Willemijn LA Scha¨ fer*
Wienke GW Boerma
NIVEL, Netherlands Institute for Health Services Research, Utrecht, The Netherlands
Dionne S Kringos
NIVEL, Netherlands Institute for Health Services Research, Utrecht, The Netherlands and Department of
Social Medicine, Academic Medical Centre (AMC), University of Amsterdam, The Netherlands
Evelyne De Ryck
Department of General Practice and Primary Health Care, Ghent University, Belgium
Stefan Greß and Stephanie Heinemann
Hochschule Fulda – University of Applied Sciences, Fulda, Germany
Anna Maria Murante
Laboratorio MeS, Istituto di Management, Scuola Superiore Sant’Anna, Italy
Danica Rotar-Pavlic
ULMF – University of Ljubljana, Slovenia
Franc¸ ois G Schellevis
NIVEL, Netherlands Institute for Health Services Research, Utrecht, The Netherlands and Department of
General Practice and Elderly Care Medicine, EMGO Institute for Health and Care Research, VU University
Medical Center, Amsterdam, The Netherlands
Chiara Seghieri
Laboratorio MeS, Istituto di Management, Scuola Superiore Sant’Anna, Italy
Michael J Van den Berg
RIVM – National Institute for Public Health and the Environment, Bilthoven, The Netherlands and Tranzo,
Tilburg University, The Netherlands
Gert P Westert
Radboud University Nijmegen Medical Centre, The Netherlands
Sara Willems
Department of General Practice and Primary Health Care, Ghent University, Belgium
Peter P Groenewegen
NIVEL, Netherlands Institute for Health Services Research, Utrecht, The Netherlands and Department of
Sociology and Department of Human Geography, Utrecht University, The Netherlands
- *Corresponding Author:
- Willemijn LA Scha¨fer
NIVEL, Netherlands Institute
for Health Services Research
Utrecht, The Netherlands
Email: w.schafer@nivel.nl
Received date: 24 October 2012; Accepted date: 25 January 2013
Keywords
health care surveys, health services research,
outcome assessment (health care), primary
health care
Background
Many European countries share the goal of initiating
or sustaining strong primary health care systems. As a
result, there is a demand for benchmarking information
and a growing tendency to learn from foreign experiences. Evidence on the outcomes of primary
health care in European countries is, however, still
incomplete.[1] Variation in the organisation of primary
health care in Europe enables analyses of the relationship
between primary care organisation and outcomes.
Decision makers may benefit from information about arrangements of primary health care which are more
likely to produce better outcomes.[2]
In 2010, the three-year Quality and Costs of Primary
Care in Europe (QUALICOPC) study started.
This study aims to compare and analyse how the
primary health care systems of 35 countries perform
in terms of quality, costs and equity. The results of this
study will contribute to evidence on the benefits of
strong primary health care and on the performance of
health care systems in general. The European countries
include 27EUcountries, Iceland,Norway,Turkey,
Switzerland and Macedonia. Outside Europe, Australia,
Canada and New Zealand have joined the study. For
this study, data will be gathered by means of surveys
among general practitioners (GPs) and their patients.[1]
National characteristics of the organisation of primary
health care will be derived from other sources, such as
the Primary Health Care Activity Monitor (PHAMEU)
database.[3] GPs were chosen as survey subjects, because
they can be seen as the main providers of primary
health care. However, the project aims to provide
insight into not only GP care, but also primary health
care as a whole. Fieldworkers, who will visit GP practices to recruit patients and assist them, if necessary,
with filling in the questionnaire, will also fill in a
practice questionnaire. The data from GPs, patients
and fieldworkerswill be linked to each other. For more
information on the QUALICOPC study, see Box 1.[1]
Primary health care can be characterised as the first
level of access to care and is provided near patients’
homes. Primary health care includes curative and
rehabilitative care, preventive care and health education.
[4,5] A recent literature review on primary health
care6 distinguishes three levels of care, namely the
structure, process and outcome of care. Within these
levels, 10 core dimensions to measure primary health
care were identified (see Table 1).
The QUALICOPC study aims to comprehensively
evaluate the breadth of primary health care by gathering
data on all these dimensions.
The analyses will focus on the following overarching
themes: quality of the process of care (including the
dimensions of access, continuity, coordination and
comprehensiveness of primary health care services),
experiences of patients (as an indicator of the dimension
quality of primary health care), costs of primary health care (as a part of the dimension efficiency of
care), equity (related to the dimension access and the
quality of primary health care), avoidable hospitalisation
(as an indicator of the dimension quality of
primary health care). A sixth synthesising theme will
be the identification of ‘good practices’ of primary
health care provision (related to all dimensions to
measure primary health care).[1]


To collect data related to these six themes, new
questionnaires had to be developed. Many previous
studies have used questionnaires for primary health
care physicians and patients. In the past, comprehensive
primary care studies have been performed, for
example by Barbara Starfield[7] and the Commonwealth
Fund,[8] but only a limited number of European countries
were included. Furthermore, many studies that
have used questionnaires from GPs and patients had a
focus on specific subjects or themes rather than a
multidimensional approach. This study aims to unravel
the processes and contributions of primary
health care to its outcomes in terms of quality, costs
and equity. The questions in the questionnaire should
not only cover all themes but also be suitable for use in
international surveys, which means that differences in
the health care context between countries need to be
taken into account.
This article describes the background to and development
of the questionnaires for the QUALICOPC
study. It addresses the question ‘How can the quality,
costs and equity of a primary health care system be
measured?’ Furthermore, criteria used for inclusion or
exclusion of questions are presented, as well as an
overview of the resulting questions that can be used for
international comparative research on primary health
care.
