Keywords
Endoscopy; Laparoscopy; Pancreatic Pseudocyst
Abbrevations
EPGS endoscopic pseudocystogastrostomy; LPGS laparoscopic pseudocystogastrostomy; PP pancreatic pseudocysts
INTRODUCTION
Currently surgical approach is frequently used for drainage of pancreatic pseudocysts (PP) [1, 2]. The laparoscopic and endoscopic approaches to internal drainage of PP are the current minimally invasive management options [3, 4]. Even through endoscopic drainage is increasingly performed, there is lack of systematic reviews comparing laparoscopic and endoscopic treatment for PP. So, the decision between endoscopic and laparoscopic approach is still controversial [1]. Indications, early and late results of those approaches are being discussed.
AIM
To present experience in treatment of PP by laparoscopic pseudocystogastrostomy (LPGS) and endoscopic pseudocystogastrostomy (EPGS) and to compare results, feasibility and safety.
MATERIAL AND METHODS
We performed a retrospective analysis of patients, who in period 2008–2015 were diagnosed with PP and underwent surgical treatment. All the PPs had course of disease more than 4 weeks and were surrounded by a well defined wall detected by computed tomography (CT) or transabdominal ultrasonography. Patients, which PPs had connection with pancreatic duct system, were excluded from this study. For cytological and biochemical (a-amylases, carcinoembryonic antigen (CEA)) examination fine needle aspiration biopsy (FNAB) in endoscopic ultrasound (EUS) guidance was performed. Patients diagnosed with malignant process (CEA>192 and atypical cells) were excluded from further investigation. Repeated examination of PP fluid (cytological, biochemical, microbiological) was made during operation. Patients were divided in two groups according to performed drainage procedure of PP. First group - LPGS, second– EPGS. Patients diagnosed with large diameter, multilocular or with necrotic debris cysts were managed by LPGS. Other patients underwent EPGS. Groups were compared by age, gender, pancreatic pseudocyst’s age, diameter and localization, as well as intraoperative, early and late postoperative complications.
Statistical analysis was performed using SPSS 17.0 software (IBM SPSS Inc., Chicago, IL, USA). Descriptive data are reported as means, standard deviations or range. Continuous data were compared with t-test analysis and categorical data were analyzed by Fisher’s exact test. P<0.05 was considered as statistically significant.
Technique of Laparoscopic Pseudocystogastrostomy
The LPGS technique was described in detail previously by Šileikis et al. [5]. Surgeries were performed under general anaesthesia. Four trocars were introduced in to abdominal cavity. Abdominal cavity was inspected with laparoscope. The laparoscopic ultrasound (LUS) were used to confirm localization of PP and it’s relation with stomach. Then, gastrotomy of anterior wall was performed. With laparoscopic needle under LUS control PP‘s fluid sample was collected for examination. The anterior wall of stomach was sutured with abdominal wall for support. Cystogastrostomy between posterior wall of stomach and adherent anterior wall of PP was created using the ultracision scalpel. After necrosectomy and content aspiration, the cavity of PP was inspected. The anterior gastrotomy was closed by single sutures. Through the nasogastric tube methylene blue was injected to check quality of sutures. If needed, additional sutures was made. All trocars wounds were sutured.
Technique of Endosc opic Pseudocystogastrostomy
All the procedures were performed under intravenous or endotracheal anesthesia. After the PP’s bulge was located and its apex was identified by using endoscopic ultrasound (EUS), the intervention started with papillotome needle puncture. Fluid content of the PP was aspirated for examination and then the gastric wall was dilated up to 15 mm using a guidewire balloon. Revision of PP cavity was performed with endoscope via gastric wall if necrotic debris was suspected in cyst lumen on EUS and it was removed with Dormia basket. Then, two double pigtailed catheters were passed into the PP over the wire to facilitate the drainage of PP’s content into the stomach. In some cases (when cyst lumen infection was suspected) additional nasocystic drainage was created near the cystogastric catheters to promote every day washing of cyst lumen for 7 days.
