Pancreatic cancer often presents at an advanced stage that result in a very dismal five-year survival rates. Novel methods to detect tumors as early as possible are desperately needed. The U.S. Preventive Services Task Force (USPSTF) recommends against routine screening for pancreatic cancer in asymptomatic adults using abdominal palpation, ultrasonography, or serologic markers. The evidence for diet-based prevention of pancreatic cancer is limited and conflicting. Recommendations about lifestyle changes, such as stopping the use of tobacco products, moderating alcohol intake, and eating a balanced diet with sufficient fruit and vegetables is generally made. However, screening for persons with hereditary predisposition to develop pancreatic cancer has not been included in this review. Biomarkers represent one tool for the early detection of small, surgically resectable cancers in both the general and high risk populations. Some of the currently utilized biomarkers including carcinoembryonic antigen (CEA), CA 19-9, SPan-1, and DUPAN-2 unfortunately have yet to show the sensitivity and specificity needed to be used for screening asymptomatic patients in the general population for pancreatic cancer. Herein, the authors report some updated information from the 2010 ASCO Gastrointestinal Cancers Symposium in detecting early stage pancreatic cancer.
Keywords
Early Detection of Cancer; Endosonography; Mucin-1; Mucins; Pancreatic Neoplasms
Abbreviations
BRCA1: breast cancer 1; BRCA2: breast cancer 2; PRSS1: protease serine 1 (trypsin I precursor)
INTRODUCTION
Pancreatic cancer is a devastating disease. According to data compiled by the American Cancer Society in 2009, there were 42,470 newly diagnosed patients with cancer of the pancreas and 35,240 deaths [1]. The failure to detect cancer at an early stage contributes to the high death rate of this disease. A study involving 799 newly diagnosed pancreatic cancers found only 18% were considered possible for curative resection. There were no 5-year survivors in the 82% where surgical resection was not possible [2]. In Japan, a small study found that among 77 patients undergoing tumor resection, none of the seven patients with tumors under 1 cm had died at the 5-year post-operative follow-up [3]. Despite the potential benefits of surgery, a recent analysis of U.S. data from the National Cancer Data Base (NCDB) found that 51% of patients with resectable stage one pancreatic cancers failed to undergo surgical resection [4]. Because of the potential benefits of removing lesions early, additional screening methods that can assist in correctly diagnosing pancreatic cancer as early as possible are need. The U.S. Preventive Services Task Force (USPSTF) recommends against routine screening for pancreatic cancer in asymptomatic adults using abdominal palpation, ultrasonography, or serologic markers, giving it a grade D recommendation [5].
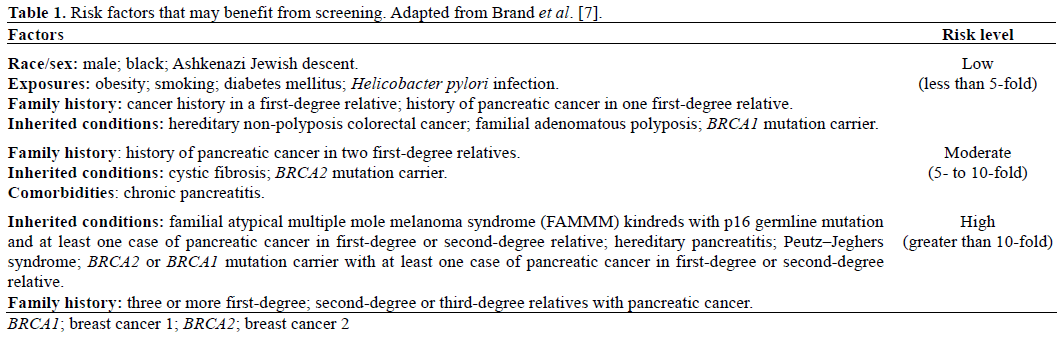
Participants of the Fourth International Symposium of Inherited Diseases of the Pancreas, held in Chicago, IL, USA on November 7-9, 2009 [6], recommend screening only for those at high risk (more than 10-fold relative risk; Table 1) for pancreatic cancer because of the low prevalence of pancreatic cancer in general population [7]. Imaging techniques are frequently used when screening high-risk individuals and include: magnetic retrograde cholangiopancreatography (MRCP/MRI), endoscopic retrograde cholangiopancreatography (ERCP), CT scan, and endoscopic ultrasound (EUS) which, for instance, was able to detect pancreatic cancer in 6.8% of asymptomatic patients at high risk for pancreatic cancer [8]. Other modalities, like biological markers, could help in early diagnosis. Herein we describe work that Gold et al. recently presented at the conference this year (Abstract #135) to determine sensitivity and specificity of a PAM4-enzyme immunoassay for detecting early stage pancreatic cancers (Table 2) [9].