Methods
Four questionnaires were developed: one for GPs, one
for patients about their experiences with their GP,
another for patients about their values regarding
primary care (i.e. what they consider important), and
finally one about the practice. Because the project aims to
provide insight into GP care as a whole, the GP questionnaire
should also include questions beyond the
scope of the tasks of the GP. The questionnaire about
what patients find important is added to weigh against
their experiences. Development of the questionnaires
consisted of four phases: a search for existing questionnaires,
the classification and selection of relevant questions
(including formulation of inclusion and exclusion
criteria), shortening of the questionnaires and the pilot
survey. An overview of the development process is
presented in Figure 1.
Phase 1: bibliometric search
In the first phase, existing questionnaires, published
between 1990 and 2010 and with an abstract written in
English, were searched for in the bibliographic
databases PubMed and Embase. The search aimed to
identify validated questionnaires for primary health
care physicians and patients, suitable for international
comparisons. Search terms were derived from the 10
dimensions formeasuring primary health care (Table 1).
In addition, attention was paid to identifying questionnaires
on avoidable hospitalisation, which is not
explicitly covered in the dimensions, and on equity,
which has received relatively little attention in international
comparative primary health care research.[2,6]
Phase 2: classification, selection,
rephrasing and new questions
In the second phase, questions from the included
questionnaires were classified according to the 10
dimensions. Next, the researchers selected questions
that contribute to answering the main research questions
of the QUALICOPC study. Questions were
rephrased to fit the study approach and aim. Furthermore,
new questions were formulated for gaps that
were identified. The identified questions were divided
between the provisional list of questions for the GP
questionnaire and the Patient Experiences and Patient
Values questionnaires.
Phase 3: consensus rounds
Next, in three consensus rounds, the researchers
evaluated the questionnaires and selected the questions
for inclusion. Each of the questions was discussed
for its relevance to the purpose of this study and
the exclusion criteria in order to further increase the
suitability of the questions for the surveys. The researchers
developed the following set of criteria for
inclusion/exclusion:
• the question is not suitable for international comparison
(e.g. not applicable in several countries)
• the question refers to a characteristic of the health
care system (that can be found elsewhere, e.g. the
PHAMEU database) rather than to a characteristic
of an individual practice or experience of a patient
• very little variation in the answers is expected, both
within and between countries
• the question is very detailed and will provide only
fractional information
• answers to the questions are expected to be unreliable
(e.g. due to social desirability bias)
• the question is likely to be too difficult for the
respondent (e.g. it demands a high level of literacy).
In three rounds, the researchers submitted the
questions to these criteria, until consensus was found.
At this stage, questions were reformulated where
necessary to increase comprehensibility.
Pilot survey
As a final step, a pilot survey was held with GPs and
patients in Belgium, the Netherlands and Slovenia,
aiming to test the practicality and applicability of the
survey and the comprehensibility and appropriateness
of the questions. In each country, a convenience
sample of GPs (around 10) was invited to participate.
GPs were asked to fill in the questionnaire, which
contained an extra column to add comments and
questions to the questionnaire. Furthermore, project
researchers visited the general practices to recruit a
random sample of patients. In each practice, four
consecutive patients who agreed to fill in the questionnaire
were included. This resulted in a total of 112
completed questionnaires from patients (40 in Belgium
and Slovenia and 32 in the Netherlands). During the visits, researchers filled in a checklist, took notes of the
proceedings and asked the patients to directly mention
problems or questions which they did not understand.
Based on the findings of the pilot a final consensus
round was held in which the questionnaires were
further shortened and questions which were found
too difficult were rephrased.
During the pilot and the subsequent final consensus
round, special attention was paid to the intelligibility
of questions, because the changed wording of several
questions could have affected their validity. Explicit
cognitive testing, however, has not been part of the
pilot study. For two reasons it was decided not to
assess the psychometric properties of the draft questionnaires.
First, questions dealing with factual circumstances
or facilities are less suitable for such testing.
Besides, questions copied from validated questionnaires
have been tested already. For instance, the
questions on services that GPs offer to their patients
that are derived from the European GP Task Profile
study have been tested for internal consistency and
scale reliability.[9]
Results
In this section, the results of each of the phases of the
development are discussed. Next, the final outcomes,
namely the questionnaires, are presented.
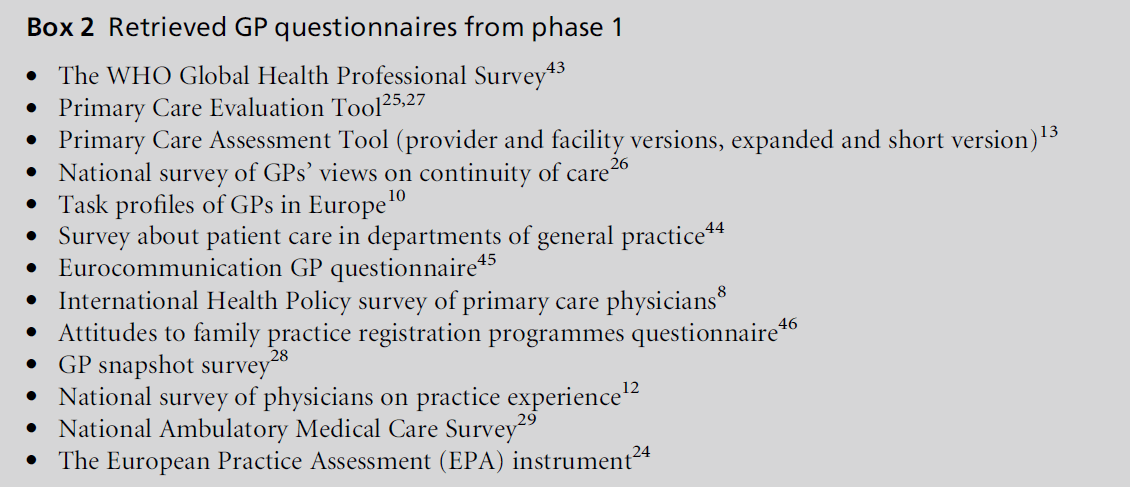
Phase 1: bibliometric search
Through the bibliometric search, 2783 potentially
relevant studies for the GP questionnaire were identified.
