We are living in
a complex, changing world, and within health care, primary care is undergoing
per-haps the greatest degree of change. Not so long ago, primary care was
largely defined by the services provided by general medical practitioners, who
were broadly trained to provide a wide range of services. The primary focus was
on the care of individual patients, who would access the healthcare system via
an initial consultation and have most of their prob-lems sorted out
individually. Only a small proportion would need to be referred to more
specialised services, generally hospital-based services, for more expensive,
extensive or specific investigations. Other health pro-fessionals played
support roles that freed up the time of general practitioners (GPs), who could
focus on patients with more serious conditions. The service was more reactive
than proactive, as diagnosis, investigation and management would commence once
patients presented with their symptoms.
The continuing and rapid trend in primary care is in the direction of
providing teams of highly trained, more specialised services that keep patients
within the community for longer, defer or delay admission to hospitals, and
accelerate discharge back to the com-munity. A more proactive approach to maintaining
health and preventing illness sees patients being investigated increasingly
within general practices, and increasingly managed by practice nurses with
expanded roles.[1] Pharmacists and nurses may prescribe a range of
medications without reference to medical practitioners, although following
medically supported protocols.[2] Many GPs have moved along the
medical spectrum to offer services once provided by general physicians,
and many subspecialise in ‘special interests’ to become GPs with special
interests (GPwSIs).[3] Referral to hospital-based specialists is more
likely to be directed to a narrower subspecialty, with patients either
par-tially or completely investigated. Investigations and procedures can more
easily be instigated, and their results managed, within primary care. A
substantial proportion of inpatient activity, within the range of 60–80%, is
now taking place in ‘same-day’ centres,often attached
to facilities for overnight accommo-dation of those patients too ill to go
home.
These changes have clear implications for the measurement of the
quality of care. Quality is a construct that should include the perspectives of
all stakeholders – patients, commissioners, professional regulators and
individual health professional groups.[4,5] These perspectives
differ: patients are known to be more concerned with accessibility
issues, commissioners with costs and cost efficiency, professional
regulators with standards of care, and individual professional groups with
training standards.[6,7] Whereas once the perspective of the
individual practitioner was an im-portant part of the complexity, a focus on
outcomes of primary health care replaces individual performance perspectives
with that of the whole primary care team, and individual knowledge and skills
with those of the team role played by individual practitioners. Increas-ingly,
primary care teams need not just any practi-tioner to fill specific roles, but specific
practitioners with specific knowledge and skills that make the team function
better. Individuals will need to be trained to meet specific roles, and these
roles will change as healthcare provision models change. In some cases the role
changes may be evolutionary, building on prior knowledge and skills, whereas in
others the changes may be revolutionary, as certain roles become un-necessary
and new roles emerge. Therefore all team members may require periodic
retraining for a new role, as well as the usual continuing professional
development that maintains currency of existing and evolving professional
roles.
This view may be a challenge to the traditional view of clinical
practice as the results of the endeavours of only one or two individuals within
the group. How-ever such development should not be seen as a threat, so long as
the focus is maintained on what primary care is supposed to deliver. This also
requires a shift from consideration of structures and processes of primary care
practice, towards the outcomes of pri-mary care service delivery,[8]
adopting a more systems-based approach to health care.[9] Most of the
clinical indicators in
the Quality and Outcomes Framework used in the UK reflect baseline structure
and process measures,[10] although many can be achieved only through
effective teamwork. It is not yet clear how well such intermediate
measures predict longer-term health outcomes, and each clinical condition may
have a unique set of predictive factors for outcomes, for example low back
pain.[11]
The future of health care requires health profes-sionals to be
effective team members. Effective teams are not created easily or
quickly, but instead require effective guidance, leadership,
collaborative working and joint ownership of outcomes. The ability to work in
teams may be something that health professional students can learn,[12]
although true teamwork can probably be developed only within genuine teams.[13]
The importance of stability of personnel to team function is not fully
understood, but teams in primary care are likely to be more stable than those
that will emerge in hospitals, where restrictions on working hours already
require new models of teamwork to provide effective continuity of care
over 24 hours a day, 7 days a week. In primary care almost all clinical care is
provided within relatively normal working hours, minimising the necessity for complex
handover and continuity procedures, although regional after-hours co-operative
services will have to transmit information to and from their network of primary
care practices. Most team members will work together most of the time.
