Keywords
Endoscopy ; Pancreatic Pseudocyst
INTRODUCTION
The science behind pancreatitis and its complications is an ever evolving and challenging field. More than two centuries after the first description of pancreatic pseudocyst by Eugene Opie, some clear consensus and guidelines have evolved. Atlanta Symposium in 1992 attempted to offer a global ‘consensus’ and a universally applicable classification system for acute pancreatitis, tough comprehensive; some of the definitions were confusing [1]. Recent data and deeper understanding of pathophysiology of organ failure and necrotising pancreatitis, and the advent of superior diagnostic imaging have propelled towards the formation of revised Atlanta classification in 2012.
Local complications of acute pancreatitis among others are acute pancreatic fluid collection, pancreatic pseudocyst, acute necrotic collection and walled-off necrosis. Rarer complications are gastric outlet dysfunction, splenic and portal vein thrombosis, and colonic necrosis [2].
Pancreatic Pseudocysts
The first description of pancreatic pseudocyst dates back almost two and half centuries to 1761 A.D. [3]. In revised Atlanta classification, collections are defined based on time of onset after acute pancreatitis (before or after 4 weeks) and type of contents of the collection (fluid alone versus solid component with variable amount of fluid). Pancreatic pseudocyst is a delayed; more than 4 weeks complication of interstitial oedematous pancreatitis versus acute peripancreatic fluid collection (APFC) when it is less than 4 weeks. Acute necrotic collection (ANC), is debri containing peripancreatic fluid collection in the early phase before demarcation and walled-off necrosis (WON), which is surrounded by a capsule usually occurs after 4 weeks of severe pancreatitis [2].
A disruption of the main pancreatic duct or its intrapancreatic branches in the absence of necrosis is crucial for the formation of pancreatic pseudocyst (Figure 1). The persistent leakage of pancreatic juice results in a persistent and localised fluid collection, usually after 4 weeks of the acute event. In acute necrotising pancreatitis, a pseudocyst with debri develops as a result of a ‘disconnected duct syndrome’ due to presence of a viable distal pancreatic remnant contributed by pancreatic neck or body necrosis [4]. Pseudocysts are formed after acute as well as chronic pancreatitis but more common after acute exacerbations of chronic pancreatitis [5]. The prevalence of pancreatic pseudocysts in acute pancreatitis is 6%-18.5% [6] and about 20%- 40% in chronic pancreatitis [7].
Figure 1. Pancreatic pseudocyst.
Metal Stents in PFC
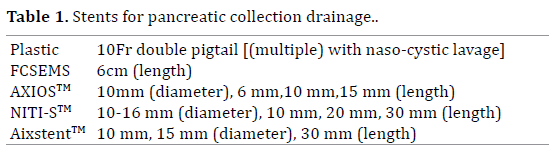
The stents used for drainage of encapsulated PFC has evolved over the years form plastic stents to metals stents and with experience and innovation, specialized stents has made it into current practice (Figure 2). Previously, stents used in interventional EUS was the same as those used in ERCP. Due to the risk of leakage or peritonitis; fully covered self expandable metal stents (FCSEMS) are the preferred choice as opposed to uncovered stents for pancreatic pseudocyst drainage. Double pigtailed plastic stents and FCSEMS are used in uncomplicated pseudocyst drainage. The outcomes of FCSEMS are similar to plastic stents for uncomplicated pseudocyst drainage [8]. Multiple plastic stents with nasocystic lavage used to be the conventional treatment for infected pseudocyst. FCSEMS and specialized stents i.e. Taewong Niti-STM Biliary Stent [Nagi]TM and AXIOSTM (Table 1) have been used lately for infected pseudocyst drainage with good outcome [9].
Figure 2. Specialized pancreatic pseudocyst stent.
Evolution in Management of Pancreatic Fluid Collection (PFC)
The conventional management of PFC were percutaneous drainage under radiologic guidance, conventional transmural drainage (CTD), trans-abdominal US guided endoscopic transmural drainage and open surgical drainage [10, 11]. Since its introduction in 1980’s, EUS guided PFC drainage has superseded other modalities as the treatment of choice for PFC.
23 articles have described metal stent placement in pseudocyst with a pubmed search using ‘pseudocyst’ and ‘metal stent’ as MESH terms. Three were prospective non-randomized trials, four retrospective studies and 16 case series and reports. 11 of these publications used FCSEMS with anti-migration system and 13 others used FCSEMS. The largest prospective study by Walter D et al., 61 patients were followed up: 46 had WON and 15 had pancreatic pseudocyst [12]. The overall technical success rate was 98%. The clinical success rate was 81% and 93% for WON and pseudocyst respectively. Median removal time for a stent was 32 days with five experiencing major complications resulting in migration, dislodgement, infection and perforation. A smaller prospective study by Shah RJ et al. showed 91% technical success and 93% clinical success with minor complications of about 15% [13]. In a series of 148 patients, EUS guided pseudocyst drainage of the uncinate process was more commonly associated with perforation [14]. Pancreatic abscess were associated with higher complications about 30% and lower clinical success [15]. The ability to deploy this stents in a single step process seems to be one of the most crucial favourable points highlighted in these studies.
