Keywords
Drug Toxicity; Pancreatitis; Vaginosis, Bacterial
INTRODUCTION
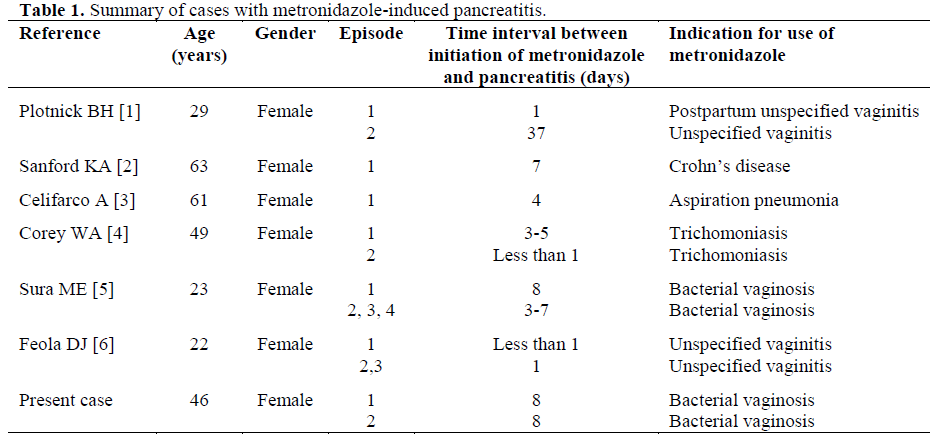
Metronidazole has been widely used to treat various parasitic infections, pseudomembranous colitis, anaerobic infections, acne rosacea, Helicobacter pylori and Crohn's disease. The adverse affects of metronidazole include nausea, anorexia, vomiting, diarrhea, abdominal cramping, neutropenia, metallic taste, urticaria, headache, peripheral neuropathy and a disulfiram-like reaction. Pancreatitis is a very rare adverse effect and only six cases of metronidazole-induced pancreatitis have been reported in the English literature so far (Table 1) [1, 2, 3, 4, 5, 6].
We report a case of recurrent acute pancreatitis associated with oral metronidazole therapy for bacterial vaginosis.
CASE REPORT
A 46-year-old African American female presented to the emergency room with complaints of nausea, vomiting and severe epigastric pain one day after completing a seven day course of metronidazole. She was diagnosed with bacterial vaginosis eight days earlier by her gynecologist and was started on oral metronidazole 500 mg three times a day and was instructed to avoid alcohol consumption. Her past medical history was significant for uterine fibroids and an episode of acute pancreatitis approximately six years ago requiring a 5-day hospitalization. This episode was presumed to be secondary to alcohol use. She reported her alcohol consumption as being 1-2 glasses of wine a week however she denied any alcohol use for the last 2 weeks prior to this admission. Upon further questioning, the patient recalled having an episode of bacterial vaginosis six years ago and then being treated with oral metronidazole. A day after finishing a seven day course of metronidazole she started experiencing nausea, vomiting and abdominal pain and was admitted for acute pancreatitis. At that time the pancreatitis was presumed to be related to alcohol use.
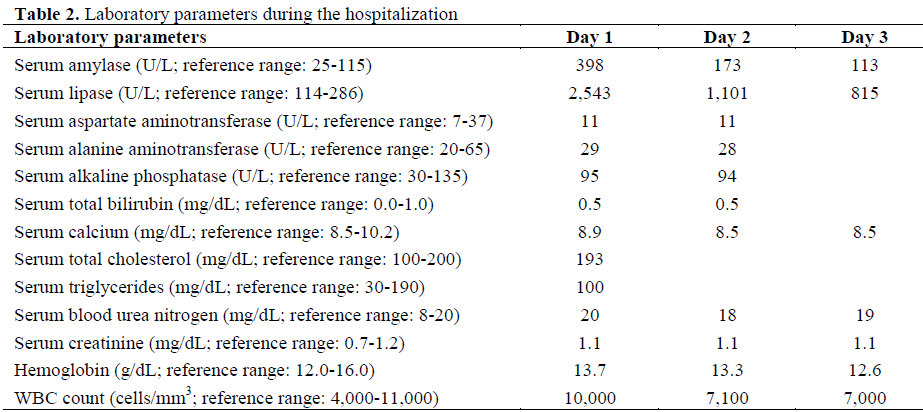
On examination the patient had normal vital signs. The abdominal examination was significant for a mildly distended abdomen with severe epigastric and right upper quadrant tenderness. There was no rigidity or guarding and bowel sounds were normal. There were no palpable abdominal masses. Laboratory parameters are shown in Table 2. The patient was hospitalized for acute pancreatitis. She had an abdominal ultrasound which showed a normal gallbladder and biliary ducts. The patient was treated with intravenous fluids, intravenous hydromorphone and intravenous promethazine. Her symptoms resolved totally by day 2 of hospitalization and she was discharged home on day 4 with instructions to avoid metronidazole in future.
DISCUSSION
Drug induced pancreatitis occurs rarely in clinical practice with only 1.4% of all episodes of acute pancreatitis related to the use of medications. [7]. Proposed criteria for classifying drugs as having an association with pancreatitis [8] include the following:
1) pancreatitis develops during treatment with the drug;
2) other likely causes of pancreatitis are not present;
3) pancreatitis resolves upon discontinuing the drug;
4) pancreatitis usually recurs upon readministration of the drug.
