Keywords
Acute Disease; Adult; Carcinoma; Carcinoma, Non-Small-Cell Lung; Female; Humans; Lung Neoplasms; Neoplasm Metastasis; Pancreatic Neoplasms; Pancreatitis; Small Cell Lung Carcinoma
INTRODUCTION
A variety of tumors have been reported to metastasize to the pancreas, including prostatic carcinoma, renal cell carcinoma, squamous cell carcinoma of the skin, carcinoma of the breast, hepatoma, a variety of sarcomas, Hodgkin’s disease, small cell lung carcinoma and non-small cell lung carcinoma, and pancreatic metastases are relatively common in advanced small cell lung carcinoma and non-small cell lung carcinoma [1, 2, 3, 4]. Metastasis-induced acute pancreatitis, however, is very unusual. In this report, we documented a case of metastasis-induced acute pancreatitis as an initial manifestation of small cell lung carcinoma, and reported dramatic improvement of the patient’s condition after using chemotherapy to treat the metastases. We concluded that, when cases of acute pancreatitis in patients with small cell lung carcinoma are encountered, the patient should be screened for pancreatic metastases and, if found, these metastases should be treated aggressively.
CASE REPORT
A 51-year-old woman was admitted to Nagoya City University Hospital with severe epigastralgia. She had been smoking 20 cigarettes a day for 30 years. There was no history of excessive alcohol consumption, medication or cholelithiasis. On admission to Nagoya City Hospital, pertinent physical findings were confined to the abdomen, the patient exhibiting abdominal tenderness and guarding over the epigastrium. Laboratory data were as follows: WBC count, 6,100 mm-3 (reference range: 3,000-8,500 mm-3); RBC, 411 x104 mm-3 (reference range: 378-499 x104 mm-3); hemoglobin, 12.6 g/dL (reference range: 10.8-14.9 g/dL); BUN, 10 mg/dL (reference range: 8-22 mg/dL); creatinine, 0.7 mg/dL (reference range: 0.4-0.7 mg/dL); and calcium, 9.4 mEq/L (reference range: 8.7-10.3 mEq/L). The pancreatic enzymes were elevated: serum amylase, 135 U/L (reference range: 37-125 U/L); lipase, 276 U/L (reference range: 13-49 U/L); and elastase-1, 2,000 ng/dL (reference range: 100-400 ng/dL). Urophanic amylase was elevated to 887 U/L (reference range: 0-650 U/L). Small cell lung carcinoma markers were elevated: neuron-specific enolase, 24 ng/mL (reference range: 0-10 ng/mL) and pro-gastrin-releasing peptide, 2,310 ng/mL (reference range: 0-46 ng/mL).
Plain chest X-ray films revealed a left parahilar tumor (Figure 1). Chest computed tomography (CT) showed multiple diffuse parahilar lymphadenopathy and a 44x33 mm mixed density lung mass with irregular margins at the left hilum (Figure 2a). Abdominal US disclosed 1-3 cm multiple low echoic masses within the swollen pancreatic body and tail (Figure 3a). Magnetic resonance imaging (MRI) confirmed the US findings (Figure 4ac), but abdominal CT demonstrated only a swollen pancreas. Because the pancreatic duct was normal in the US, CT and MRI images, the MRCP image was not diagnostic at that time. Bone scintigraphy revealed a hot spot in the right arm. A head MRI was normal. A cytological diagnosis of the sputum revealed small cell carcinoma. Since the acute pancreatic symptom was severe, bronchoscopy, endoscopic retrograde pancreatography and endoscopic US-guided fine needle aspiration biopsy (EUS-FNA) were not performed.
Figure 1. Chest X-ray films revealed a left parahilar tumor (arrow).
Figure 2. a. Contrast-enhanced chest computed tomography showed
ultiple diffuse parahilar lymphadenopathy and a 44x33 mm mixed
density lung mass with irregular margins at the left hilum (arrow). b. After two courses of chemotherapy, the lung tumor disappeared.
