Keywords
injuries; Pancreas; Wounds, Nonpenetrating
Abbreviations
AAST: American Association for the Surgery of Trauma; GCS: Glasgow coma scale; ISS: injury severity score; OIS: organ injury scale
INTRODUCTION
Injury to the pancreas after blunt abdominal trauma is less frequent than that of other solid organs, such as the liver and spleen. Pancreatic injuries rarely occur alone and are often associated with other intra-abdominal injuries [1]. Hence, these patients must be managed as all other trauma patients with the aim of ensuring hemodynamic stability first before any specific treatment of the pancreatic injuries if such treatment is required.
With the increasing adoption of non-operative management in blunt abdominal trauma [1], an accurate diagnosis of pancreatic injury is of paramount importance due to its numerous associated complications [2]. However, this is often difficult preoperatively due to its retroperitoneal location, the lack of early clinical signs and suboptimal standard investigations [2].
Surgical management of pancreatic trauma remains debatable with options ranging from simple drainage to pancreaticoduodenectomy, each with their benefits and associated complications. All these issues prompted us to review our institution’s experience of pancreatic injuries after blunt abdominal trauma and to highlight the various challenges in its management.
METHODS
Study Population
All patients in this study were treated at Tan Tock Seng Hospital from December 2002 to June 2008. Tan Tock Seng Hospital is a 1,300 bed hospital in Singapore which provides medical care to over 1.5 million people. It handles the highest number of trauma patients in Singapore and admits an average of 1,000 severe trauma patients yearly, of which 96% are for blunt injuries, with 40% of trauma admissions having an injury severity score (ISS) of more than 16 (unpublished personal data).
All patients with blunt abdominal trauma were initially reviewed in the Emergency Department by the emergency physicians and trauma surgeons. Any patient who was persistently hemodynamically unstable from a suspected abdominal injury which was refractory to resuscitation or with other definite indications for exploratory laparotomy warranted immediate surgery. Otherwise, computed tomography CT) scans were routinely performed for these patients straight from the Emergency Department.
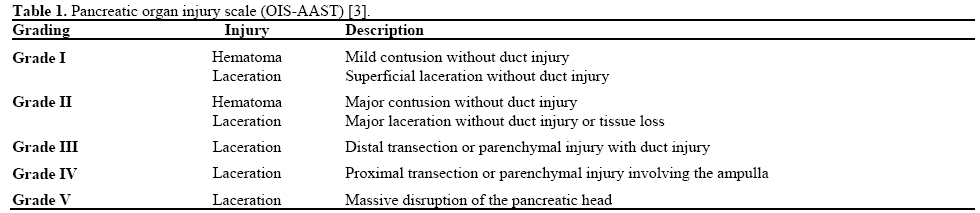
Our study included all cases with pancreatic injuries from blunt abdominal trauma which were diagnosed either through CT scans and/or during exploratory laparotomy. Patients were excluded if they suffered penetrating injuries. The data collected include the patient’s age, gender, mechanism of injury, initial vital signs, ISS, selected investigations, laparotomy observations, severity of pancreatic injuries and the eventual outcome. All trauma patients were managed by one dedicated surgical trauma team in the institution. Pancreatic injuries were graded according to the pancreatic injury severity score (organ injury scale as defined by the American Association for the Surgery of Trauma (OIS-AAST) (Table 1) [3].
STATISTICS
Median, range, and frequencies were reported as descriptive statistics.
ETHICS
Oral consent was obtained from each patient. The patients were treated according to the ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004.