After careful screening, 13 relevant primary
health care physician questionnaires were identified,
an overview of which is presented in Box 2. For the
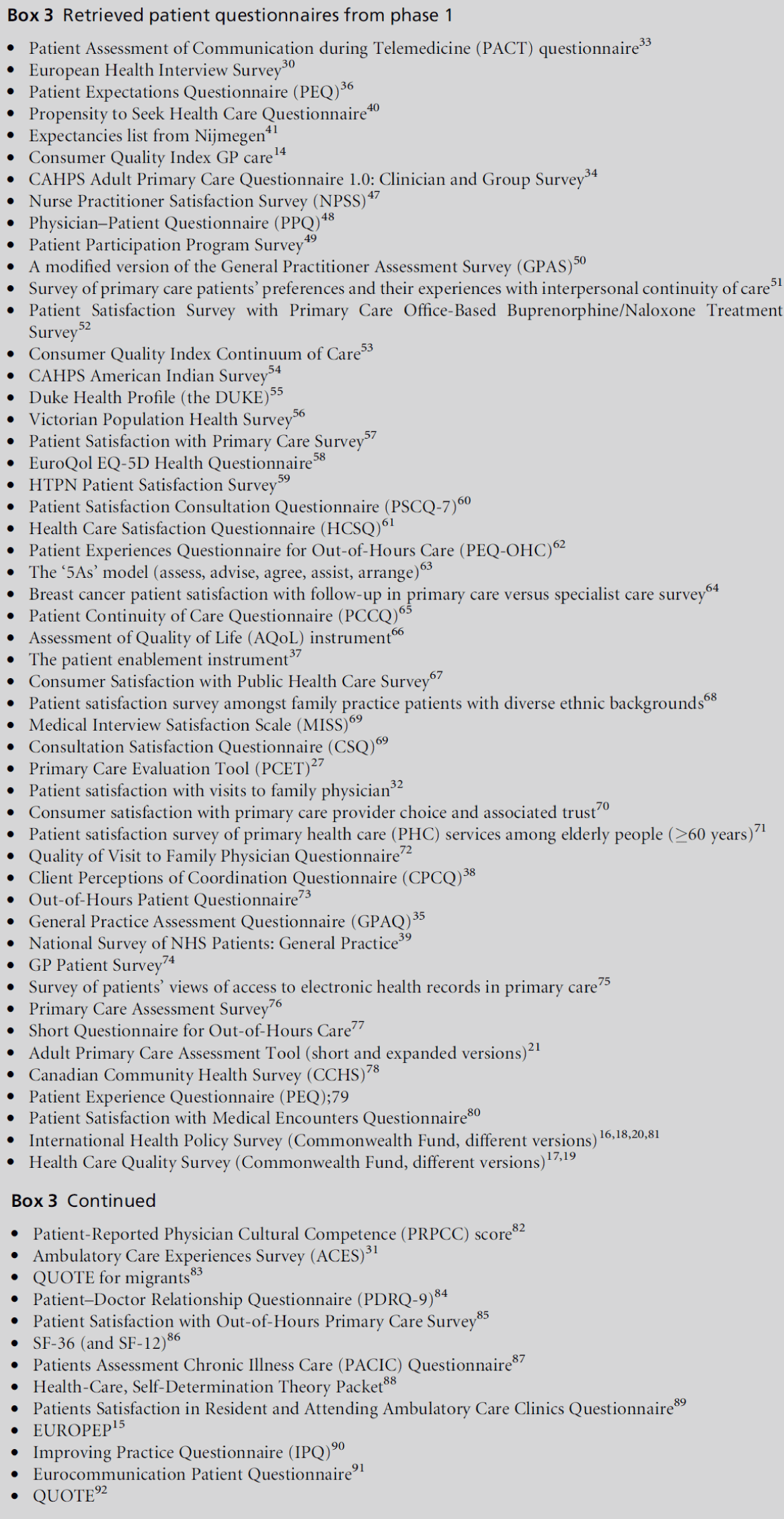
patient questionnaire, 2213 potentially relevant sources
were found, which eventually resulted in 64 relevant
questionnaires (see Box 3).