Figure 3. a. Abdominal ultrasonography disclosed 1-3 cm multiple
low echoic masses within the swollen pancreas body and tail. b. After two courses of chemotherapy, the pancreas metastatic
tumors disappeared.
Figure 4. a. T1 weighted magnetic resonance imaging (MRI)
confirmed the ultrasonography findings. MRI showed multiple low
intensity masses within the swollen pancreas body and tail. b. After
two courses of chemotherapy, the pancreas metastatic tumors
disappeared in T1-weighted MRI. c. Gadolinium-enhanced MRI
showed multiple low intensity masses. d. After two courses of
chemotherapy, the pancreas metastatic tumors had disappeared in
gadolinium-enhanced MRI.
The patient received conventional treatment of a fasting couplet with an anti-pancreatic exocrine enzyme (gabexate mesylate 600 mg/day) and antibiotics (meropenem, 1 g/day). However, the treatment did not improve her condition. Therefore, ulinastatin (150,000 U/day) was added to her treatment after one week. Still, her condition remained unchanged. Thus, aggressive combination chemotherapy with two courses of PVP-IAV therapy was performed (CDDP+VP16 therapy was modified to PVP-IAV therapy at the Department of Pulmonology in our hospital at the time). PVP and IAV therapy were scheduled alternatively once every 3 weeks. Each procedure was performed twice over the course of 12 weeks. At the time the patient was treated, the standard PVP therapy at Nagoya City University Hospital was cisplatin 36 mg/m2 days 1, 2, 3 plus etoposide 100 mg/m2 days 1, 2, 3, and the standard IAV therapy was ifosfamide 1,500 mg/m2 day 1 plus adriamycin 40 mg/m2 day 1 plus vincristine 1.5 mg/m2 day 1. After two courses of chemotherapy, the lung tumor and the parahilar lymphadenopathy had disappeared on the chest X-ray and CT (Figure 2b). The pancreas metastatic tumors had also disappeared on abdominal US (Figure 3b) and MRI (Figure 4bd). Chemotherapy also caused a rapid and dramatic improvement in her condition and a significant decrease in follow-up amylase levels. The same combination chemotherapy was continued in another hospital near the patient’s home. However, she died due to multiple brain metastatic tumors 8 months after her initial presentation with pancreatitis. Permission for a postmortem was not granted.
DISCUSSION
Prospective confirmation of a diagnosis of metastasis-induced acute pancreatitis is difficult in the absence of EUS-FNA or exploratory laparotomy with pancreatic biopsy. Since permission for a postmortem was not granted, we could not confidently diagnose the pancreatic masses found in this patient as metastases. However, chemotherapeutic treatment for small cell carcinoma was effective against the pancreatic masses of this patient, suggesting that the pancreatic masses were small cell carcinoma. In addition, metastases to the pancreas from small cell lung carcinoma are frequent and are found in 24% of patients at post-mortem [3]; primary small cell carcinoma of the pancreas is very rare, only 1-1.4% of pancreatic cancers [5, 6]. Finally, while 96% of small cell cancers are of pulmonary origin, only about 4% arise in extra-pulmonary sites [7]. Taken together, these data suggest that it is likely that the pancreatic tumors were metastatic small cell lung carcinoma in this patient, and that the acute pancreatitis was induced by these metastases.
