achieve early detection of other synchronous or metachronous extrapancreatic cancers [32, 33].
From a surgical and practical point of view, it should be noted that frequently surgical resection is performed for a pancreatic mass which could be inflammatory (i.e., chronic pancreatitis) or neoplastic [26, 34, 35]. Practically, differential diagnosis of these two entities is not always possible, especially when the clinical presentation and laboratory/imaging findings are not typical. In this case the highly sophisticated modern diagnostic approach (which could include determination of molecular/genetic indices) may be unreliable and accurate diagnosis in the individual patient is often possible only following radical resection of the affected pancreatic parenchyma, which is appropriate therapy for both chronic pancreatitis as well as for pancreatic cancer [35, 36].
Prognosis
Several molecular alterations observed in pancreatic cancer have prognostic significance. For example, Kras gene mutations have been reported as a negative prognostic factor after surgery and adjuvant chemoradiation, or surgery alone. Increased expression of EGFR or its ligands has been associated with an enhanced malignant phenotype and a worse prognosis [37, 38]; EGFR overexpression is also associated with a high probability to respond to anti-EGFR agents [39]. In contrast, pancreatic cancers with genomemaintenance genes mutations and microsatellite instability may have a better prognosis, but they may show a different response to some chemotherapeutic regimens [6, 32]. Loss of SMAD4 expression correlates with a better survival following resection of pancreatic cancer [39, 40]. Therefore, information based on genetic/molecular profile of pancreatic cancer could be used to determine cancer sub-types, classify tumor phenotype, and determine prognosis (in association with known prognostic factors) with a higher accuracy [41].
Therapy
Biochemical differences caused by the specific genetic alterations observed in pancreatic cancer could be used to target malignant cells, avoiding at the same time damage of normal cells. For example, the CAPANI pancreatic cancer cell line harboring BRCA2 gene mutations is very sensitive to the DNA cross-linking agent mitomycin C [6, 42, 43]. In experimental models, purine synthesis inhibitors (such as L-alanosine) have been used to target the selective loss of Mtap function observed in cancers [6]. Since angiogenesis is essential for tumor growth, antiangiogenetic therapy represents an interesting type of treatment of pancreatic cancer. Bevacizumab (a humanized monoclonal antibody against VEGF) has been used in combination with gemcitabine in pancreatic cancer, but without significantly prolonging survival [44]. Other angiogenic inhibitors that target other non-VEGF pathways (such as sorafenib which inhibits the VEGF receptor, platelet-derived growth factor receptor (PDGFR), stem-cell factor receptor (SCFR), Rafl, and FMS-like tyrosine kinase 3 (FLT3) have been used in the treatment of advanced pancreatic cancer with poor results [45]. Other antiangiogenetic agents, such as axitinib, aflibercept, integrin, and cilengitide, have been used in the management of metastatic pancreatic cancer, without improving patient’s outcome [44]. Erlotinib (an orally active anti-EGFR inhibitor) has demonstrated a small but statistically significant increase in the survival of patients with advanced pancreatic cancer [46]; in 2005, erlotinib was the first targeted therapy approved by the FDA for pancreatic cancer. Another anti-EGFR agent is cetuximab, which however was ineffective in phase III trial in patients with locally advanced and metastatic pancreatic cancers [47], but is still under investigation in the treatment of pancreatic cancer. Matrix metalloproteinase inhibitors (MMPIs) are other examples of angiogenesis inhibitors, which have been used in the treatment of pancreatic cancer, without prolonging survival [48]. Cyclooxygenase inhibitors reduce angiogenesis and invasiveness of cancer and enhance apoptosis; these antiangiogenetic agents have also been used in the treatment of pancreatic cancer, with conflicting results [38].
Tumor-stroma interaction (which is important for the progress of pancreatic cancer) can mediate specific gene expression in the tumor, which could be used as a therapeutic target [49]. Cyclopamine specifically inactivates the hedgehog pathway (see above); it has been shown that cyclopamine produces dramatic antitumor effects in xenograft models of human pancreatic cancers without demonstrable side effects in treated mice [50]. Intense research is focused in developing more potent inhibitors of the hedgehog pathway.
Other therapeutic approaches in pancreatic cancer based on molecular biology include gene therapy and signal transduction inhibition and oncolytic viral therapy [51]. Intensive research efforts are focused on the role of immunotherapy in cancer treatment; immunotherapy currently represents the most important and rapidly grown area of cancer research. Passive immunotherapy includes the use of antitumor agents that have been generated in vitro (antibodies, effector cells, etc.), whereas active immunotherapy aims to stimulate an antitumor response in vivo by means of vaccination [52, 53].
Conflict of interest
The authors have no potential conflict of interest
References
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009. CA Cancer J Clin 2009; 59: 225-49.
- Neoptolemos JP, Dunn JA, Stocken DD, et al. Adjuvant chemoradiotherapy and chemotherapy in resectable pancreatic cancer. A randomized controlled trial. Lancet 358:1576–85.
- Orr RK. Outcomes in pancreatic cancer surgery. Surg Clin North Am 2010; 90: 219 – 234.