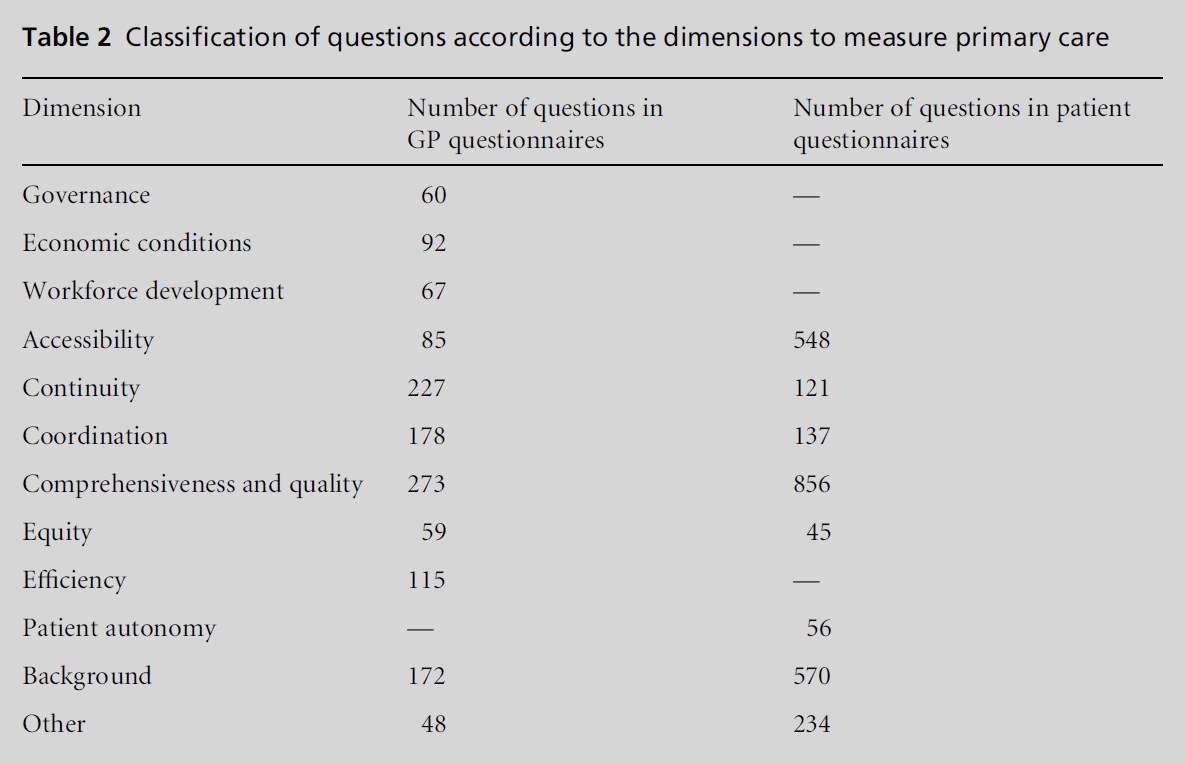
Phase 2: classification, selection,
rephrasing and new questions
All questions from the retrieved questionnaires were
classified according to the dimensions to measure
primary care. The result of this classification is
presented in Table 2. As some questions were classified
in more than one dimension, the total number in the
figure is higher than the number of questions that
emerged from the search.
For each of the dimensions, the researchers selected
questions potentially relevant to this study. An
example of a question which was not included in the
first selection phase is about the health plans of the
patients. This question is country specific and not
suitable for comparison between countries. After this
first phase, 138 questions for GPs and 117 for patients
remained.
Phase 3: consensus rounds
During the consensus phase, the questions on the
provisional were further narrowed (based on the
exclusion criteria) and rephrased, where necessary.
For instance, as more and more GPs work part-time,
the question about the number of GP colleagues
working in the same practice was further specified to
include the number of full-time equivalents (FTEs) in
addition to the absolute number. The number of
remaining questions after each round is indicated in Figure 1.

Figure 1 Phases in the development of the questionnaires.
Pilot
The pilots showed that the questionnaires were
reasonably well understood and easily administered,
suggesting acceptable clarity and applicability. However,
both the GP and Patient Experiences questionnaires
were too long, as the average time needed for
completion exceeded the set limits of 30 minutes for
GPs and 20 minutes for patients. Furthermore, in the
GP questionnaire mistakes were identified (e.g. names
of equipment were incorrect). Some questions in the
patients’ questionnaire appeared too difficult.
The pilot resulted in a further reduction of the
questionnaire, reformulation of several questions
and the development of a short practice questionnaire
about general characteristics of the practice (e.g.
cleanliness of the waiting room).
GP questionnaire
The final GP questionnaire (see Appendix A – available
online) contains 60 questions (25 of which have
two or more subquestions). The majority of the
questions have prestructured multiple choice answers.
In 13 questions, GPs are also asked to fill in numerical
answers (e.g. a percentage or a number of hours).
Appendix A (available online) also provides an
overview of the thematic content of each of the
questions and the sources used for the questions.
Three questions focus on the background of the GP
and four on the characteristics of the practice (e.g. the
composition of the practice population). ‘Efficiency is
measured by seven questions for instance on time
allocation of the GP. Within the theme ‘‘workforce
development’’ there are four questions, from additional
professional activities of GP and disciplines
working in the practice to job satisfaction. Five questions
focus on ‘economic conditions’ (payment of the
GP and co-payment for patients). ‘Equity in access’ is
reflected in questions about restrictions in access and
availability of care for uninsured patients.
To gain insight into the relationship between GPs
and the broader contacts of primary care, there are 12
questions about ‘coordination and cooperation’ between
GPs and other disciplines. Eleven questions
about the ‘continuity of care’ provided by the GPs
concentrate on disease management and on referrals
and information exchange. Special attention is paid to
medical record keeping.
‘Quality of care’ is measured with three questions
regarding the use of guidelines and feedback from
colleagues or authorities. ‘Comprehensiveness of care
services’ is reflected in 12 questions, dealing with the
available equipment and the GPs’ task profiles (e.g. the
range of problems for which the GP is the first point of
contact). Finally, nine questions covering ‘accessibility of care’ can be divided into those about physical access
(distance to the practice and opening hours) and those
about financial access to care services.
The European study on GP Task Profiles, carried
out in 30 European countries in 1992–93, is a major
source for the GP questionnaire.[10] Several questions
were copied from this questionnaire. Other important
sources are, for example, international surveys by the
Commonwealth Fund[8,11,12] (questions about financial
incentives, guideline use and medical record keeping)
and Starfield’s Primary Care Assessment Tool (question
about care for uninsured persons).[13]
For several topics, no examples of existing questions
were found and new questions had to be formulated.
These topics were involvement of GPs in disease management
programmes, equity in access and patient
involvement in the decision-making process.