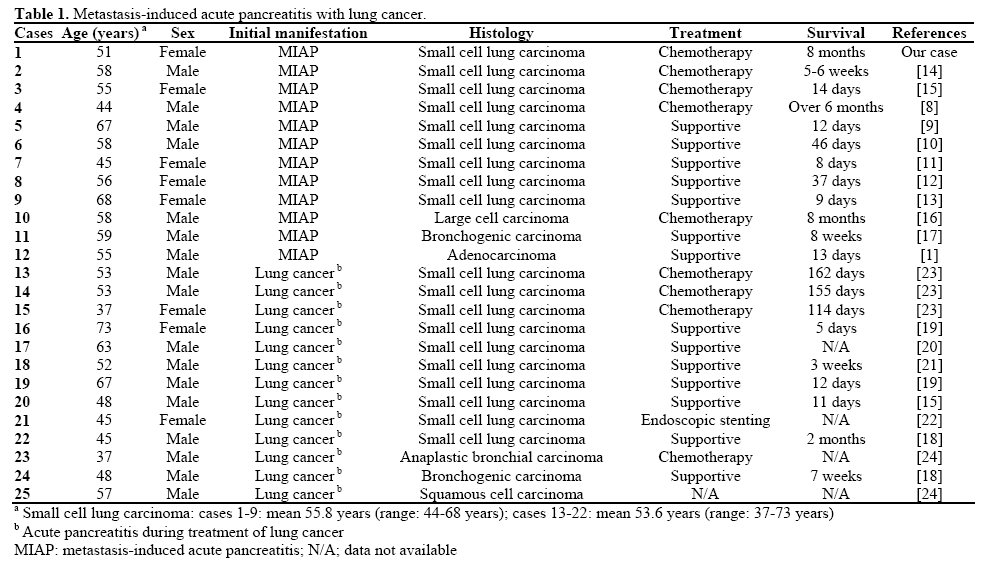
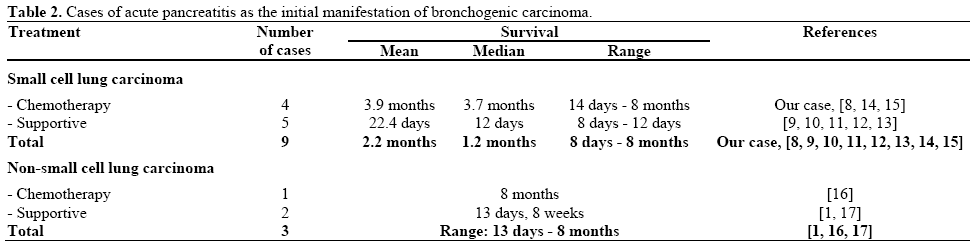
Metastasis-induced acute pancreatitis can occur as an initial manifestation of a carcinoma or later in the course of the disease (Table 1). There are no standard treatment approaches to metastasis-induced acute pancreatitis due to the rarity of this disease and its grim prognosis. Reported survival times range from 8 days to 8 months (the present case) with a mean survival of approximately 2.2 months from the onset of the pancreatitis (Table 2). However, only in the nine cases in which acute pancreatitis manifested as an initial symptom of small cell lung carcinoma [8, 9, 10, 11, 12, 13, 14, 15] did treatment with chemotherapy have a significant effect on patient survival time; patients treated with chemotherapy survived an average of 3.9 months while patients with only supportive therapy survived an average of 22.4 days (Table 2). Perhaps of greater importance, however, the chemotherapeutic treatment of the patient reported here resulted in a rapid and significant regression of her pancreatitis symptoms and a dramatic improvement in her general condition.
Notably, while therapy directed against pancreatic metastases dramatically improved the condition of the patient, the conventional treatment of fasting coupled with intravenous therapy with gabexate mesylate/nafamostat mesilate and antibiotics had no effect on the patient’s condition. We concluded that when cases of acute pancreatitis in patients with small cell lung carcinoma are encountered, the possibility of metastasis-induced acute pancreatitis must be considered and that, should pancreatic metastases be found in these patients, chemotherapy may provide substantial benefit.
