Keywords
Laparoscopy; Minimally Invasive Surgical Procedures; Pancreaticoduodenectomy; Robotics; Whipple Disease
Abbreviations
MIS minimally invasive surgical; MIPD minimally invasive pancreaticoduodenectomy; PD pancreaticoduodenectomy;
BACKGROUND
Pancreatic cancer is the fourth leading cause of cancerrelated death among men and women in the United States. It is the most lethal cancer with a mean 5-year survival rate of 4-6% for all comers [1]. Despite the advent of new chemotherapeutic, immunologic, and radiologic treatment modalities the only potential for cure remains surgical expatriation of the tumor with its draining lymphatic basins.
While the anatomic boundaries of a pancreaticoduodenectomy (PD) have not changed, the operative approach significantly changed with development of minimally invasive surgical techniques (MIS). Here we define a minimally invasive pancreaticoduodenectomy (MIPD) as either a completely laparoscopic or robotic approach including both the dissection and reconstruction phases. While an MIS approach does not significantly modify the steps in the operation itself, for a MIPD the hope is that the method by which these steps are undertaken are less traumatic/ inflammatory and potentially more precisely performed [2, 3]. The advantages that MIS has provided to other more common procedures such as the cholecystectomy include those related to an enhanced visualization of the operative field with magnification and illumination resulting in less blood loss during surgery and an enhanced recovery after surgery with less pain and less wound- related complications such as wound infections and hernias.
Initial concern that a MIS approach would compromise oncologic principles has been investigated in several non-pancreatic malignancies. The Clinical Outcomes of Surgical Therapy Study Group (COST) demonstrated noninferiority between laparoscopic assisted colectomy and the traditional open approach for colon cancer [4]. These results were supported by the European Colon Cancer Laparoscopic or Open Resection study group trial (CCLOR) which again compared results for colon cancer between laparoscopic and open surgery [5]. While laparoscopy has been readily adopted for lesions in the distal pancreas with equivalent short and long-term oncologic outcomes [6] there have been less widespread acceptance of a laparoscopic approach for lesions in the head of the pancreas.
The first reported MIPD in 1994 garnered both enthusiasm and concern [7]. The typical advantages of decreased pain, reduced wound-related complications, shorter hospitalizations and quicker recovery that have been observed with several MIS abdominal procedures was tempered by concerns for increased complexity, longer operative times, the need for advanced laparoscopic skills and a lack of perceived benefits and potentially increased morbidity and mortality. These concerns were again highlighted in a recent analysis of 7061 patients from the National Cancer Database (NCDB) between 2010-2011 that revealed that most (~92%) MIPD were performed in low volume centers (<10 cases/2 years), while there were no differences in terms of number of lymph nodes, rate of positive surgical margins, length of stay or readmission, the 30-day mortality was significantly higher for patients undergoing MIPD versus open surgery (OR=1.87, confidence interval 1.25-2.80, p=0.002) [8]. This study identifies several important issues regarding the safety and efficacy of MIPD. Most institutions performing this complex operation are diverse, low volume centers at the beginning of the learning curve without established MIPD programs, the patient populations and indications for operative management are heterogeneous as are the expertise of the operating surgeons and facilities.
AIM
This article will review the available data from high volume centers with established MIS-PD programs (>40 completed MIPD), and who are assumed to have moved beyond the learning curve to determine if the benefits of MIS, including both laparoscopic and robotic surgery, are extended to the PD [9-14]. In addition to evaluating the safety and efficacy of MIPD, we report our own institutional unpublished data from our first 50 MIPD and again comment on the learning curve for this complex procedure.
METHOD
A comprehensive literature search was performed of the PubMed database for articles containing case series in which at least 40 MIPD had been performed in a single institution between the years of 1994-2015. MIPD was defined as a completely laparoscopic or robotic dissection and resection of the head of the pancreas/duodenum/ porta hepatis, followed by a completely intracorporeal reconstruction of the pancreatic, biliary and intestinal tract. Hybrid procedures in which part of the dissection or reconstruction was extracorporeal or through a “minilaparotomy” were not included. These articles were then reviewed for information regarding peri-operative, postoperative and oncologic outcomes.