Patient Experiences questionnaire
The Patient Experiences questionnaire, dealing with
the experiences of patients with their GP (see Appendix
B – available online), contains 41 multiple choice
questions (10 of which have two or more subquestions).
Many questions ask to what extent the
patient agrees with a statement. The questionnaire is
meant to be completed in the GP’s waiting room by
patients after consultation with their GP.
The 18 questions which concentrate on the patient’s
background concern the patient’s socio-economic
status, perceived health, reason for visiting the GP,
and visits to medical specialists and hospitals. Six
questions deal with measuring experiences with ‘continuity
of care’, e.g. the use of medical records. ‘Quality
of care’ as experienced by patients is measured in 13
questions (e.g. about the satisfaction of care needs in
connection to the patient’s relationship with the GP,
aspects of communication, safety, complaint handling
and preventive activities).
As in the GP questionnaire, the 14 questions about
the ‘accessibility of care’ can be divided into physical
and financial access. These questions also include the
time the GP has available for the patient, the availability
of home visits and waiting times. Three questions
pay attention to ‘equity in access’ and one
question to ‘equity in treatment’. ‘Coordination’ is
measured with five questions on experiences of coordination
in the case of referral and on treatment by a
practice nurse.
To mirror the questions in the GP questionnaire
about autonomy, patients are asked about their involvement
in decision making and referrals. ‘Comprehensiveness
of services’ is mirrored in a question
about patients’ views on the breadth of the clinical task
profile of services offered by the GP. Finally, two
questions specifically related to avoidable hospitalisation
were included.
Major sources for this questionnaire were the Consumer
Quality Index for GPs,14 the EUROPEP,[15]
several international Commonwealth Fund questionnaires
[16–20] and Starfield’s Adult Primary Care Assessment
Tool.[21] Compared with the GP questionnaires,
more questions for patients were identified in the
domain of equity in access and treatment. As few
questions were found on patient autonomy, new
questions had to be developed on this theme.
Patient Values questionnaire
Next, a Patient Values questionnaire was developed.
Measuring what patients consider important enables
the weighting of their experiences.[22] The Patient Values
questionnaire contains [19] questions (seven of which
have three or more subquestions). Again, most questions
are statements with multiple choice answers. A
few questions ask the patient to choose from a list what
they consider most important and fill in a number.
The 12 questions asking about the patient’s background
are similar to those in the Patient Experiences
questionnaire. Three questions contain statements
asking patients about the importance of certain aspects
of care (e.g. ‘How important is it that the practice
has extensive opening hours?’).
Finally, four questions focus on communication
between GPs and patients. The statements in these
questions were developed by the GULiVer partnership
based on their research on ‘tips’ from lay people on
how medical consultations could become more successful
from their perspective.[23]
Practice questionnaire
A 12-question practice questionnaire was developed
to record the response rate among patients during the
implementation of the survey and to measure practice-
related indicators with regard to the communication
of opening hours, and equity in access (e.g. for
handicapped persons). Most questions were based on
the European Practice Assessment indicators.[24]
Discussion
The four questionnaires have been developed to
characterise the organisation and delivery of primary
health care and to compare and analyse its outcomes.
The development of questionnaires for a multicountry
study on broad themes such as quality, costs and equity
in primary care requires a balance between methodological
requirements and practical feasibility. Indeed,
all dimensions deserved to be thoroughly investigated,
although theymay be difficult tomeasure reliably, but it must be accepted that only a limited set of questions
can be asked.
Nonetheless, the QUALICOPC consortium has
been able to produce the four questionnaires—as far
as possible—based on existing, validated questionnaires
and tested through a pilot survey in three
countries. A limitation of the pilot survey is that it
was carried out in only three countries. However,
much attention has been paid to having valid translations
in each language. In each country, an official
back-and-forth translation procedure is used for the
questionnaires, in which translators are asked to take
comprehensibility into account. Another limitation of
the questionnaire development is that questions, derived
from various validated sources, often had to be
‘processed’ to make them suitable for the QUALICOPC
study. This may have resulted in a loss of validity and
needs to be taken into account in the analysis phase.
The questionnaires for GPs and patients contain
questions that go beyond general practice. Furthermore,
data about primary health care (e.g. about its
costs) will be gathered at the national level in available
databases. Nevertheless, results regarding quality of
primary health care as a whole need to be interpreted
with care.
The dimension ‘Governance’ has not been covered
in any of the questionnaires, because aspects of governance
are relatively distant from daily reality in
primary health care. However, information on governance
will be used and derived from the PHAMEU
database. Relatively new topics that will be explored
in the QUALICOPC study are equity in access and
treatment, patient autonomy, disease management,
avoidable hospitalisation and patient experiences with
primary health care in general. There are also aspects
of care which might be interesting, but are not included
in these questionnaires. This included new
developments around telemedicine, but also the experiences
of patients around disease management programmes.
Equity in health can also not be measured
through this survey, as we only include patients who
visit GP practices and, moreover, we do not measure
health outcomes. Several questions had to be omitted
to keep the length of the questionnaire reasonable.
Because the sources were identified from Western
countries, the questionnaires that we developed are
more likely to be suitable for use in Western countries
than in others. However, the 35 countries in which the
questionnaires will be used in the context of the
QUALICOPC study match this profile well. The
results of the study will add to the available evidence
on the relationship between the strength of primary
care systems and their outcomes. The data from the
35 countries will be linked to the practices and their
patients. Analyses of the data will provide insight into
variations between countries at the level of the patient,
GP practice and country. The patient questionnaires may also be suitable for use at the practice level by GPs
to analyse developments in the GP practice by inviting
a sample of patients every year to complete a questionnaire.
References
- Scha¨fer WLA, Boerma WGW, Kringos DS et al.