RESULTS
Out of sixty-three patients, who were involved in waiting list for surgical treatment of PP, 14 (22.2%) patients were assigned to LPGS (group I) and 49 (77.8%) patients to EPGS (group II). Table 1 summarizes comparison of groups. In group I–71.4% of patients were men, in group II the dominating gender also were men - 63.3%, p=0.58. There were no significant age difference between group I and II, p=0.97. In both groups majority of patients had chronic pancreatitis (mainly caused by increased alcohol consumption): group I–71.4% of patients, group II–85.7%, p=0.31. Most PP’s were diagnosed by CT scan: in group I–92.9% of cases, in group II - 87.8%. Bigger average cists diameter (the biggest dimension)
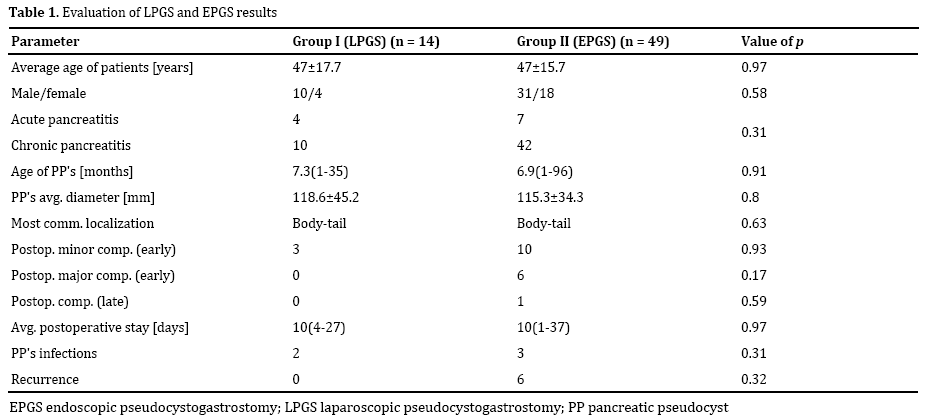
where in group I–118.6 ± 45.2 mm, but the difference was not significant, p=0.8. In group I average thickness of PP wall was 4.8 mm. Average time between diagnosis and operation performance–7.3 ± 19.6 month in group I and 6.9 ± 12.2 month in group II, p=0.91. Necrotic debris during operation was found in 11 of our patients (78.6%) in group I. In both cases most common location of PP were in the body and tail of pancreas–35.7% in group I and 40.8% in group II, p=0.63. After examination of fluid sample, infection were diagnosed to 2 (14.3%) patients in group I and to 3 (6.1%) patients in group II, p=0.31. There were no intraoperative complications, no conversions, no deaths neither I nor in II group. Average time of operation in group I was 145 ± 37.6 min. Early postoperative complications were divided into two groups: minor and major. In group I–21.4% of patients had early minor complications (postoperative hemorrhage which required endoscopic haemostasis and haemotransfusion), but no major, whereas in group II–12.2% of patients had some major complications (peritonitis and suppuration of PP, open surgical interventions were needed). Average postoperative stay in both groups were same–10 days, p=0.97. For 2% of patients in group II late postoperative complications (later than 21 day after intervention) appeared (infection of PP content, additional pseudocytogastrostomy or nasocystic drainage was needed). During 12 months of follow-up period there were no recurrence in group I, whereas in group II recurrence PP appeared in 12.2% of patients, p=0.32.
DISCUSSION
The first documented description of a PP can be ascribed to Morgagni in 1761 [6]. Friedrich Wilhelm Wandesleben performed surgical drainage of a traumatic pancreatic pseudocyst in November 1841 and this operation should be acknowledged as the world’s first reported operation on the human pancreas [7]. The first pseudocystogastrostomy was performed in 1921 [8]. The laparoscopic and endoscopic approaches have played a significant role in the surgical management of pseudocysts with excellent outcomes [1, 9]. The first laparoscopic pseudocystogastrostomy was performed in 1991 [5]. Endosc opic approach treatment of PP is known for more than thirty years. EUS-guided pseudocyst drainage was first described in 1992. Since 2003, when Giovannini et al. reviewed the safety of EUS-guided cystogastrostomy, its acceptance has grown and it is now the preferred method of endoscopic drainage based on documented safety and efficacy [10].