INCREASED INTEREST
The desire to broaden the benefits associated with MIS appears to have sparked interest in its application to PD. In a recent analysis of the NCDB by Adam et al. found that the use of MIPD for primary pancreatic adenocarcinoma increased by 45% (179 cases) between 2010-2011. While there are many reports of the technical feasibility of performing this challenging procedure, there remains a paucity of data to demonstrate that it is not only a different approach but also one that offers significant advantages.
OUTCOMES COMPARISON: MIS vs. OPEN PANCREATICODUODENECTOMY
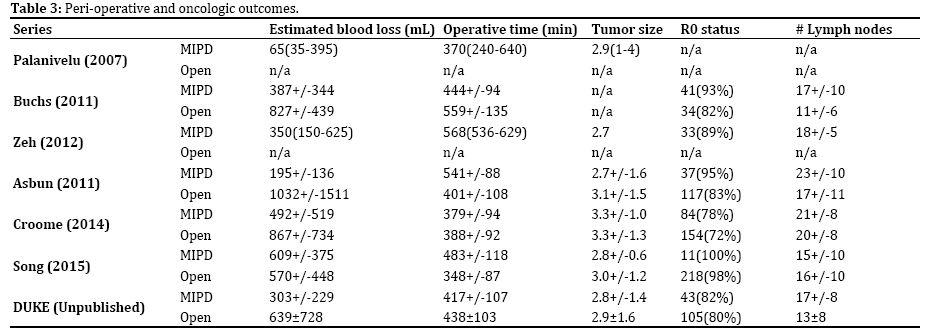
MIS approaches provide improved intraoperative illumination and magnification resulting in an enhanced view allowing for more meticulous dissection- this translates into significantly less estimated blood loss in all series where an open control was available. Most retrospective studies document a longer operative time for MIPD compared to open counterparts. In our selected series of 6 institutions (Table 1) who have performed over 40 MIPD the results are mixed: Palanivelu documents a significantly increased operative time, whereas Kendrick shows equivalent times and Buchs’ series shows decreased operative time when using the MIS approach. These results provide insight into the importance of patient and tumor related factors that institutions and individuals who have surpassed the learning curve may factor into performing a PD.

Clinically significant complications such as delayed gastric emptying (DGE) (grade B/C) and pancreatic fistula (grade B/C) formation appear to be comparable between open and MIS groups. However, in the Croome cohort the patients treated with MIS had a significantly lower rate of DGE (9 vs. 18%). Although reoperation rates appeared higher in the open groups (Asbun et al. 7 vs. 3.8% and Buchs et al. 12.8 vs. 4.5%) this was not statistically significant. 90-day mortality rates were also comparable to open groups when this data was available for comparison, otherwise the rates of 1-5% (Table 2). In our series of 50 patients there were 4 who required reoperations within 30 days of the index MIPD, the reasons for re-operation were multifactorial: 1 patient was placed on ECMO after returning to the ED 8 days post discharge with sepsis from a primary pneumonia and likely abdominal source, 2 patients required operative debridement and placement of wound vacuum assisted closure devices on POD 7 and POD 30, one final patient was brought back to the OR on POD 2 for a diagnostic laparoscopy for a bile leak – an operative drain was left and a transhepatic drain placed by radiology subsequently led to closure of the bile leak from the hepatico-jejunostomy. This equivalent mortality between open PD and MIPD in high volume centers highlights the importance of a dedicated program and team for complex procedures such as MIPD, in the NCDB review by Adam et al. 30-day mortality was significantly increased in MIPD patients vs. open (OR=1.87, confidence interval (CI): 1.25- 2.80, p=0.002), in this series the majority of institutions captured (53%) were low volume centers that performed 10 or less cases/2 years. In this same study although not statistically significant hospital case volume for MIPD tended towards an inverse association with 30-day mortality (OR=0.69, CI 0.46-1.05, p= 0.09).