QUALICOPC, a multi-country study evaluating quality,
costs and equity in primary care. BMC Family Practice
2011;12:115.
- Scha¨fer W, Groenewegen PP, Hansen J, Black N. Priorities
for health services research in primary care.
Quality in Primary Care 2011;19:77–83.
- Kringos DS, Boerma WG, Bourgueil Y et al. The European
primary care monitor: structure, process and
outcome indicators. BMC Family Practice 2010;11:81.
- Boerma WGW, Dubois CA. Mapping primary care
accross Europe. In: Saltman RB, Rico A, Boerma
WGW (eds). Primary Care in the Driver’s Seat? Organizational
reform in European primary care. Open University
Press: Buckingham, 2006; 22–49.
- Health Council of the Netherlands. European Primary
Care Report. Health Council of the Netherlands: The
Hague, 2004.
- Kringos DS, Boerma WG, Hutchinson A, van der Zee J,
Groenewegen PP. The breadth of primary care: a systematic
literature review of its core dimensions. BMC
Health Services Research 2010;10:65.
- Starfield B, Shi L, Macinko J. Contribution of primary
care to health systems and health. Milbank Quarterly
2005;83:457–502.
- The Commonwealth Fund. International Health Policy
Survey of Primary Care Physicians in Eleven Countries.
The Commonwealth Fund: New York, 2009.
- BoermaW.Task Profiles of General Practitioners in Europe.
NIVEL: Utrecht, 2003.
- Boerma W. Profiles of General Practice in Europe: An
international study of variation in the tasks of general
practitioners. NIVEL: Utrecht, 2003.
- Schoen C, Osborn R, Huynh PT, Doty M, Peugh J,
Zapert K. On the front lines of care: primary care
doctors’ office systems, experiences, and views in seven
countries. Health Affairs (Millwood) 2006;25(6):w555–
71.
- Commonwealth Fund. National Survey of Physicians on
Practice Experience. Commonwealth Fund: New York,
2003.
- Starfield B. Primary Care Assessment Tool – Expanded
Version (Provider survey). 1998.
- Meuwissen LE, de Bakker LH. ‘Consumer Quality-index
huisartsenzorg’ meet patie¨ntenervaringen en vergelijkt
huisartsenpraktijken [Consumer Quality Index GP care’
measures patient experiences and compares GP practices].
Nederlands Tijdschrift voor Geneeskunde 2009;
153(A 180).
- Wensing M, Baker R, Vedsted P et al. EUROPEP 2006.
Centre of Quality of Care Research, 2006. www.
topaseurope.eu/files/Europep%202006rapport_0.pdf
- Commonwealth Fund. International Health Policy Survey
of Adults’ Experiences with Primary Care. Commonwealth
Fund: New York, 2004.
- Commonwealth Fund. Health Care Quality Survey.
Commonwealth Fund: New York, 2006.
- Commonwealth Fund. International Health Policy Survey
of Sicker Adults. Commonwealth Fund: New York,
2008.
- Commonwealth Fund. Survey on Disparities in Quality of
Health Care. Commonwealth Fund: New York, 2001.
- Commonwealth Fund. International Health Policy Survey
of Adults with Health Problems. Commonwealth
Fund: New York, 2002.
- Shi L, Starfield B, Xu J. Validating the Adult Primary
Care Assessment Tool. Journal of Family Practice 2001;
50(2):161–75w.
- Delnoij DM, Rademakers JJ, Groenewegen PP. The
Dutch Consumer Quality Index: an example of stakeholder
involvement in indicator development. BMC
Health Services Research 2010;10:88.
- Bensing JM, Deveugele M, Moretti F et al. How to make
the medical consultation more successful from a
patient’s perspective? Tips for doctors and patients
from lay people in the United Kingdom, Italy, Belgium
and the Netherlands. Patient Education and Counseling
2011;84:287–93.
- Engels Y, Campbell S, DautzenbergMet al. Developing a
framework of, and quality indicators for, general practice
management in Europe. Family Practice 2005;
22:215–22.
- Boerma W, Kringos DS, Verschuuren M, Pellny M, Bulc
M. Primary Care Quality Management in Slovenia, 2008.
WHO, Copenhagen. https://www.nivel.nl/sites/default/
files/bestanden/Primary-care-quality-management-in-
SLOV.pdf
- Westert GP, Schellevis FG, Bakker DH, Groenewegen
PP, Bensing JM, Van der Zee J. Monitoring health
inequalities through general practice: the Second Dutch
National Survey of General Practice. European Journal of
Public Health 2005;15:59–65.
- Kringos DS et al. A snapshot of the organization and
provision of primary care in Turkey. BMC Health
Services Research 2011;11:90.
- Australian Capital Territory Department of Health. GP
Snapshot Survey. Australian Capital Territory Department
of Health: Canberra, 2009.
- Centers for Disease Control and Prevention. National
Ambulatory Medical Care Survey 2010. Centers for
Disease Control and Prevention: Atlanta, 2009.
- Eurostat. European Health Interview Survey. Eurostat:
Luxembourg, 2008.
- Tufts Medical Center ifCRaHPS. Ambulatory Care Experiences
Survey (ACES). Tufts Medical Center: Boston,
2003.
- Leiblum SR, Schnall E, Seehuus M, DeMaria A. To
BATHE or not to BATHE: patient satisfaction with visits
to their family physician. Clinical Research and Methods
2008;40:407–11.
- Agha Z, Schapira RM, Laud PW, McNutt G, Roter DL.
Patient satisfaction with physician-patient communication
during telemedicine. Telemedicine and e-Health
2009;15:830–9.
- CAHPS. Adult Primary Care Questionnaire 1.0: Clinician
&Group Survey (6-points scale). AHRQ, Rockville, 2009.