RESULTS
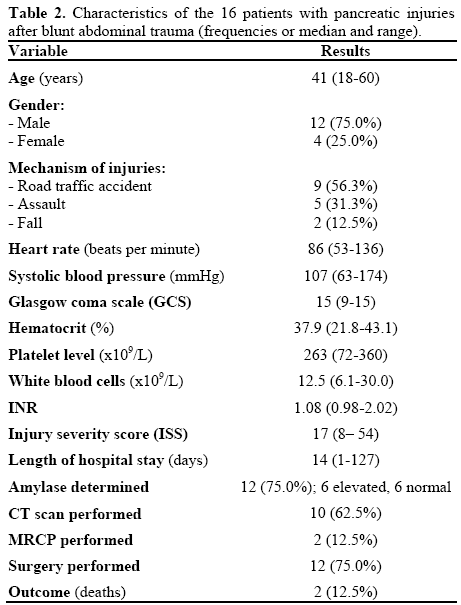
From December 2002 to June 2008, 16 patients having a median age of 41 years (range: 18-60 years) formed the study group. All patients arrived at the Emergency Department within 2 hours from the alleged incident. There was a male predominance of 75% (n=12) and motor vehicle collisions and blunt assault from assailants accounted for 56.3% (n=9) and 31.3% (n=5) of the injuries, respectively. According to the AAST grading for pancreatic injury, grade I injury was present in 4 (25.0%) patients, grade II in 7 (43.8%), grade III in 2 (12.5%), grade IV in 2 (12.5%) and grade V in1 (6.3%).
The median Glasgow coma scale (GCS) [4] on arrival was 15 (range: 9-15) while median heart rate and systolic blood pressure were 86 beats per minute (bpm) (range: 53-136 bpm) and 107 mmHg (range: 63-174 mmHg), respectively. Review of the initial hematological investigations showed a median hematocrit of 37.9% (range: 21.8-43.1%; reference range: 33-45%), median platelet level of 263 x109/L (range: 72-360 x109/L; reference range: 170-420 x109/L), median white blood cells of 12.5 x109/L (range: 6.1-30.0 x109/L; reference range: 4-10 x109/L) and median INR of 1.08 (range: 0.98-2.02). Serum amylase estimation was carried out in 12 patients (75.0%), for which only 6 (50.0%) had elevated levels which were not related to the grading of the pancreatic injury. Table 2 reports the various characteristics of the study group.
Six (37.5%) patients were immediately sent to the operating theatre from the Emergency Department due to refractory hemodynamic instability in the presence of suspected hemoperitoneum after focused assessment with sonography for trauma with or without the aid of diagnostic peritoneal lavage. In these 6 patients, almost all (n=5; 83.3%) had massive associated intraabdominal injuries which resulted in significant intraabdominal hemorrhage, ranging from major vessel laceration to massive lacerations of the liver. The two patients with grades IV and V pancreatic lacerations died from circulatory collapse due to the associated injuries within 12 hours post-operatively without any definitive resection performed. One patient had grade III injury for which a distal pancreatectomy was performed. The other three patients had grade II injuries which were managed with external drainage. Pre-operative CT scans (Figure 1) were performed in the other 10 (62.5%) patients, with four of them managed non-operatively. The remaining six were operated on after evaluation of their CT scans, all within 6 hours after the CT scans. Some of these CT scan findings included pancreatic transection, active contrast extravasation from the pancreas and massive splenic rupture. In this group of six patients, a distal pancreatectomy was performed in one patient with grade III injury while pancreaticoduodenectomy (Whipple procedure) was performed in the other patient with grade IV injury. The remaining patients had their pancreatic injuries managed with external drainage. Table 3 reports the grading and management of the pancreatic injuries in our series.
Figure 1: CT scan showing peripancreatic hematoma.

In one patient with pancreatic head contusion and questionable pancreatic duct status, an intraoperative cholecystogram was carried out through the gallbladder which failed to visualize the pancreatic duct. Hence, a duodenotomy was performed, and cannulation of the ampulla of Vater with pancreatography showed normal integrity of the pancreatic duct. The duodenotomy was then closed using interrupted sutures. Unfortunately, this patient subsequently developed a leak from the duodenotomy site and subsequently presented as an intra-abdominal abscess which necessitated percutaneous drainage. He also required another exploratory laparotomy as his condition did not improve and drainage of the abscess was performed; no obvious leak was detected intraoperatively. He was discharged eventually in good condition after a 4-month stay.