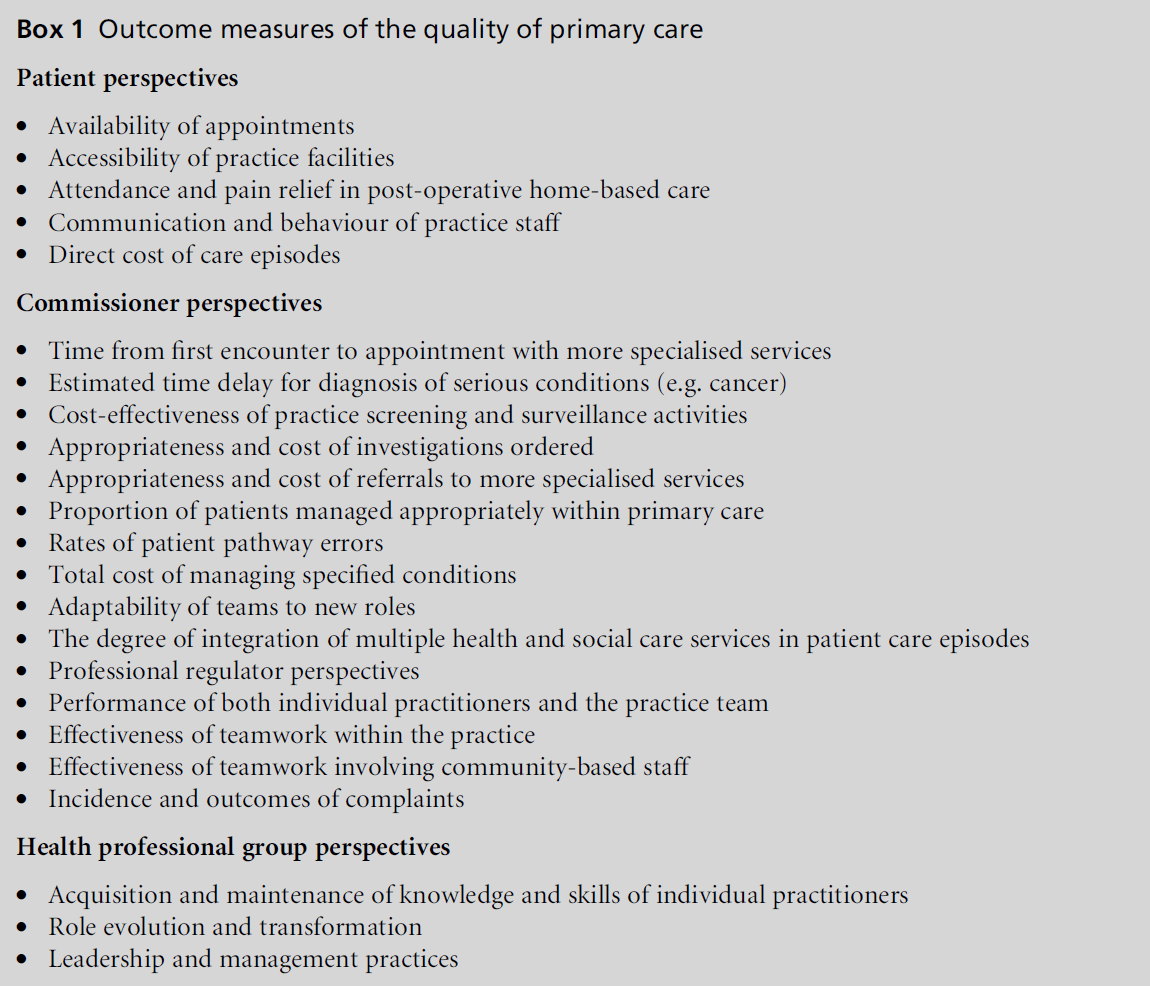
While discussions about improving quality will generally attract
universal support, improvement may not happen unless it is looked for. A list
of potential outcome measures for the quality of primary care that address
these changes, grouped by stakeholder per-spective, is provided in Box 1. Some
are not new, and the list is by no means exhaustive, but it demonstrates a
shift to measures of outcomes of at least individual healthcare episodes,
rather than processes, and to team rather than individual effort. Just as
teamwork is increasingly the process by which health care is provided, outcome
measurement methods will have to focus on team performance, although ideally
they will be sensitive to the roles and functions of individ-ual team members.
This shift in measurement may require method-ological development. The
best way to measure team performance is to focus on achievement of team goals, rather than
individual performance, but this is coun-ter to the thus-far different
cultures and hierarchical nature of the healthcare professions. The culture
will need to change and adopt the continuing quality improvement principles of no
fault reporting, which may require careful attention to whistleblowing and
data-protection procedures. However, the price of not changing may be high.
References
- Leese B. New opportunities for nurses and other
healthcare professionals? A review of the potential impact
of the new GMS contract on the primary care
workforce. Journal of Health Organization and Management
2006;20:525–36.
- Department of Health. Nurse and pharmacist prescribing
powers extended. www.dh.gov.uk/en/Publications
andstatistics/Pressreleases/DH_4122999 (accessed 5 April
2007).
- Nocon A and Leese B. The role of UK general practitioners
with special clinical interests: implications for
policy and service delivery. British Journal of General
Practice 2004;54:50–6.
- Donabedian A. The seven pillars of quality. Archives of
Pathology and Laboratory Medicine 1990;114:1115–18.
- Institute of Medicine. Measuring the Quality of Health
Care. In: Donaldson MS (ed). The National Roundtable
on Health Care Quality. Washington: Institute of Medicine,
1999.
- Jenkinson C, Coulter A, Bruster S, Richards N and
Chandola T. Patients’ experiences and satisfaction with health care: results of a questionnaire study of specific
aspects of care. Quality and Safety in Health Care
2002;11:335–9.
- Price M, Fitzgerald L and Kinsman L. Quality improvement:
the divergent views of managers and clinicians.
Journal of Nursing Management 2007;15:43–50.
- Donabedian A. The quality of care. How can it be
assessed? Journal of the American Medical Association
1988;260:1743–8.
- Enthoven AC and Vorhaus CB. A vision of quality in
health care delivery. Health Affairs (Project Hope) 1997;
16:44–57.
- Department of Health. Quality and Outcomes Framework
2004. London: Department of Health. www.dh.gov.
uk/en/Policyandguidance/Organisationpolicy/Primary
care/Primarycarecontracting/QOF/DH_4125653.
- Enthoven P, Skargren E, Carsetnsen J and Oberg B.
Predictive factors for 1 and 5 year outcome for disability
in a working population of patients with low back pain
treated in primary care. Pain 2006;122:137–44.
- Kyrkjebo JM, Brattebo Gand Smith-Strom H. Improving
patient safety by using interprofessional simulation
training in health professional education. Journal of
Interprofessional Care 2006;20:507–16.
- West M. Effective Teamwork. Oxford: Blackwell, 2004,
pp. 27–48.