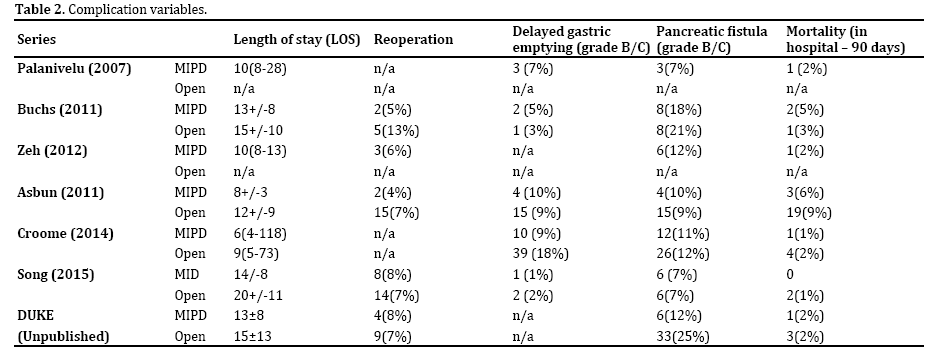
Length of stay as a metric for outcomes is difficult to interpret in these series. Aside from potential bias in patient selection, there is insufficient data on discharge criteria as well as enhanced recovery after surgery protocols which may be in place. Many reports have documented decreased pain on a subjective questionnaire, decreased narcotic requirements, early return of bowel function, and earlier time to flatus. In our analysis of these 6 high volume centers, in the 3 studies where information was available, the LOS was significantly shorter in the MIPD groups vs. open.
Oncologic outcomes variables are also difficult to interpret from these series, as the primary indication for operative management was heterogeneous between studies and groups within each study. However, some generalizations can be made, the rate of R0 status in cases where the indication was for malignancy was unchanged between approach groups, however the number of lymph nodes harvested was significantly increased in most studies aside from Croome et al. 2014 and Song et al. 2015 (Table 3).
LEARNING CURVE
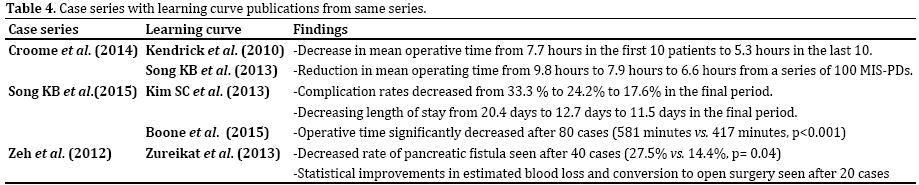
As adoption of MIS for colonic and gastrointestinal surgery has become more widely accepted so has the realization that as for any new endeavor a learning curve, and the ability for incremental improvements over time and experience exist [15]. The concept of a learning curve for any surgical procedure correlates well with the reservoir of literature supporting volume-outcomes relationships, particularly those described for open PD [16]. The traditional surgical learning curve is described as having three portions: a slow and challenging beginning, followed by a steep acceleration phase with rapid progression, and finally a plateau phase associated with continued subtle improvements over time. Several of the authors in the above publications who have documented large series of MIS-PD [17-20], including our own institution’s published series [21], have proceeded to document improvements in outcome variables with increasing experience (Table 4).
Published data from our own institution support the ability of dedicated institutions and surgeons to overcome the significant hurdles that are represented by the MIS-PD learning curve, in particular we documented a significant reduction in operative time after the first ten patients (478.5 min vs. 430.5 mins; p=0.01) [21].
A significant learning curve exists for MIPD, high volume institutions with dedicated surgeons and teams are able to surpass the initial, occasionally arduous, beginning phase and accelerate through the steep learning curve yielding measurable and statistically significant improvements in both peri-operative and post-operative outcomes. Centers that cannot support the volume needed to surpass the learning curve may be able to document the feasibility of the technique but not the potential benefits; in fact there is evidence that low volume centers may have significantly worse peri-operative and post-operative outcomes.
TEACHING THE MINIMALLY INVASIVE PANCREATICODUODENECTOMY
While data from high volume institutions document both safety, efficacy and therefore feasibility of a MIPD program, for this approach and the potential benefits therein to be more widely adopted and sustained this technique must also be transferable to others. To implement MIPD as part of our surgical training program we have modularized the steps in the MIPD procedure into beginner, intermediate, advanced, and expert portions that are divided amongst appropriate level trainees. Figure 1 summarizes our previously published modular and step-wise method for teaching the minimally invasive pancreaticoduodenectomy [21].
Figure 1. Teaching the Minimally Invasive Pancreaticoduodenectomy
[21].