- National Primary Care Research and Development
Centre. General Practice Assessment Questionnaire
(GPAQ). National Primary Care Research and Development
Centre: Manchester, 2010.
- Zebiene E, Svab I, Sapoka V et al. Agreement in patientphysician
communication in primary care: a study from
Central and Eastern Europe. Patient Education and
Counseling 2008;73:246–50.
- Howie JG, Heaney DJ, Maxwell M, Walker JJ, Freeman
GK, Rai H. Quality at general practice consultations:
cross-sectional survey. BMJ 1999;319(7212):738–43.
- McGuiness C, Sibthorpe B. Development and initial
validation of a measure of coordination of health care.
International Journal of Quality in Health Care 2003;
15:309–18.
- National Health Service. The National Surveys of NHS
Patients: general practice 2002 – questionnaire. National
Centre for Social Research, Middlesex. 2002.
- Bindman AB, Grumbach K, Osmond D et al. Preventable
hospitalizations and access to health care. JAMA
1995;274:305–11.
- Van de Lisdonk EH. Nijmeegse Verwachtingen Lijst
[Expectancies List from Nijmegen]. https://www.nivel.nl/
sites/default/files/bestanden/ns2_r2_h07.pdf. 1985.
- UNESCO. International Standard Classification of Education
(ISCED). https://www.unesco.org/education/information/
nfsunesco/doc/isced_1997.htm. 1997.
- Hodgetts G, Broers T, Godwin M. Smoking behaviour,
knowledge and attitudes among family medicine physicians
and nurses in Bosnia and Herzegovina. BMC
Family Practice 2004;5:12.
- Himmel W, Kochen MM. How do academic heads of
departments of general practice organize patient care?
A European survey. British Journal of General Practice
1995;45(394):231–4.
- Van den Brink-Muinen A, Van Dulmen AJ, Bensing JM.
Eurocommunication II: a comparative study between
countries in Central and Western Europe on doctor–
patient communication in general practice: final report.
NIVEL: Utrecht, 2003. www.nivel.nl/sites/default/files/
bestanden/EurocommunicationII.pdf
- Sandvik H, Cho HJ. Attitudes to family practice registration
programmes. Survey of Korean and Norwegian
family doctors. Family Practice 2002;19:72–6.
- Agosta LJ. Patient satisfaction with nurse practitioner
delivered primary health care services. Louisiana State
University and Agricultural and Mechanical College.
Unpublished, 2005. etd.lsu.edu/docs/available/etd-
07012005–130406/unrestricted/Agosta_dis.pdf
- Ahlen GC, Mattsson B, Gunnarsson RK. Physician
patient questionnaire to assess physician patient agreement
at the consultation. Family Practice 2007;24:498–
503.
- Allan J, Schattner P, Stocks N, Ramsay E. Does patient
satisfaction with general practice change over a decade?
BMC Family Practice 2009;10:13.
- Baker D, Mead N, Campbell S. Inequalities in morbidity
and consulting behaviour for socially vulnerable groups.
British Journal of General Practice 2002;52(475):124–30.
- Baker R, Boulton M, Windridge K, Tarrant C, Bankart J,
Freeman GK. Interpersonal continuity of care: a crosssectional
survey of primary care patients’ preferences
and their experiences. British Journal of General Practice
2007;57(537):283–9.
- Barry DT, Moore BA, Pantalon MV et al. Patient satisfaction
with primary care office-based buprenorphine/
naloxone treatment. Journal of General Internal Medicine
2007;22:242–5.
- Berendsen AJ, Groenier KH, de Jong GM et al. Assessment
of patients’ experiences across the interface between
primary and secondary care: Consumer Quality
Index continuum of care. Patient Education and Counseling
2009;77:123–7.
- Agency for Healthcare Research and Quality, Rockville.
CAHPS. American Indian Survey. 2009 March 4.
- Department of Community and Family Medicine. Duke
Health Profile. Duke University Medical Center, Durham,
N.C. USA, 2007.
- Department of Human Services. Victorian Population
Health Survey. Victorian Government Department of
Human Services, Melbourne, Victoria, 2007.
- Esch BM. Patient satisfaction with primary care: an
observational study comparing anthroposophic and
conventional care. Health and Quality of Life Outcomes
2008;6:74. https://www.ncbi.nlm.nih.gov/pmc/articles/
PMC2570361/
- Euroqol. EQ 5D [This is a sample questionnaire-it needs
to be applied for]. EuroQol Group, Rotterdam, 2010.
- Fleming NS, Herrin J, Roberts W, Couch C, Ballard DJ.
Patient-centeredness and timeliness in a primary care
network: baseline analysis and power assessment for
detection of the effects of an electronic health record.
Proceedings (Baylor University Medical Center) 2006;
19:314–19.
- Frostholm L, Fink P, Oernboel E et al. The uncertain
consultation and patient satisfaction: the impact of
patients’ illness perceptions and a randomized controlled
trial on the training of physicians’ communication
skills. Psychosomatic Medicine 2005;67:897–905.
- Gagnon M, Hebert R, Dube M, Dubois MF. Development
and validation of the Health Care Satisfaction
Questionnaire (HCSQ) in elders. Journal of Nursing
Measurement 2006;14:190–204.
- Garratt AM, Danielsen K, Forland O, Hunskaar S. The
Patient Experiences Questionnaire for Out-of-Hours
Care (PEQ-OHC): data quality, reliability, and validity.
Scandinavian Journal of Primary Health Care 2010;
28(2):95–101.
- Glasgow RE, Emont S, Miller DC. Assessing delivery of
the five ‘As’ for patient-centered counseling. Health
Promotion International 2006;21:245–55.
