Neil Bhardwaj, Sebastien Haiart, Harsh A Kanhere and Guy J Maddern
University of Adelaide Discipline of Surgery, The Queen Elizabeth Hospital. Woodville, SA, Australia
- *Corresponding Author:
- Neil Bhardwaj
Department of Surgery; The Queen Elizabeth Hospital;
Woodville road; Woodville, Adelaide, SA 5011; Australia
Phone: +61-(08).8222.6511
Fax: +61-(08).8222.6028
E-mail: neilbhardwaj@yahoo.co.uk
Received July 28th, 2013 – Accepted November 6th, 2013
Keywords
Carcinoma, Merkel Cell; Neoplasm Metastasis; Pancreas
INTRODUCTION
Merkel cell carcinomas is a rare skin tumour first described by Toker in 1972. The cells arise from the amine precursor uptake and decarboxylation cell system and, although originally thought to migrate from the neural crest, recent mammalian studies suggest they develop from epidermal cell lineage. They only represent a fraction of skin cell tumours with an incidence of 0.18-0.41/100,000 and UV light and fair skin are known risk factors [1]. Merkel cell carcinoma show a propensity for local spread and metastasis to regional lymph nodes and, although distant metastasis has been reported in multiple sites including intra-abdominal, thoracic, and the central nervous system [2, 3, 4], pancreatic metastasis is rare. We present a case of pancreatic metastasis of Merkel cell carcinoma and review the literature concentrating particularly on the pattern of presentation of this rare disease and the variety of surgical, adjuvant and neo-adjuvant treatments available.
CASE REPORT
A 62-year-old Caucasian woman from regional Australia presented to our hospital in 2013 for investigation of a pancreatic mass found on CT whilst being investigated by her general practitioner for epigastric pain, bloating and anorexia. The scan showed a large mid-body pancreatic mass with vascular involvement, thought to be most likely a primary pancreatic tumour, and she was referred to our unit for further treatment (Figure 1). Her tumour markers including CA 19.9 were normal and after discussion in the multidisciplinary meeting she underwent a trans-hepatic percutaneous biopsy for this unresectable mass. Pathological examination of this tissue showed CD56 and CK20 positivity and two independent pathologists reported it to be most likely of Merkel cell carcinoma origin.
Figure 1. Large mid-pancreatic body mass.
In 2004, she presented to her general practitioner with a lesion on the dorsum of her right hand. A punch biopsy was reported as being consistent with a squamous cell carcinoma in-situ and this was confirmed after complete excision. Several months later a 25x20 mm lesion at the same location was excised without pre-operative punch biopsy as it was thought to be either recurrent squamous cell carcinoma or an infection. This lesion showed small to medium round cells, a high nuclear-tocytoplasmic ratio with an area of vague trabeculae highly suggestive of Merkel cell carcinoma. This was confirmed on immunohistochemistry as it was positive for CD56, several keratin markers and CK20.
In light of this new diagnosis, further imaging was organised which revealed ipsilateral axillary lymphadenopathy. FNA was inconclusive so a lymph node biopsy was taken, which was consistent with lymph node metastasis of Merkel cell carcinoma, similar to the lesion on the right hand. A level 3 axillary clearance, including excision of the clinically involved thoracodorsal artery and nerve, was undertaken. All nodes were pathologically involved and the patient was referred for oncological treatment. She completed a course of radiotherapy; however, chemotherapy had to be ceased as she was admitted to ICU with severe sepsis. She survived that episode and lived independently till she was referred to our department almost 9 years later.
After the diagnosis of metastatic Merkel cell carcinoma she was discharged home and was due to be followed up by oncology with a view to discussing the possibilities of oncological treatment. However, she was admitted 6 weeks later to her local hospital with general deterioration. Given the poor prognosis, her decreased reserve from the prior round of chemotherapy associated sepsis and underlying Parkinson’s disease she opted to undergo no further treatment. She passed away soon after this admission.
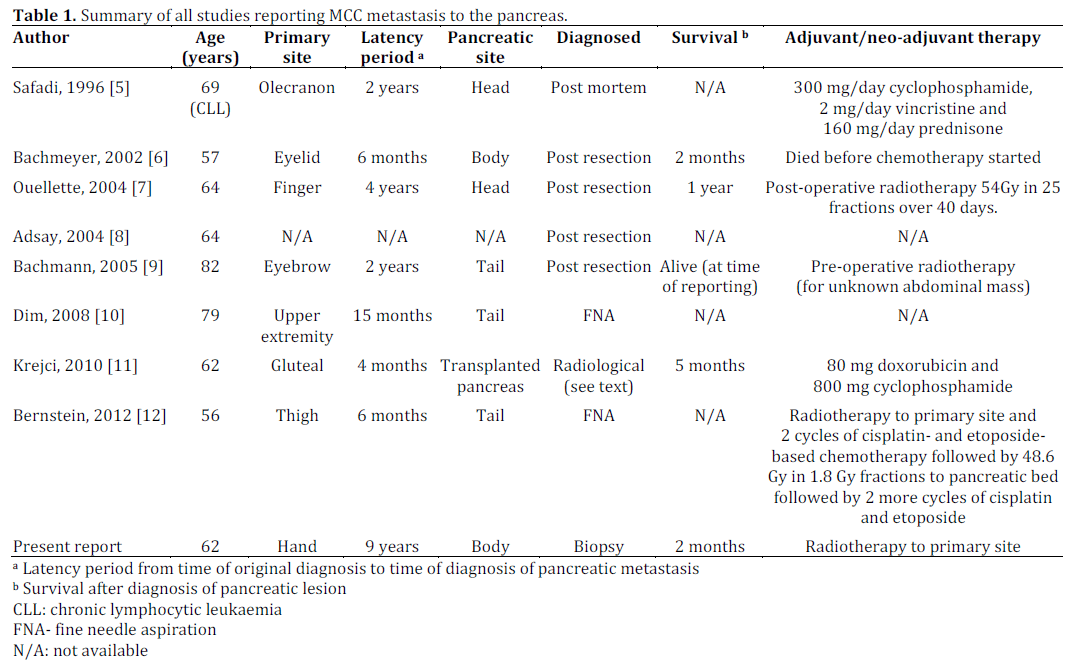
After an extensive literature search, only 8 cases of Merkel cell carcinoma metastasising to the pancreas were identified (Table 1), the present study has been added to the table to allow easy comparison. Each article was reviewed and relevant references in those papers requested and reviewed as well.