A PP is a complex entity with multiple characteristics, each of which may dictate one method of treatment over another [6]. According to European Society of Gastrointestinal Endoscopy (ESGE) guidelines (2012) - endoscopic therapy as the first-line therapy for uncomplicated chronic PPs for which treatment is indicated and that are within endoscopic reach [11]. A major limitation of endoscopy in the past was that only pseudocysts causing a visible luminal compression could be treated successfully, resulting in technical success rates of 50-60%. However, with the advent of EUS, even pseudocysts not causing a luminal compression can be identified and drained under real-time imaging guidance [12]. Endosc opic intervention for transmural drainage is feasible when a favorable anatomical situation is present such as a common wall between the PP and the stomach/ duodenum, absence of varices and distance between PP and gastric wall must be less than 1 cm (without EUS), but then using EUS this distance can be even more then 1 cm [13, 14]. Aljarabah et al. hold that endoscopic drainage is more suitable for chronic PP within the head and body of the gland, whereas acute PP with walled of necrosis, are more appropriate to manage with laparoscopic surgery [3]. An existing communication between the PP and the pancreatic ductal system allows endoscopic transpapillary drainage [1]. Sheng et al. state that endoscopic drainage is associated with a high rate of technical failure, PP recurrence, infection, bleeding, stent blockage and inadequate drainage [15]. The major complications of EPGS include immediate or delayed infection (0-8%), bleeding (0-9%), retroperitoneal perforation (0-5%) and stent displacement (4-6.5%) [14]. In our data out of 49 patients who underwent EPGS, 6 (12.2%) had PP infection in the early postoperative period and one in the late postoperative period (later than 21 day after intervention). Recurrence, secondary infection or even sepsis with the endoscopic approach may be explained in part by inadequacy of the size of the stoma created endoscopically, with subsequent blockage or displacement of stents, particularly in patients with acute rather than chronic PP [3, 16]. In our data, we had 6 (12.2%) recurrence cases during 12 months of follow-up. Furthermore the endoscopists are less equipped to deal with bleeding than the laparoscopic surgeon, who has a wider access to a range of options such as suturing, the ultrasonically activated scalpel, vascular endostaplers, endoclips and hemostatic thrombin [3].
A pseudocystogastrostomy through laparoscopic approach becoming more common, as experience grows with minimally invasive techniques [17]. With the availability of advanced imaging systems and cameras, better hemostatic equipment and excellent suturing skills, most PP can be approached and managed by a laparoscopic approach [18]. There are several different laparoscopic procedures for PP treatment: pancreatic pseudocystogastrostomy, pseudocystoduodenostomy and pseudocystojejunostomy. Out of all transgastric approaches, anterior gastrostomy is associated with better morbidity and mortality rates and shorter operative time [1, 19, 20]. Laparoscopy seems to have a distinct advantage over endoscopic drainage, because the complete removal of necrosis is possible as well as a wide cystogastrostomy opening [20]. Surgery, either laparoscopic or conventional, may be preferable when adjunctive procedures such as cholecystectomy need to be performed. In fact, in one series more than 50% of patients had gallstone pancreatitis necessitating laparoscopic or open cholecystectomy [6]. Although some advocate routine suturing of the pseudocystogastrostomy to prevent postoperative bleeding, others have not found this to be routinely necessary and have not encountered postoperative bleeding [19, 21]. We report 3 (21.4%) cases from 14 of early postoperative bleeding from pseudocystogastrostomy. Routine suturing of pseudocystogastrostomy was not used. In a systematic review of the literature, laparoscopic drainage was associated with lower morbidity, rapid recovery and lower recurrence rates in compare with open surgery [19]. During 12-month follow-up we did not have any case of cyst recurrence. So LPGS is reported to be feasible, highly effective and safe treatment method [9, 20, 21]. Nevertheless, laparoscopic approach has technical limitations. In our experience we had two cases, when PP was very large (22–24 cm in diameter) and manipulations with laparoscopic instruments were not possible, because of the lack of space, and therefore surgical conversion to laparotomy was needed. Furthermore even being small some PPs can be symptomatic. For those intraoperative identification and selection of cystogastrostomy place can be complicated.
The experience of our clinic showed, that recently endoscopic approach is used more frequently then laparoscopic. This is influenced by increased experience and technical capabilities of EPGS: dilatation of pseudocyctogastrostomy, revision of PP cavity, removal of necrotic debris and possibility of transpapillary stenting. Even, EPGS patients had more early and late postoperative complications, those complications were easy to control (in most of the cases were enough of endoscopic haemostasis). Despite greater number of PP recidivation during 12 months of follow-up, EPGS is cheaper, has a shorter operation time and same hospitalization time in compare with LPGS [22].
This study has some limitations which have to be pointed out. First of all, retrospective nature of research. Therefore the underlying criteria that led to the choice of specific surgical technique could not be strictly defined. This is reflected in our received data of both groups. Second, there was small sample size. Third, number of patients in both groups was different.
CONCLUSION
We have found that both methods to be feasible, effective and safe. Endosc opic treatment should be stated as the first choice treatment approach for patients with pancreatic pseudocyst and only then it fails, LPGS should be performed.
Conflict of Interest
The authors declare that they have no competing interests.
References
- Zhao X, Feng T, Ji W. A systematic review of endoscopic versus surgical treatment for pancreatic pseudocyst. Dig Endosc 2015. [PMID: 26331472]
- Pan G, Wan MH, Xie K-L, Li W, Hu W-M, Liu X-B, et al. Classification and Management of Pancreatic Pseudocysts. Medicine 2015; 94:e960. [PMID: 26091462]
- Aljarabah M, Ammori BJ. Laparoscopic and endoscopic approaches for drainage of pancreatic pseudocysts: a systematic review of published series. Surg Endosc 2007; 21:1936-44. [PMID: 17717626]
- Makarewicz W, Kaska L, Stefaniak T, Kobiela J, Sledzinski Z. Videoscopic procedures in gastrointestinal and endocrine surgery. Wideochirurgia i inne techniki maloinwazyjne 2006; 2:87-93.