EUS guided PFC drainage can be done via transgastric, transduodenal, transjejunal (Rouy-en-Y patients) or transesophageal approach (Figure 3) [16, 17]. In a RCT; EUS guided approach compared to surgical cytsogastrostomy showed no superiority of surgery over EUS arm with EUS arm costing half of surgery [18]. A meta-analysis comparing EUS guided PFC drainage and conventional transmural drainage (CTD) involving 299 patients showed no difference in clinical or technical success in both groups but 3 deaths were documented in CTD group [19].
Figure 3. Transgastric pancreatic pseudocyst stent placement
Infected pseudocyst has been managed by open or laparoscopic surgery until two decades ago. In a RCT of 22 patients, endoscopic necrosectomy reduced the proinflammatory response as well as new-onset multiple organ failure, intra-abdominal bleeding, enterocutaneous fistula and death compared to surgical necrosectomy [20]. Endoscopic drainage alone (Figure 4) has not been adequate for this condition while surgical drainage has been reported to have a high morbidity [21]; EUS-guided cyst-enterostomy in combination with nasocystic lavage to flush out necrotic debris was introduced [22]. TENSION-trial, in which 98 patients had endoscopic step-up approach compared with the surgical method is yet to be published [23]. Direct endoscopic necrosectomy (DEN)(Figure 5) was introduced by Seifert et al in 2000; in a retrospective review showed that DEN was associated with good long-term maintenance and high success rate of 80%-88% compared to standard endoscopic drainage [24, 25]. DEN is a safe and effective minimally invasive treatment for infected walled-off pancreatic necrosis and infected pseudocysts. Main outcome predictor was the extent of necrosis and fluid collection [26, 27].
Figure 4. Infected pancreatic pseudocyst with stent in-situ.
Figure 5. Infected pancreatic pseudocyst after DEN.
CONCLUSION
EUS guided PFC drainage is better than open surgical drainage; the success rate is higher with lesser morbidity and cost. Pseudocyst with a bulge can be managed by CTD but pseudocyst without a bulge; EUS guided drainage is safer. A single step approach is better than multistep approach. Metal stents are similar to plastic stents in terms of treatment outcome for uncomplicated pseudocyst but plastic stents have more migrations. Necrotic pancreas management via EUS guided metal stent drainage is safe and can achieve treatment success of up to 81-92%. The use of metal stents in pseudocyst management has caused a significant paradigm shift away from conventional surgical approach. More randomized studies are needed to look at the long term outcome and cost effectiveness of metal stent use in pancreatic pseudocyst management.
Conflict of Interest
The authors declare that they have no conflicts of interest.
References
- Bollen TL, van Santvoort HC, Besselink MG, van Leeuwen MS, Horvath KD, et al. The Atlanta Classification of acute pancreatitis revisited. Br J Surg 2008; 95:6–21. [PMID: ]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut 2012; 62:102–111. [PMID: 23100216]
- Cannon JW, Callery MP, Vollmer CM Jr. Diagnosis and management of pancreatic pseudocysts: what is the evidence. J Am CollSurg 2009; 209: 385-93. [PMID: 19717045]
- Pelaez-Luna M, Vege SS, Petersen BT, Chari ST, Clain JE, Levy MJ, et al. Disconnected pancreatic duct syndrome in severe acute pancreatitis: clinical and imaging characteristics and outcomes in a cohort of 31 cases. Gastro intest Endosc 2008; 68:91–7. [PMID: 18378234]
- Khanna AK, Tiwary SK, Kumar P. Pancreatic Pseudocyst : Therapeutic Dilemma 2012. [PMID: 22577595]
- Maringhini A1, Uomo G, Patti R, Rabitti P, Termini A, Cavallera A, Dardanoni G, et al. Pseudocysts in acute nonalcoholic pancreatitis: incidence and natural history. Dig Dis Sci 1999; 44:1669–73. [PMID: 10492151]
- Barthet M, Bugallo M, Moreira LS, Bastid C, Sastre B, Sahel J. Management of cysts and pseudocysts complicating chronic pancreatitis. A retrospective study of 143 patients. Gastroentérologie Clin Biol 1993; 17:270–6. [PMID: 8339886]
- Bang JY, Varadarajulu S. Metal versus Plastic Stent for Transmural Drainage of Pancreatic Fluid Collections. ClinEndosc 2013; 46:500–2. [PMID: 24143311]