- Abbruzzese JL. New applications of gemcitabine and future directions in the management of pancreatic cancer. Cancer 2002; 95:941–5.
- Sakorafas GH, Pappa I, Smyrniotis V. Pancreatic cancer: molecular genetics and clinical applications. Encyclopedia of Life Sciences 2010; Edition] [In Press].
- Maitra A, Kern SE, Hruban RH. Molecular pathogenesis of pancreatic cancer. Best Pract Res Clin Gastroenterol 2006; 20: 211 – 226.
- Vitone LJ, Greenhalf W, Mc Faul CD, Neoptolemos JP. The inherited genetics of pancreatic cancer and prospects for secondary screening. Best Pract Res Clin Gastroenterol 2006; 20:253 – 283.
- Lynch HT, Smyrk T, Kern SE et al. Familial pancreatic cancer: a review. Semin Oncol 1996; 23: 251–275.
- Silverman DT, Schiffman M, Everhart J et al. Diabetes mellitus,other medical conditions and familial history of cancer as risk factors for pancreatic cancer. Br J Cancer 1999; 80: 1830–1837.
- Bartsch DK. Familial pancreatic cancer. Br J Surg 2003; 90: 386–387.
- Tersmette AC, Petersen GM, Offerhaus GJ et al. Increased riskof incident pancreatic cancer among first-degree relatives of patients with familial pancreatic cancer. Clin Cancer Res 2001; 7: 738–744.
- Murphy KM, Brune KA, Griffin CA et al. Evaluation of candidate genes MAP2K4, MADH4, ACVR1B, and BRCA2 in familial pancreatic cancer: deleterious BRCA2 mutations in 17%. Cancer Res 2002; 62: 3789–3793.
- Greer J, Whitcomb D. Role of BRCA 1 and BRCA 2 mutations in pancreatic cancer. Gut 2007; 56: 601–5.
- Goggins M, Canto M, Hruban R. Can we screen high-risk individuals to detect early pancreatic carcinoma? J Surg Oncol 2000; 74: 243 – 248.
- Canto MI, Goggins M, Yeo CJ et al. Screening for pancreatic neoplasia in high-risk individuals: an EUS- based approach. Clin Gastroenterol Hepatol 2004; 2[7]: 606–621. JOP. J Pancreas (Online) 2012 Jul 10; 13(4):332-337. JOP. Journal of the Pancreas - https://www.serena.unina.it/index.php/jop - Vol. 13 No. 4 - Jul 2012. [ISSN 1590-8577] 337
- Shi C, Klein AP, Goggins M, et al. Increased. prevalence of precursor lesions in familial pancreatic cancer patients. Clin Cancer Res 2009; 15: 7737 – 7743
- Canto MI. Screening and surveillance approaches in familial pancreatic cancer. Gastrointestinal EndoscClin N Am 2008; 18: 535 – 553.
- Harinck F, Canto MI, Schulick R, et al. Surveillance in individuals at high risk of pancreatic cancer: too early to tell? Gut 2010; 59: 1006 – 100719. Sakorafas G, Smyrniotis V, Lombardo KMR, Sarr MG. Primary pancreatic cystic neoplasms revisited. Part II. Mucinous cystic neoplasms. Surg Oncol [In Press]
- Sakorafas G, Smyrniotis V, Lombardo KMR, Sarr MG. Primary pancreatic cystic neoplasms revisited. Part III. Intraductal Papillary Mucinous Neoplasms.Surg Oncol [In Press]
- Ishikawa O, Ohigashi H, Imaoka S et al. Minute carcinoma of the pancreas measuring 1 cm or less in diameter—collective review of Japanese case reports. Hepatogastroenterology 1999; 46: 8–15.
- Yan L, Mc Faul C, Howes N et al. Molecular analysis to detect pancreatic ductal adenocarcinoma in high-risk groups. Gastroenterology 2005; 128: 2124–2130.
- Sakorafas GH, Tsiotou AG, Tsiotos GG. Molecular biology of pancreatic cancer: oncogenes, tumor suppressor genes, growth factors and their receptors from a clinical perspective. Cancer Treat Rev 2000; 26: 29-52.
- Sakorafas GH, Tsiotos GG. Molecular biology of pancreatic cancer; potential clinical implications.Bio Drugs 2001; 15: 439 – 452.
- Howes N, Greenhalf W &Neoptolemos J. Screening for early pancreatic ductal adenocarcinoma in hereditary pancreatitis. Med Clin North Am 2000; 84: 719–738.
- Sakorafas GH, Tsiotou AG. Pancreatic cancer in patients with chronic pancreatitis: a challenge from a surgical perspective. Cancer Treat Rev 1999; 25: 207 – 217.
- Argani P, Iacobuzio-Donahue CA, Ryu B et al. Mesothelin is overexpressed in the vast majority of ductal adenocarcinomas of the pancreas: identification of a new pancreatic cancer marker by serial analysis of gene expression [SAGE]. Clin Cancer Res 2001; 7[12]: 3862–3868.