- Grunfeld E, Fitzpatrick R, Mant D et al. Comparison
of breast cancer patient satisfaction with follow-up in
primary care versus specialist care: results from a
randomized controlled trial. British Journal of General
Practice 1999;49(446):705–10.
- Hadjistavropoulos H, Biem H, Sharpe D, Bourgault-
Fagnou M, Janzen J. Patient perceptions of hospital
discharge: reliability and validity of a Patient Continuity
of Care Questionnaire. International Journal for Quality
in Health Care 2008;20:314–23.
- Hathorne G, Richardson J, Day N. Using the Assessment
of Quality of Life (AQoL) Version 1. 2010. https://
www.buseco.monash.edu.au/centres/che/pubs/tr12.pdf
- Jiang L, Gan C, Kao B et al. Consumer satisfaction with
public health care in China. Journal of Social Sciences
2009;5:223–35.
- Kersnik J, Ropret T. An evaluation of patient satisfaction
amongst family practice patients with diverse ethnic
backgrounds. Swiss Medical Weekly 2002;132(9–10):
121–4.
- Kinnersley P, Stott N, Peters T, Harvey I, Hackett P. A
comparison of methods for measuring patient satisfaction
with consultations in primary care. Family Practice
1996;13:41–51.
- Chu-Weininger MY, Balkrishnan R. Consumer satisfaction
with primary care provider choice and associated
trust. BMC Health Services Research 2006;6:139. www.
biomedcentral.com/1472–6963/6/139
- Mahfouz AA, Al Sharif AI, El Gama MN, Kisha AH.
Primary health care services utilization and satisfaction
among the elderly in Asir region, Saudi Arabia. East
Mediterranean Health Journal 2004;10:365–71.
- Marcinowicz L, Rybaczuk M, Grebowski R, Chlabicz S.
A short questionnaire for measuring the quality of
patient visits to family practices. International Journal
for Quality in Health Care 2010;22:294–301.
- National Primary Care Research and Development
Centre. Out-of-Hours Patient Questionnaire. NPCRDC,
Manchester, 2007.
- NHS Department of Health. The GP Patient Survey
Questionnaire. Department of Health: London, 2010.
- Pyper C, Amery J, Watson M, Crook C. Access to
electronic health records in primary care – a survey of
patients’ views. Medical Science Monitor 2004;10(11):
SR17–22.
- Safran DG, Kosinski M, Tarlov AR et al. The Primary
Care Assessment Survey: tests of data quality and
measurement performance. Medical Care 1998;36:728–
39.
- Salisbury C, Burgess A, Lattimer V et al. Developing a
standard short questionnaire for the assessment of
patient satisfaction with out-of-hours primary care.
Family Practice 2005;22:560–9.
- Statistics Canada. Canadian Community Health Survey
2009 Questionnaire. Statistics Canada: Ottawa, 2009.
- Steine S, Finset A, Laerum E. A new, brief questionnaire
(PEQ) developed in primary health care for measuring
patients’ experience of interaction, emotion and consultation
outcome. Family Practice 2001;18:410–18.
- Takemura Y, Liu J, Atsumi R, Tsuda T. Development of a
questionnaire to evaluate patient satisfaction with medical
encounters. Tohoku Journal of Experimental Medicine
2006;210:373–81.
- Commonwealth Fund. International Health Policy Survey.
Commonwealth Fund, New York, 2001.
- Thom DH, Tirado MD, Woon TL, McBride MR. Development
and evaluation of a cultural competency
training curriculum. BMC Medical Education 2006;6:38.
- Uiters E. Primary Health Care Use among Ethnic Minorities
in the Netherlands: a comparative study. NIVEL,
Utrecht, 2007. www.nivel.nl/sites/default/files/bestanden/ Primary-health-care-use-among-ethnic-minorities-inthe-
Netherlands-a-comparative-study-2007.pdf
- Van der Feltz-Cornelis CM. Patient–Doctor Relationship
Questionnaire (PDRQ-9) in primary care: development
and psychometric evaluation. General Hospital Psychiatry
2004;26:115–20.
- van Uden CJ, Ament AJ, Hobma SO, Zwietering PJ,
Crebolder HF. Patient satisfaction with out-of-hours
primary care in the Netherlands. BMC Health Services
Research 2005;5(1):6.
- Van der Zee KI, Sanderman R. Het meten van de
algemene gezondheidstoestand met de RAND-36 [Dutch
version: Measuring general health status by SF-36].
Noordelijk Centrum voor Gezondheidsvraagstukken:
Groningen, 2010.
- Wensing M, van Lieshout J, Jung HP, Hermsen J,
Rosemann T. The Patients Assessment Chronic Illness
Care (PACIC) questionnaire in the Netherlands: a
validation study in rural general practice. BMC Health
Services Research 2008;8:182.
- Williams GC, Ryan RM, Deci EL. Health Care, Self-
Determination Theory Questionnaire. 2010. www.self
determinationtheory.org/questionnaires/10-questionnaires/
51
- Yancy WS Jr, Macpherson DS, Hanusa BH et al. Patient
satisfaction in resident and attending ambulatory care
clinics. Journal of General Internal Medicine 2001;16:
755–62.
- Carter M, Roland M, Bower P, Gask L, Greco M, Jenner
D. Improving your Practice with Patient Surveys.
NPCRDC: Manchester, 2005.
- Kerssens JJ, Groenewegen PP, Sixma HJ et al. Comparison
of patient evaluations of health care quality in
relation to WHO measures of achievement in 12
European countries. Bulletin of the World Health
Organization 2004;82(2):106–14.
- Zebiene E, Svab I, Sapoka V et al. Agreement in patientphysician
communication in primary care: a study from
Central and Eastern Europe. Patient Education and
Counseling 2008;73:246–50.