- Fabbri C, Luigiano C, Cennamo V, Polifemo AM, Barresi L, Jovine E, et al. Endoscopic ultrasound-guided transmural drainage of infected pancreatic fluid collections with placement of covered self-expanding metal stents: a case series. Endoscopy 2012; 44: 429–33. [PMID: 22382852]
- Nici AJ, Hussain SA, Kim SH, Mehta P. Unique usage of a partially covered metal stent for drainage of a pancreatic pseudocyst via endosonography-guided transcystgastrostomy. Dig Endosc 2012; 24:185–7. [PMID: 22507094]
- Thomasset SC, Berry DP, Garcea G, Ong SL, Hall T, Rees Y, et al. A simple, safe technique for the drainage of pancreatic pseudocysts. ANZ J Surg 2010; 80:609–14. [PMID: 22507094]
- Walter D, Will U, Sanchez-Yague A, Brenke D, Hampe J, Wollny H, López-Jamar JM, et al. A novel lumen-apposing metal stent for endoscopic ultrasound-guided drainage of pancreatic fluid collections: a prospective cohort study. Endoscopy 2015; 47:63–7. [PMID: 25268308]
- Shah RJ, Shah JN, Waxman I, Kowalski TE, Sanchez-Yague A, Nieto J, Brauer BC, et al. Safety and efficacy of endoscopic ultrasound-guided drainage of pancreatic fluid collections with lumen-apposing covered self-expanding metal stents. Clin Gastro enterol Hepatol 205; 13: 747–52. [PMID: 25290534]
- Varadarajulu S, Christein JD, Wilcox CM. Frequency of complications during EUS-guided drainage of pancreatic fluid collections in 148 consecutive patients. J Gastro enterol Hepatol 2011; 26:1504–8. [PMID: 21575060]
- Sadik R, Kalaitzakis E, Thune A, Hansen J, Jönson C. EUS-guided drainage is more successful in pancreatic pseudocysts compared with abscesses. World J. Gastro enterol 2011; 17:499–505. [PMID: 21274380]
- Itoi T, Itokawa F, Sofuni A, Umeda J, Tsuchiya T. Late bleeding after EUS-guided transjejunal drainage of a pancreatic pseudocyst in a Roux-en-Y patient. Dig Endosc2011; 1:51–3). [PMID: 21535202]
- Trevino JM, Christein JD, Varadarajulu S. EUS-guided transesophageal drainage of peripancreatic fluid collections. Gastro intest Endosc 2009; 70:793–7. [PMID: 19647247]
- Varadarajulu S, Bang JY, Sutton BS, Trevino JM, Christein JD, Wilcox CM. Equal efficacy of endoscopic and surgical cystogastrostomy for pancreatic pseudocyst drainage in a randomized trial. Gastroenterology 2013; 145: 583–90.e1. [PMID: 23732774]
- Panamonta N, Ngamruengphong S, Kijsirichareanchai K, Nugent K, Rakvit A. Endoscopic ultrasound-guided versus conventional transmural techniques have comparable treatment outcomes in draining pancreatic pseudocysts. Eur J Gastro enterol Hepatol 2012; 24:1355–62. [PMID: 23114741]
- Bakker OJ, van Santvoort HC, van Brunschot S, Geskus RB, Besselink MG, Bollen TL, et al. Endoscopic transgastricvs surgical necrosectomy for infected necrotizing pancreatitis: a randomized trial. JAMA 2012; 307:1053–61. [PMID: 22416101]
- Prachayakul V, Phisalprapa P, Aswakul P. Infected Walled-Off Pancreatic Necrosis following EUS-Guided Drainage Successfully Treated Using Multiple Stents in Different Sites Technique. Case Rep Gastro enterol 2013; 7:404–8. [PMID: 24163653]
- Baron TH, Thaggard WG, Morgan DE, Stanley RJ. Endoscopic therapy for organized pancreatic necrosis. Gastroenterology 111: 755–64. [PMID: 8780582]
- vanBrunschot S, van Santvoort HC, Gooszen HG, Fockens P. [Endoscopic versus surgical treatment of infected necrotising pancreatitis: the TENSION study]. Ned Tijdschr Geneeskd 2012; 156: A4329. [PMID: 22278038]
- Seifert H, Biermer M, Schmitt W, Jürgensen C, Will U, Gerlach R, Kreitmair C, et al. Transluminal endoscopic necrosectomy after acute pancreatitis: a multicentre study with long-term follow-up (the GEPARD Study) 2009; Gut 58:1260–6. [PMID: 19282306]
- Gardner TB, Chahal P, Papachristou GI, Vege SS, Petersen BT, Gostout CJ, et al. A comparison of direct endoscopic necrosectomy with transmural endoscopic drainage for the treatment of walled-off pancreatic necrosis. GastrointestEndosc2009; 69:1085–94. [PMID: 19243764]
- Rische S, Riecken B, Degenkolb J, Kayser T, Caca K. Transmural endoscopic necrosectomy of infected pancreatic necroses and drainage of infected pseudocysts: a tailored approach. Scand. J. Gastroenterol 2013; 48: 231–40. [PMID: 23268585]
- Gardner TB, Coelho-Prabhu N, Gordon SR, Gelrud A, Maple JT, Papachristou GI, et al. Direct endoscopic necrosectomy for the treatment of walled-off pancreatic necrosis: results from a multicenter U.S. series. GastrointestEndosc 2011; 73:718–26. [PMID: 21237454]