Conflict of interest The authors have no potential conflicts of interest
References
- DG Niccolini, JH Graham, PA Banks. Tumor-induced acute pancreatitis. Gastroenterology 1976; 71:142-5. [PMID 1278639]
- T Berge, NG Toremalm. Bronchial cancer - a clinical and pathological study. I. Histopathology and metastases. Scand J Respir Dis 1975; 56:109-19. [PMID 170673]
- DH Line, TJ Deeley. The necropsy findings in carcinoma of the bronchus. Br J Dis Chest 1971; 65:238-42. [PMID 4944570]
- MJ Matthews. Morphology of lung cancer. Semin Oncol 1974; 1:175-82. [PMID 4377934]
- AL Cubilla, PJ Fitzgerald. Classification of pancreatic cancer (nonendocrine). Mayo ClinProc 1979; 54:449-58. [PMID 221755]
- CV Reyes, T Wang. Undifferentiated small cell carcinoma of the pancreas: a report of five cases. Cancer 1981; 47:2500-2. [PMID 6268272]
- RM Levenson, Jr., DC Ihde, MJ Matthews, MH Cohen, AF Gazdar, PA Bunn, Jr., et al. Small cell carcinoma presenting as an extrapulmonary neoplasm: sites of origin and response to chemotherapy. J Natl Cancer Inst 1981; 67:607-12. [PMID 6268879]
- KC Stewart, WJ Dickout, JD Urschel. Metastasis-induced acute pancreatitis as the initial manifestation of bronchogenic carcinoma. Chest 1993; 104:98-100. [PMID 8391965]
- M Hall, NJ Bundred, AW Hall. Oat cell carcinoma of the bronchus and acute pancreatitis. Eur J Surg Oncol 1987; 13:371-2. [PMID 3040475]
- A Noseda, D Gangji, M Cremer. Acute pancreatitis as presenting symptom and sole manifestation of small cell lung carcinoma. Dig Dis Sci 1987; 32:327-31. [PMID 3028735]
- AT Evans. Necrotising pancreatitis and diabetes associated with disseminated small cell carcinoma of lung. Scott Med J 1988; 33:377. [PMID 2854301]
- MI Maclennan AC. Small cell carcinoma induced acute pancreatitis. Br J Radiol. 1993; 66:2. [PMID 8384507]
- YW Huang, JC Yang, YL Chang, YM Tsang, TH Wang. Acute pancreatitis combined with acute Budd-Chiari syndrome as the initial manifestation of small cell lung cancer. J Formos Med Assoc 2005; 104:431-5. [PMID 16037834]
- JK Schmitt. Pancreatitis and diabetes mellitus with metastatic pulmonary oat-cell carcinoma. Ann Intern Med 1985; 103:638-9. [PMID 2994535]
- NM Chowhan, S Madajewicz. Management of metastases-induced acute pancreatitis in small cell carcinoma of the lung. Cancer 1990; 65:1445-8. [PMID 2155057]
- M Gutman, M Inbar, JM Klausner. Metastases-induced acute pancreatitis: a rare presentation of cancer. Eur J Surg Oncol 1993; 19:302-4. [PMID 8390948]
- GR McLatchie, CW Imrie. Acute pancreatitis associated with tumour metastases in the pancreas. Digestion 1981; 21:13-7. [PMID 7227664]
- M Levine, SH Danovitch. Metastatic carcinoma to the pancreas. Another cause for acute pancreatitis. Am J Gastroenterol 1973; 60:290-4. [PMID 4355449]
- SG Allan, N Bundred, O Eremin, RC Leonard. Acute pancreatitis in association with small cell lung carcinoma: potential pitfall in diagnosis and management. Postgrad Med J 1985; 61:643-4. [PMID 2991875]
- KH Kim, CD Kim, SJ Lee, G Lee, YT Jeen, HS Lee, et al. Metastasis-induced acute pancreatitis in a patient with small cell carcinoma of the lung. J Korean Med Sci 1999; 14:107-9. [PMID 10102535]
- A Papagiannis, K Zarogoulidis, D Delis, D Patakas. A 52-year-old man with a lung mass and acute abdominal pain. Chest 2000; 117:894-6. [PMID 10713023]
- JS Woo, KR Joo, YS Woo, JY Jang, YW Chang, J Lee, 2nd, et al. Pancreatitis from metastatic small cell lung cancer successful treatment with endoscopic intrapancreatic stenting. Korean J Intern Med 2006; 21:256-61. [PMID 17249510]
- KY Yeung, DJ Haidak, JA Brown, D Anderson. Metastasis-induced acute pancreatitis in small cell bronchogenic carcinoma. Arch Intern Med 1979; 139:552-4. [PMID 220925]
- K Wernecke, PE Peters, M Galanski. Pancreatic metastases: US evaluation. Radiology 1986; 160:399-402. [PMID 3523591]