Updates from the 2010 ASCO Gastrointestinal Cancers Symposium
Abstract #135: The PAM4 serum enzyme immunoassay (EIA) for detection of early-stage pancreatic carcinoma
There are many biomarkers currently being looked at for detecting pancreatic cancer in high risk patients or determining the nature of suspicious tumors. Some of the specificity and sensitivities are reported in Table 3.

PAM4 is a purified monoclonal antibody that was generated against mucin collected from the tumor of a RIP1 xenograft and was shown in previous studies to be a marker of early pancreatic adenocarcinoma [10, 11]. In 2009, the group presented the results of additional in vitro immunohistochemistry, and ex vivo enzyme immunoassay (EIA) studies finding 92% of stage I mucinous cystic neoplasm stained strongly with PAM4. Furthermore, this staining correlated with the pathological grade of the lesion [12]. Studies done in 2006 on serum with an EIA to quantitate PAM4 were able to differentiate pancreatic cancer from pancreatitis with a sensitivity of 77% and specificity of 95% [13]. At this year’s conference, the group reports having determined the sensitivity and specificity of EIA for PAM4 in the serum from 68 patients suffering from different stages of pancreatic cancer. In stage I and stage II pancreatic cancer patients, the serum levels of PAM4, determined by an EIA, were able to detect early pancreatic cancer with sensitivity rates of 62% and 86%, respectively. Furthermore, stage Ia (n=13) and stage Ib (n=8) had sensitivities of 54% and 75% for detecting pancreatic cancer, respectively. The overall sensitivity and specificity for detecting all grades of pancreatic cancer compared to healthy controls were 81% and 95%, respectively.
Discussion
Since the detection and resection of early disease is the only real treatment capable of offering cure and long term disease control, developing and validating new biomarkers like PAM4, and then using them for screening, holds much promise to reduce mortality from pancreatic cancer. The development of selective biomarkers also has the potential to be useful for developing selective imaging agents and selective treatments.
With recent advances in human genetics and diagnostic tools, physicians can now offer screening services to those at high risk for developing pancreatic cancer (Table 1). A multifaceted approach for detection and treatment in high risk patients is warranted and is currently being exemplified at our institution. Our team with a special expertise in pancreatic cancer includes an oncologist, gastroenterologist performing endoscopy, pathologists, cancer genetic counselors, and surgeons in addition to ancillary staff. The team makes use comprehensive genetic testing and counseling services and specialized tests including endoscopic ultrasound (EUS), magnetic resonance cholangiopancreatography (MRCP), endoscopic retrograde cholangiopancreatography (ERCP), and computed tomography (CT) scans. It is important to note that not all tests and services are appropriate for everyone, and depending upon individual risk factors and personal history, the recommendations that a patient receives if a suspicious lesion is found will vary. We look forward to the further development of markers such as PAM4 and hope they can be developed and utilized as part of a comprehensive approach to screening of patients at high risk for pancreatic cancer.
Conflict of interest
The authors have no potential conflicts of interest
References
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, ThunMJ. Cancer Statistics, 2009. CA Cancer J Clin 2009; 59:225-49. [PMID 19474385]
- Geer RJ, Brennan MF. Prognostic indicators for survival after resection of pancreatic adenocarcinoma. Am J Surg 1993; 165:68-72. [PMID 8380315]
- Ariyama J, Suyama M, Satoh K, Sai J. Imaging of small pancreatic ductal adenocarcinoma. Pancreas 1998; 16:396-40. [PMID 9548685]
- Bilimoria KY, Bentrem DJ, Ko CY, Stewart AK, Winchester DP, Talamonti MS. National failure to operate on early stage pancreatic cancer. Ann Surg 2007; 246:173-80. [PMID 17667493]
- Agency for Healthcare Research and Quality (AHRQ). Screening for Pancreatic Cancer. Recommendation Statement. U.S. Department of Health & Human Services Washington, DC, USA, 2004.