Endoscopic retrograde cholangiopancreatography (ERCP) was not carried out in our series but magnetic resonance cholangiopancreatography (MRCP) was performed in 2 (12.5%) patients postoperatively and confirmed the integrity of the pancreatic ducts.
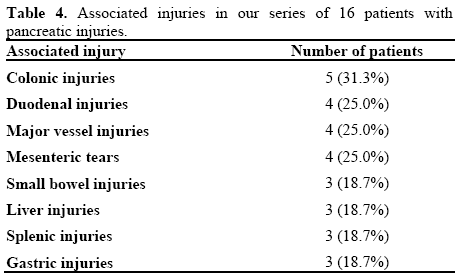
In the four patients with duodenal injuries diagnosed during exploratory laparotomy, one underwent pancreaticoduodenectomy while the other three had their duodenal contusion treated conservatively. There were also four patients with major vascular injuries from the portal vein, superior mesenteric vein (n=2) and splenic vein. Two of them died eventually from their injuries.
Other significant intra-abdominal findings included colonic injuries in five patients (80.0%), mesenteric tears in four (25.0%) and splenic injuries in three (18.8%). Table 4 illustrates the various associated intra-abdominal injuries in our series.
Outcome
The median ISS was 17 (range: 8-54), and the median length of inpatient stay was 14 days (range: 1-127 days). As previously mentioned, the two (12.5%) patients with grade IV and V pancreatic injuries died from significant blood loss due to their associated injuries. Their injury severity scores were 34 and 55, respectively, and both were already in significant hemodynamic compromise in the Emergency Department.
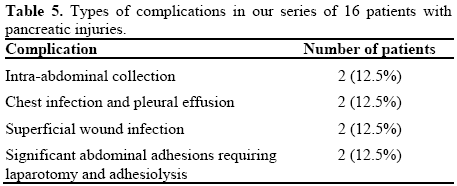
Intra-abdominal abscess was seen in two (12.5%) of our patients. One resulted from the intraoperative duodenotomy as previously described which eventually necessitated another laparotomy while the other had the emergency Whipple procedure initially and was subsequently diagnosed with the abscess after he complained of abdominal pain and evidence of sepsis several days postoperatively. Percutaneous drainage of the abscess was successful and both were discharged in good condition. Other complications included chest infection with pleural effusion (n=2; 12.5%) and superficial wound infection (n=2; 12.5%). There were two patients (12.5%) who developed severe abdominal pain within 3 weeks after the initial exploratory laparotomy. After numerous investigations, the cause in both cases was attributed to intestinal obstruction secondary to adhesions. Both eventually underwent laparotomy and adhesiolysis after failure of conservative measures. Table 5 reports the complications in our series.
DISCUSSION
The incidence of pancreatic injuries after blunt abdominal trauma is very low, with rates of less than 1% quoted for all trauma admissions [5]. However, missed pancreatic injuries are often associated with numerous complications, such as pancreatitis, pancreatic fistula, abscess and pseudocysts [6]. Furthermore, the increasing adoption of non-operative management for blunt abdominal trauma [1] has only served to focus attention on the importance of accurate identification of the presence and extent of the pancreatic insults. However, the diagnosis of pancreatic injuries is challenging for several reasons: the lack of early physical signs, its retroperitoneal location and the unreliability of current standard diagnostic modalities [2].
Pancreatic injuries occur after blunt trauma when the pancreas is crushed against the vertebrae. The spectrum of injuries ranges from minor contusions to massive disruption of the pancreatic head [7]. In addition, pancreatic injuries rarely occur by themselves and are often associated with other intra-abdominal injuries, such as those of the liver, duodenum and major vessels [8]. Hence, the immediate priority in managing these patients must be to control any significant hemorrhage while any definitive treatment can only commence when the patient has been stabilized.
Amylase
Serum amylase estimation has been reported to be neither specific nor sensitive for diagnosing pancreatic injuries [9]. Even if elevated, there is no correlation to the severity of the injury [9]. This was also seen in our series. Nonetheless, some authors have cited a sensitivity of up to 75% when correlating elevated serum amylase levels to pancreatic injuries [10]. In our institution, serum amylase is never used for determining the severity of pancreatic injuries due to the prompt availability of CT scans or urgent surgery depending on the hemodynamic stability of the patients. However, a persistently elevated serum amylase level after the initial insult requires exclusion of a pancreatic fistula or other complications.