The MID-PD program at Duke University Hospital began in 2010 – the program was modular in approach with the initial first 25-50 cases performed as hybrid procedures in which the exposure, mobilization and dissection was laparoscopic and the reconstruction performed through a ‘mini-laparotomy’ as the usual OPD reconstruction. The reason for this was multifactorial: patient safety - as we left the most technically challenging composnents of the operation to the familiar standard open technique and surgeon fatigue and operative times remained reasonable with this approach.
Although there were no specific pre-operative selection criteria for patients to be eligible for MIS PD – in patients with evidence of vascular involvement at the time of exposure and dissection this mandated a conversion to open for both safety and oncologic reasons. These considerations were made abundantly clear to the patients in whom MID-PD was offered: if at any time there was the possibility that the MIS approach was compromising patient safety or oncologic principles we would convert to open, patients were likewise free to opt for a standard OPD if they wished. In all the initial 25 cases, two attendings were present at all times – an MIS-foregut surgeon with expertise in gastric and pancreatic surgery (AP) and another attending with expertise in open pancreatic surgery (TP, DT, BC, RW). Trainees were involved at all stages: because of our modular approach to the MIS-PD portions of each case were divided between trainees at all levels from port placement for interns, laparoscopic cholecystectomy for juniors, laparoscopic gastro-jejunostomy and hepaticojejunostomy for senior residents and fellows – with the pancreatico-jejunostomy reserved for attending’s and senior fellows. How the pancreatico-jejunostomy was performed was dependent on the texture of the gland as well as the diameter of the pancreatic duct – in firm glands with a large diameter duct the reconstruction method involved a duct-to mucosa technique with an inner layer of interrupted sutures between the pancreatic duct and a small opening the intestine along with an outer layer of interrupted sutures between the pancreatic capsule and the full thickness of the intestine. In cases were the gland was soft and the pancreatic duct was small an invagination technique was employed with a running suture to the entire cut edge of the pancreas and the intestine.
Based on our experience from the first 50 MIPD – the first significant hurdle is represented by operative time. In the initial 10 MIPD operative time is significantly longer due to unfamiliarity with the approach, the equipment and basic trouble shooting issues from both surgeons and the operative teams including nursing and anesthesia. After the first 10 MIPD the operative time normalizes to approximate OPD. Within the following 40 cases improvements in operative time, blood loss, and complications continue but seem to plateau with less marked difference, however gradual improvements do persist.
The capacity to support and grow a MIPD program is dependent on the ability of the institution to overcome a significant learning curve for a technically challenging operation. Over the past 5 years we have navigated and experienced this process- a time and resource consuming endeavor but ultimately an important intervention that we believe may offer benefit to carefully selected patients. Our experience has led us to reflect on several key points that have been important in our success:
A staged and modular approach: we began with a hybrid approach where initially only the mobilization, exposure and dissection were done laparoscopically and the reconstruction was performed in the open manner. Over time this was transitioned to a TLPD as we navigated the learning curve. Furthermore dividing portions of the case between multiple attending’s and trainee’s allows for maximal exposure and sharing of expertise.
Initially all cases involved 2 attendings with a team approach: one with expertise in minimally invasive foregut surgery and another trained in open pancreatic surgery. This pairing we believe, allows for maximum synergy, minimal redundancy, highest patient safety profile, and ensures the needed volume of cases.
In the 5 years since the MIPD program began 2 fellows (SZ and KS) who were trained in this era have begun practicing as attending’s here at Duke and currently perform MIPD independently. During their training they had been exposed to every modular component of the MIPD multiple times either as the operating surgeon or the assistant and were able to safely perform the entire MIPD by the end of their training.
LIMITATIONS
As with any retrospective single center studies the possibility of selection bias exists. Specifically the findings of lower operative blood loss and higher rates of R0 resections between open and MIPD groups comes with the caveat that in most centers MIPD patients are highly selected for vascular involvement and tumor size. Lack of adequate matching within these high volume series makes generalizations from this data at high risk for confounding. Furthermore, information regarding length of hospital stay is difficult to interpret, as discharge criteria vary widely between institutions and the adoption of “Enhanced Recovery After Surgery” protocols is heterogeneous.