- Šileikis A, Beiša A, Elena Z, Saulius J, Strupas K. Minimally invasive management of pancreatic pseudocysts. Videosurgery Miniinv 2013; 8:211–215. [PMID: 24130634]
- Gumaste VV, Aron J. Pseudocyst management endoscopic: drainage and other emerging techniques. J Clin Gastroenterol 2010; 44:326-31. [PMID: 20142757]
- Schnelldorfer T. The birth of pancreatic surgery: a tribute to Friedrich Wilhelm Wandesleben. World J Surg 2010; 34:190-3. [PMID: 19806393]
- Jedlica R. Eine neue Operationsmethode der Pancreascysten (Pancreatogastrostomie). Zentralbl Chir 1923; 50:132.
- Sharma D, Kataria S, Pathak R, Barua B, Lal R. Laparoscopic drainage of a large pancreatic pseudocyst. JSLS 2012; 16:675-7. [PMID: 23484586]
- Nelsen EM, Johnson EA, Walker AJ, Pfau P, Gopal DV. Endosc opic ultrasound-guided pancreatic pseudocyst cystogastrostomy using a novel self-expandable metal stent with antimigration system: A case series. Endosc Ultrasound 2015; 4:229-34. [PMID: 26374582]
- Dumonceau JM, Delhaye M, Tringali A, Dominguez-Munoz JE, Poley JW, Arvanitaki M, et al. ESGE guideline for endoscopic treatment of chronic pancreatitis. Endoscopy 2012; 44:784-796. [PMID: 22752888]
- Varadarajulu S, Bang JY, Sutton BS, Trevino JM, Christein JD, Wilcox CM. Equal efficacy of endoscopic and surgical cystogastrostomy for pancreatic pseudocyst drainage in a randomized trial. Gastroenterology 2013; 145:583-90. [PMID: 23732774]
- Aghdassi A, Mayerle J, Kraft M, Sielenkämper AW, Heidecke CD, Lerch MM. Diagnosis and treatment of pancreatic pseudocysts in chronic pancreatitis. Pancreas 2008; 36:105-12. [PMID: 18376299]
- Wang GX, Liu X, Wang S, Ge N, Guo JT, Liu W, et al. Stent displacement in endoscopic pancreatic pseudocyst drainage and endoscopic management. World J Gastroenterol 2015; 21:2249-53. [PMID: 25717266]
- Sheng QS, Chen DZ, Lang R, Jin ZK, Han DD, Li LX, et al. Laparoscopic cystogastrostomy for the treatment of pancreatic pseudocysts: a case report. World J Gastroenterol 2008; 14: 4841-3. [PMID: 18720552]
- Behrns KE, Ben-David K. Surgical therapy of pancreatic pseudocysts. J Gastrointest Surg 2008; 12:2231-9. [PMID: 18461418]
- Gumbs AA. Video: Laparoscopic anterior cystogastrostomy. Surg Laparosc Endosc Percutan Tech 2010; 20:e97-8. [PMID: 20551804]
- Palanivelu C, Senthilkumar K, Madhankumar MV, Rajan PC, Shetty AR, Jani K, et al. Management of pancreatic pseudocyst in the era of laparoscopic surgery - experience from a tertiary centre. Surg Endosc 2007; 21:2262-7. [PMID: 17516116]
- Hamza N, Ammori BJ. Laparoscopic drainage of pancreatic pseudocysts: a methodological approach. J Gastrointest Surg 2010; 14:148-55. [PMID: 19789929]
- Simo KA, Niemeyer DJ, Swan RZ, Sindram D, Martinie JB, Iannitti DA. Laparoscopic transgastric endolumenal cystogastrostomy and pancreatic debridement. Surg Endosc 2014; 28:1465-72. [PMID: 24671349]
- Abdemur A, Johnson S, Barsoum G, Cappellani A, Zanghì A, Di Vita M, et al. Laparoscopic treatment of intrasplenic pancreatic pseudocyst. Eur Rev Med Pharmacol Sci 2014; 2:24-7. [PMID: 25535187]
- Saul A, Luna MAR, Chan C, Uscanga L, Andraca FV, Calleros JH, et al. EUS–guided drainage of pancreatic pseudocysts offers similar success and complications compared to surgical treatment but with lower cost. Surg Endosc 2015. [PMID: 26139498]