- Klump B, Hsieh CJ, NehlsOet al. Methylation status of p14ARF and p16INK4a as detected in pancreatic secretions. Br J Cancer 2003; 88: 217–222.
- Yamaguchi Y, Watanabe H, Yrdiran S et al. Detection of mutations of p53 tumor suppressor gene in pancreatic juice and its application to diagnosis of patients with pancreatic cancer: comparison with K-ras mutation. Clin Cancer Res 1999; 5: 1147– 1153.
- Uehara H, Nakaizumi A, Tatsuta M, et al. Diagnosis of pancreatic cancer by detecting telomerase activity in pancreatic juice: comparison with K-ras mutations. Am J Gastroenterol 1999; 94: 2513–19.
- Wilentz RE, Su GH, Dai JL et al. Immunohistochemical labeling for Dpc4 mirrors genetic status in pancreatic adenocarcinomas: a new marker of DPC4 inactivation. Am J Pathol 2000; 156: 37–43.
- Yamamoto H, Itoh F, Nakamura H et al. Genetic and clinical features of human pancreatic ductal adenocarcinomas with widespread microsatellite instability. Cancer Res 2001; 61[7]: 3139–3144.
- Nakata B,Wang YQ, Yashiro M et al. Prognostic value of microsatellite instability in resectable pancreatic cancer. Clin Cancer Res 2002; 8[8]: 2536–2540.
- Sakorafas GH, Farnell MB, Farley DR, et al. Long-term results after surgery for chronic pancreatitis. Int J Pancreatol 2000; 27: 131 – 142.
- Sakorafas GH, Farmell MB, Nagorney DM, et al. Pancreatoduodenectomy for chronic pancreatitis: long-term results in 105 patients. Arch Surg 2000; 135: 517 – 523.
- Stapleton GN, Williamson RC. Proximal pancreatoduodenectomy for chronic pancreatitis.Br J Surg 1996; 83:1433 – 1440.
- MacKenzie MJ. Molecular therapy in pancreaticadenocarcinoma. Lancet Oncol 2004;5[9]:541–9.
- Oliveira-Cunha M, Siriwardena AK, Byers R. Molecular diagnosis in pancreatic cancer. Diagn Histopathol 2008; 14: 214 – 222.
- Tascilar M, Skinner H, Rosty C, et al. The SMAD4 protein and prognosis of pancreatic ductal adenocarcinoma. Clin Cancer Res 2001; 7: 4115.
- Welsh J, Sapinoso L, Kern S, et al. Large-scale delineation of secreted protein biomarkers overexpressed in cancer tissue and serum. Proc Natl Acad Sci USA 2003; 100: 3410–15.
- Couch FJ, Johnson MR, Rabe K et al. Germ line Fanconi anemia complementation group C mutations and pancreatic cancer. Cancer Res 2005; 65[2]: 383–386.
- van der Heijden MS, Yeo CJ, Hruban RH & Kern SE. Fanconi anemia gene mutations in young-onset pancreatic cancer. Cancer Res 2003; 63[10]: 2585–2588.
- Wong HH, Lemoine NR. Pancreatic cancer: molecular pathogenesis and new therapeutic targets. Nat Rev Gastroenterol Hepatol 2009; 6: 412 – 422.
- Wallace JA, et al. Sorafenib [S] plus gemcitabine [G] for advanced pancreatic cancer [PC]: A phase II trial of the University of Chicago Phase II Consortium [Abstract]. J Clin.Oncol 2007;25:a4608.
- Moore MJ, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 2007;25:1960–1966.
- Philip PA, et al. Phase III study of gemcitabine [G] plus cetuximab [C] versus gemcitabine in patients [pts] with locally advanced or metastatic pancreatic adenocarcinoma [PC]: SWOG S0205 study [Abstract]. J. Clin. Oncol 2007;25:a4509.
- Bramhall SR, Schulz J, Nemunaitis J, Brown PD, Baillet M, Buckels JA. A double-blind placebo-controlled, randomised study comparing gemcitabine and marimastat with gemcitabine and placebo as first line therapy in patients with advanced pancreatic cancer. Br J Cancer 2002;87:161–7.
- Iacobuzio-Donahue CA, Ryu B, Hruban RH & Kern SE. Exploring the host desmoplastic response to pancreatic carcinoma: gene expression of stromal and neoplastic cells at the site of primary invasion. Am J Pathol 2002; 160[1]: 91–99.
- Thayer SP, di Magliano MP, Heiser PWet al. Hedgehog is an early and late mediator of pancreatic cancer tumorigenesis. Nature 2003; 425[6960]: 851–856.
- Wong HH, Lemoine NR. Biologic approaches to therapy of pancreatic cancer. Pancreatology 2008; 8: 431 – 461.
- Nakamura M, Wada K, Suzuki H, et al. Long-term outcome of immunotherapy for patients with refractory pancreatic cancer. Anticancer Res 2009; 29: 831 – 836.
- Abou-Alfa GK, Chapman PB, Feilchenfeldt J, et al. Targeting mutated K-ras in pancreatic adenocarcinoma using an adjuvant vaccine. Am J Clin Oncol 2010, Aug 3. [PMID:20686403].