The significantly increased lymph node retrieval seen with MIPD is an important indicator of oncologic feasibility of the MIS approach; however this must be taken with consideration of the importance of pathologic processing techniques and standard practices within institutions such as neoadjuvant therapy. Without standardization and reproducibility between institutions these findings are at risk for institutional bias.
While the findings of equivalent operative times and mortality appear in high volume centers, the majority of cases of MIPDs are actually performed in low volume centers. Therefore the experiences documented in this review are not generalizable for this procedure at large. Another possible limitation of this review is publication bias in which centers that have experience with MIPD but who have negative outcomes may be more hesitant to publish these findings.
FUTURE
A small cohort of surgeons at large volume centers has largely driven the enthusiasm for MIPD. This enthusiasm has been tempered by the acknowledgement of a significant learning curve, however there is no reason to believe that indications for MIS techniques will not eventually expand to PD. Published data from multiple high volume centers support equivalent outcomes and potential benefits in selected patients.
As experience is accrued patient selection criteria may be broadened. For instance MIPD with MIS vascular reconstruction has been shown to be feasible and safe in a series by Croome et al. [22]. In this series the authors compared 31 MIPD with laparoscopic vascular resection with 58 patients undergoing open surgery with vascular resection. There were no statistically significant differences between groups in terms of total number of complications, severe complications, 30-day mortality and patency of the reconstructed vessels on post-operative imaging.
As long-term data continues to mature important potential advantages may become evident. In a retrospective institutional review for PDs performed for primary adenocarcinoma of the pancreatic head [11] found that open patients as compared to MIPD patients were more likely to have a >90 day delay to initiation of adjuvant therapy or else to not receive adjuvant at all (12% vs. 5%, p=0.04). These numbers are important as time to adjuvant and completing adjuvant has been shown to prolong survival in pancreatic cancer. Furthermore, the authors were able to show a significantly longer progression-free survival between MIPD and open groups (p=0.02). These studies suggest that as experience and long term data expands indications for MIPD as well as potential benefits from a MIS approach will also increase.
Importantly, several groups including our own are in the process of designing or analyzing quality-of-life measures post operatively between MIPD and open PD groups. In a disease process where the rate of definitive cure is rare, prolonged survival benefits may be modest, and morbidity from the disease and the treatments themselves significantly adversely affect the patient, any incremental improvement in care should be sought. With this in mind, we believe our own data as well as data from several other high volume centers support the use of MIPD in selected patients in specialized centers.
Conflict of Interests
Authors declare no conflict of interests for this article.
References
- Katz MH, Hu CY, Fleming JB, Pisters PW, Lee JE, Chang GJ. Clinical calculator of conditional survival estimates for resected and unresected survivors of pancreatic cancer. Arch Surg 2012; 147:513-9. [PMID: 22351874]
- Correa-Gallego C, Dinkelspiel HE, Sulimanoff I, Fisher S, Viñuela EF, Kingham TP, Fong Y, et al. Minimally-invasive vs. open pancreaticoduodenectomy: systematic review and meta-analysis. J Am Coll Surg 2014; 218:129-39. [PMID: 24275074]
- Honda G, Kurata M, Okuda Y, Kobayashi S, Sakamoto K, Takahashi K. Laparoscopic pancreaticoduodenectomy: taking advantage of the unique view from the caudal side. J Am Coll Surg 2013; 217:e45-9. [PMID: 24051066]