- Andrén-Sandberg A. 4th international symposium on inherited diseases of the pancreas. November 7-9, 2003, Chicago, Ill., USA. Pancreatology 2003; 3:520-32. [PMID 14752237]
- Brand RE, Lerch MM, Rubinstein WS, Neoptolemos JP, Whitcomb DC, Hruban RH, et al. Advances in counselling and surveillance of patients at risk for pancreatic cancer. Gut 2007; 56:1460-9. [PMID 17872573]
- PoleyJW, Kluijt I, Gouma DJ, Harinck F, Wagner A, Aalfs C, et al. The yield of first-time endoscopic ultrasonography in screening individuals at a high risk of developing pancreatic cancer. Am J Gastroenterol 2009; 104:2175-81. [PMID 19491823]
- Gold DV, Goggins M, Newsome G, Modrak DE, Liu M, Goldenberg DM. The PAM4 serum enzyme immunoassay (EIA) for detection of early-stage pancreatic carcinoma. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 135.
- Gold DV, Lew K, Maliniak R, Hernandez M, Cardillo T. Characterization of monoclonal antibody PAM4 reactive with a pancreatic cancer mucin. Int J Cancer 1994; 57:204-10. [PMID 7512537]
- Gold DV, Karanjawala Z, Modrak DE, Goldenberg DM, Hruban RH. PAM4-reactive MUC1 is a biomarker for early pancreatic adenocarcinoma. Clin Cancer Res 2007; 13:7380-7. [PMID 18094420]
- Gold D, Modrak DE, Newsome G, Karanjawala Z, Hruban R, Goggins M, Goldenberg DM. Detection of early-stage pancreatic carcinoma. J ClinOncol 2009; 27(15 Suppl):Abstract 4613.
- Gold DV, Modrak DE, Ying Z, Cardillo TM, Sharkey RM, Goldenberg DM. New MUC1 serum immunoassay differentiates pancreatic cancer from pancreatitis. J ClinOncol 2006; 24:252-8. [PMID 16344318]
- Ni XG, BaiXF, Mao YL, Shao YF, Wu JX, Shan Y, et al. The clinical value of serum CEA, CA19-9, and CA242 in the diagnosis and prognosis of pancreatic cancer. Eur J SurgOncol 2005; 31:164- 9. [PMID 15698733]
- SimeoneDM, Ji B, Banerjee M, Arumugam T, Li D, Anderson MA, et al. CEACAM1, a novel serum biomarker for pancreatic cancer. Pancreas 2007; 34:436-43. [PMID 17446843]
- Kiriyama S, Hayakawa T, Kondo T, Shibata T, Kitagawa M, Ono H, Sakai Y. Usefulness of a new tumor marker, Span-1, for the diagnosis of pancreatic cancer. Cancer 1990; 65:1557-61. [PMID 2311067]
- Goonetilleke KS, Siriwardena AK. Systematic review of carbohydrate antigen (CA19-9) as a biochemical marker in the diagnosis of pancreatic cancer. Eur J SurgOncol 2007; 33:266-70. [PMID 17097848]
- Koopmann J, RosenzweigCN, Zhang Z, Canto MI, Brown DA, Hunter M, et al. Serum markers in patients with resectable pancreatic adenocarcinoma: macrophage inhibitory cytokine 1 versus CA19-9. Clin Cancer Res 2006; 12:442-6. [PMID 16428484]
- Ishizone S, Yamauchi K, Kawa S, Suzuki T, Shimizu F, Harada O, et al. Clinical utility of quantitative RT-PCR targeted to alpha1,4- N-acetylglucosaminyltransferase mRNA for detection of pancreatic cancer. Cancer Sci 2006; 97:119-26. [PMID 16441422]
- Matsubayashi H, Canto M, Sato N, Klein A, Abe T, Yamashita K, et al. DNA methylation alterations in the pancreatic juice of patients with suspected pancreatic disease. Cancer Res 2006; 66:1208-17. [PMID 16424060]
- Wu X, Lu XH, Xu T, QianJM, Zhao P, GuoXZ, Yang XO, Jiang WJ. Evaluation of the diagnostic value of serum tumor markers, and fecal k-ras and p53 gene mutations for pancreatic cancer. Chin J Dig Dis 2006; 7:170-4. [PMID 16808798]