DISCUSSION
This is a rare case with only 8 cases previously described in the literature and the third of its kind diagnosed by FNA or biopsy [10, 12]. It is worth noting that immunosuppression increases the risk of developing Merkel cell carcinoma [12, 13] and in particular kidney transplant patients have a 15-fold higher incidence compared to the general population [13]. This may explain two cases described in the literature; one with previous history of chronic lymphocytic leukaemia [10] and another on immunosuppression drugs post kidney and pancreatic transplant who developed Merkel cell carcinoma metastasis in his transplanted pancreas. Regional lymph node biopsy, rather than direct biopsy of the pancreas, yielded the diagnosis in this case [11].
Although this rare case report shares some similarities from the described cases in the literature, there are some unique features such as this being only one of two cases found in the body of the pancreas and one with the longest latency period; however, in keeping with three of the cases, survival was in months once the diagnosis was made. In contrast to primary Merkel cell carcinoma, there are no guidelines as to the treatment of pancreatic metastasis, which would account for the myriad of approaches undertaken in the above studies. It is noticeable that 50% were diagnosed post-resection but it is difficult to recommend this approach as the gold standard as survival and treatment data regarding those not resected were not reported. However, it would seem like a reasonable approach if the patient was fit enough and a R0 resection was possible. Nevertheless, this case report does prove that metastasis can be diagnosed by a biopsy and, as reported in several other cases, can be diagnosed by CK20 (epithelial) and CD56 (neuroendocrine) expression alone.
CONCLUSION
We report a rare case of a Merkel cell carcinoma metastasis to the pancreas and the rapidity of the patient’s deterioration justified our conservative management. It is important to exclude this rare cause of a mass in the pancreas in patients with a previous history of Merkel cell carcinoma, even if there is a long period between the primary tumour and the pancreatic mass. Whether this is done after resecting the mass, which is a reasonable approach if a R0 resections seems possible, or by biopsy/FNA remains to be determined. We believe the factors that should be taken into consideration include resectability of the lesion, disease spread and general fitness of the patient.
Conflict of interest
There was no external funding or conflict of interest in preparing this case report
References
- Schrama, D., S. Ugurel, and J.C. Becker, Merkel cell carcinoma: recent insights and new treatment options. Curr Opin Oncol, 2012. 24(2): p. 141-9.
- Abul-Kasim, K., K. Soderstrom, and L. Hallsten, Extensive central nervous system involvement in Merkel cell carcinoma: a case report and review of the literature. J Med Case Rep, 2011. 5: p. 35.
- Payne, M.M., et al., Merkel cell carcinoma in a malignant pleural effusion: case report. Cytojournal, 2004. 1(1): p. 5.
- Wolov, K., O. Tully, and G. Mercogliano, Gastric metastasis of Merkel cell carcinoma. Clin Gastroenterol Hepatol, 2009. 7(3): p. A26.
- Safadi, R., et al., Merkel cell tumor in a woman with chronic lymphocytic leukemia. Leuk Lymphoma, 1996. 20(5-6): p. 509- 11.
- Bachmeyer, C., et al., Cystic metastasis of the pancreas indicating relapse of Merkel cell carcinoma. Pancreas, 2002. 24(1): p. 103-5.
- Ouellette, J.R., et al., Merkel cell carcinoma metastatic to the head of the pancreas. JOP, 2004. 5(2): p. 92-6.
- Adsay, N.V., et al., Secondary tumors of the pancreas: an analysis of a surgical and autopsy database and review of the literature. Virchows Arch, 2004. 444(6): p. 527-35.
- Bachmann, J., et al., Pancreatic metastasis of Merkel cell carcinoma and concomitant insulinoma: case report and literature review. World J Surg Oncol, 2005. 3: p. 58.
- Dim, D.C., et al., Metastatic merkel cell carcinoma of the pancreas mimicking primary pancreatic endocrine tumor diagnosed by endoscopic ultrasound-guided fine needle aspiration cytology: a case report. Acta Cytol, 2009. 53(2): p. 223- 8.
- Krejci, K., et al., Merkel cell carcinoma of the gluteal region with ipsilateral metastasis into the pancreatic graft of a patient after combined kidney-pancreas transplantation. Onkologie, 2010. 33(10): p. 520-4.
- Bernstein, J., et al., Endoscopic ultrasound-guided fine-needle aspiration diagnosis of merkel cell carcinoma metastatic to the pancreas. Diagn Cytopathol, 2012.
- Becker, J.C., D. Schrama, and R. Houben, Merkel cell carcinoma. Cell Mol Life Sci, 2009. 66(1): p. 1-8.