Drugs are classified as having either a definite, probable or possible association with pancreatitis based on the degree to which these criteria are met. Proving a definite association requires that all the criteria mentioned above are met. An association is considered as probable if some but not all of the above mentioned criteria are met.
Our patient developed acute pancreatitis on the day after finishing a seven day course of metronidazole. Past history of a similar episode of acute pancreatitis related to metronidazole use and resolution upon discontinuing metronidazole suggest metronidazole as the most likely etiological agent for pancreatitis in our case. However, since our patient did not undergo evaluation to rule out congenital and genetic causes of pancreatitis, the association between metronidazole use and pancreatitis in our case remains probable.
Only seven cases of metronidazole induced pancreatitis (including this) are described in the English literature (Table 1) [1, 2, 3, 4, 5, 6]. All the cases of metronidazole induced pancreatitis had a moderate and self-limited course. The time lag between metronidazole exposure and development of pancreatitis was very variable; ranging from 12 h to 38 days. Hence it is important to consider metronidazole as a possible etiology for acute pancreatitis in patients presenting with pancreatitis even after a few days of metronidazole exposure. Radiographic abnormalities of pancreas like pancreatic swelling were identified in only 2 out of these 7 cases. None of the reported cases had skin rashes or eosinophilia associated with episodes of pancreatitis. In 6 out of 7 cases there was a rechallenge with metronidazole associated with recurrence of pancreatitis. The lack of alternative effective therapies for trichomoniasis lead to decision to rechallenge one patient with metronidazole [6]; the remaining five incidences of rechallenge (including our case) were due to failure on the prescribing physicians’ part to recognize this potential association between metronidazole use and acute pancreatitis [1, 2, 3, 5 and the present case].
The exact mechanism of metronidazole induced pancreatitis is unknown. Metronidazole, unlike many other antibiotics, penetrates sufficiently into pancreatic tissue to reach therapeutic levels [9]. Suggested mechanisms for metronidazole induced pancreatitis include direct toxic effects of free radicals on pancreatic B cells, immunologic damage to pancreatic ducts and metabolic effects [2, 5].
The management of metronidazole induced pancreatitis consists of standard treatment of pancreatitis with prompt discontinuation of metronidazole. Avoiding rechallenge is an equally important aspect of management.
There are no case reports of acute pancreatitis developing after the use of topical metronidazole and peak serum concentrations of topical metronidazole are significantly less than those of systemic metronidazole [10]. However topical metronidazole has a variable absorption and it is recommended that metronidazole (both systemic and topical), be avoided in patients who develop metronidazole induced pancreatitis to prevent potential complication like acute pancreatitis.
CONCLUSION
Acute pancreatitis is a very rare but potentially serious adverse effect of metronidazole use. Since nausea, vomiting and epigastric distress occur frequently with metronidazole, greater diligence is required on the part of physicians to diagnose metronidazole induced pancreatitis and patients should be informed of this possible reaction. Physicians should consider checking serum amylase and lipase levels for patients who develop nausea, vomiting and epigastric pain upon receiving metronidazole. As the time lag between metronidazole exposure and development of pancreatitis is very variable, it is important to consider metronidazole as a possible etiology for acute pancreatitis in patients presenting with gastrointestinal symptoms even after a few days of metronidazole exposure. If metronidazole is suspected as the causative agent then it should be discontinued and rechallenge should be avoided.
References
- Plotnick BH, Cohen I, Tsang T, Cullinane T. Metronidazole-induced pancreatitis. Ann Intern Med 1985; 103:891-2. [PMID 2415031]
- Sanford KA, Mayle JE, Dean HA, Greenbaum DS. Metronidazole-associated pancreatitis. Ann Intern Med 1988; 109:756-7. [PMID 3263823]
- Celifarco A, Warschauer C, Burakoff R. Metronidazole-induced pancreatitis. Am J Gastroenterol 1989; 84:958-60. [PMID 2756988]
- Corey WA, Doebbeling BN, DeJong KJ, Britigan BE. Metronidazole-induced acute pancreatitis. Rev Infect Dis 1991; 13:1213-5. [PMID 1775854]
- Sura ME, Heinrich KA, Suseno M. Metronidazoleassociated pancreatitis. Ann Pharmacother 2000; 34:1152-5. [PMID 11054984]
- Feola DJ, Thornton AC. Metronidazole-induced pancreatitis in a patient with recurrent vaginal trichomoniasis. Pharmacother 2002; 22:1508-10. [PMID 12432979]
- Lankisch PG, Droge M, Gottesleben F. Drug induced acute pancreatitis: incidence and severity. Gut 1995; 37:565-7. [PMID 7489946]
- Mallory A, Kern F Jr. Drug-induced pancreatitis: a critical review. Gastroenterology 1980; 78:813-20. [PMID 6986321]
- Buchler M, Malfertheiner P, Friess H, Bittner R, Vanek E, Schlegel P, Beger HG. The penetration of antibiotics into human pancreas. Infection 1989; 17:20- 5. [PMID 2921086]
- Lamp KC, Freeman CD, Klutman NE, Lacy MK. Pharmacokinetics and pharmacodynamics of the nitroimidazole antimicrobials. Clin Pharmacokinet 1999; 36:353-73. [PMID 10384859]