- Clinical Outcomes of Surgical Therapy Study Group. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 2004; 350:2050-9. [PMID: 15141043]
- Colon Cancer Laparoscopic or Open Resection Study Group, Buunen M, Veldkamp R, Hop WC, Kuhry E, Jeekel J, Haglind E, et al. Survival after laparoscopic surgery versus open surgery for colon cancer: long-term outcome of a randomised clinical trial. Lancet Oncol 2009; 10:44-52. [PMID: 19071061]
- Kooby DA, Hawkins WG, Schmidt CM, Weber SM, Bentrem DJ, Gillespie TW, Sellers JB, et al. A multicenter analysis of distal pancreatectomy for adenocarcinoma: is laparoscopic resection appropriate? J Am Coll Surg 2010; 210:779-85, 786-7. [PMID: 20421049]
- Gagner M, Pomp P. Laparoscopic pylorus-preserving pancreatoduodenectomy. Surg Endosc 1994; 8:408-10. [PMID: 7915434]
- Abdelgadir Adam M, Choudhury K, Dinan MA, Reed SD, Scheri RP, Blazer DG 3rd, Roman SA, et al. Minimally invasive versus open pancreaticoduodenectomy for cancer: practice patterns and short-term outcomes among 7061 patients. Ann Surg 2015; 262:372-7. [PMID: 26158612]
- Palanivelu C, Jani K, Senthilnathan P, Parthasarathi R, Rajapandian S, Madhankumar MV. Laparoscopic pancreaticoduodenectomy: technique and outcomes. J Am Coll Surg 2007; 205:222-30. [PMID: 17660068]
- Asbun HJ, Stauffer JA. Laparoscopic vs. open pancreaticoduodenectomy: overall outcomes and severity of complications using the Accordion Severity Grading System. J Am Coll Surg 2012; 215:810-9. [PMID: 22999327]
- Croome KP, Farnell MB, Que FG, Reid-Lombardo KM, Truty MJ, Nagorney DM, Kendrick ML. Total laparoscopic pancreaticoduodenectomy for pancreatic ductal adenocarcinoma: oncologic advantages over open approaches? Ann Surg 2014; 260:633-8; discussion 638-40. [PMID: 25203880]
- Song KB, Kim SC, Hwang DW, Lee JH, Lee DJ, Lee JW, Park KM, Lee YJ. Matched case-control analysis comparing laparoscopic and open pyloruspreserving pancreaticoduodenectomy in patients with periampullary tumors. Ann Surg 2015; 262:146-55. [PMID: 25563866]
- Buchs NC, Addeo P, Bianco FM, Ayloo S, Benedetti E, Giulianotti PC. Robotic versus open pancreaticoduodenectomy: a comparative study at a single institution. World J Surg 2011; 35:2739-46. [PMID: 21947494]
- Zeh HJ, Zureikat AH, Secrest A, Dauoudi M, Bartlett D, Moser AJ. Outcomes after robot-assisted pancreaticoduodenectomy for periampullary lesions. Ann Surg Oncol 2012; 19:864-70. [PMID: 21947670]
- Schlachta CM, Mamazza J, Seshadri PA, Cadeddu M, Gregoire R, Poulin EC. Defining a learning curve for laparoscopic colorectal resections. Dis Colon Rectum 2001; 44:217-22. [PMID: 11227938]
- Hardacre JM. Is there a learning curve for pancreaticoduodenectomy after fellowship training? HPB Surg 2010; 2010:230287. [PMID: 21318116]
- Kendrick ML, Cusati D. Total laparoscopic pancreaticoduodenectomy: feasibility and outcome in an early experience. Arch Surg 2010; 145:19- 23. [PMID: 20083750]
- Kim SC, Song KB, Jung YS, Kim YH, Park do H, Lee SS, Seo DW, et al. Short-term clinical outcomes for 100 consecutive cases of laparoscopic pylorus-preserving pancreatoduodenectomy: improvement with surgical experience. Surg Endosc 2013; 27:95-103. [PMID: 22752284]
- Boone BA, Zenati M, Hogg ME, Steve J, Moser AJ, Bartlett DL, Zeh HJ, et al. Assessment of quality outcomes for robotic pancreaticoduodenectomy: identification of the learning curve. JAMA Surg 2015; 150:416-22. [PMID: 25761143]
- Zureikat AH, Moser AJ, Boone BA, Bartlett DL, Zenati M, Zeh HJ 3rd. 250 robotic pancreatic resections: safety and feasibility. Ann Surg 2013; 258:554-9. [PMID: 24002300]
- Speicher PJ, Nussbaum DP, White RR, Zani S, Mosca PJ, Blazer DG 3rd, Clary BM, et al. Defining the learning curve for team-based laparoscopic pancreaticoduodenectomy. Ann Surg Oncol 2014; 21:4014-9. [PMID: 24923222]
- Croome KP, Farnell MB, Que FG, Reid-Lombardo KM, Truty MJ, Nagorney DM, Kendrick ML. Pancreaticoduodenectomy with major vascular resection: a comparison of laparoscopic versus open approaches. J Gastrointest Surg 2015; 19:189-94. [PMID: 25274069]