Computed Tomography (CT) Scan
The role of a CT scan in the evaluation of intraabdominal injuries after blunt trauma for hemodynamically stable patients is well established [11]. Apart from accurate identification and staging of the various injuries, a CT scan also guides subsequent management, be it operative or non-operative, especially in hepatic and splenic injuries [11]. Its role in pancreatic injuries has been questioned by several authors. But, since the introduction of multidetector CT scanners, the sensitivity and specificity of CT scans in detecting pancreatic injuries has been quoted to be as high as 91% [12]. Some of the CT findings suggestive of pancreatic injuries include peripancreatic fluid in the lesser sac; pancreatic hematoma or laceration and focal edema at the site of the injury [12]. Lacerations greater than 50% of the pancreas raise the suspicion of duct injury, but even smaller lacerations can involve the duct. As there remains a risk of missing or underestimating the severity of pancreatic trauma, a low threshold for repeat CT scanning must be adopted, especially in the presence of persistent symptoms.
CT scans are also often used in the detection of complications following pancreatic trauma. Some of these include pseudocysts, abscesses and fistulae. CTguided drainage procedures can be performed to minimize the necessity of any further operative intervention.
Endoscopic Retrograde Cholangiopancreatography (ERCP)
ERCP is an invaluable tool in the overall management of pancreatic trauma. In the early stages or preoperatively, it is able to provide real-time diagnostic images and allow guided intervention [13]. It can even be performed intraoperatively or in the late stages of pancreatic trauma. Apart from demonstrating the nature and extent of any ductal injuries, stenotic segments can also be diagnosed. Through its interventional ability by placement of an endoscopic stent, major surgery can be averted even in the presence of pancreatic ductal injuries [13]. However, in certain circumstances such as pancreatic tail ductal injuries, surgical resection may be preferred instead of stenting due to the associated complications of repeated ERCP, stent exchange and ductal stricture [14]. ERCP is also useful in managing post-injury or post-operative complications. Pseudocysts, pancreatic fistulae and chronic pancreatitis are some of these conditions which could be diagnosed and managed endoscopically without major surgery [13, 14].
Though some have advocated emergency intraoperative ERCP in the evaluation of ductal integrity and subsequent intervention, many of these patients are often poor candidates because of limited resources and lack of surgical expertise, hemodynamic instability, associated injuries and the risks of prolonged surgery [13, 14]. The authors advocate ERCP in patients who are hemodynamically stable with suspected pancreatic injury, especially if there is evidence of pancreatic injury from the CT scan or MRCP. Another useful situation would be when post-injury or postoperative complications are suspected. The benefits of ERCP have to be balanced with its numerous complications, such as bleeding, pancreatitis and perforation.
Magnetic Resonance Cholangiopancreatography (MRCP)
MRCP is a non-invasive diagnostic tool which is capable of evaluating pancreatic injuries with a high sensitivity and specificity [15]. It avoids the risks of pancreatitis, hemorrhage and gastrointestinal perforation associated with ERCP. Hence, MRCP has gradually been adopted as an adjunctive test in the diagnosis and management of pancreatic injury, especially in those with suspected pancreatic ductal involvement. Furthermore, no contrast material or radiation is required. Any positive MRCP finding would necessitate ERCP or even surgical intervention. However, its purely diagnostic nature and its inability to provide real-time visualization of ductal filling and extravasation are some of its disadvantages. In addition, the time taken for MRCP to be performed has restricted its usage to only hemodynamically stable patients [15].
Surgery
In patients who are hemodynamically unstable and in whom there is no prior knowledge of the nature and extent of the intra-abdominal injuries, any trauma laparotomy must begin with a long midline incision with the main aim of localizing and controlling massive bleeding, and limiting gastrointestinal contamination. Once achieved or excluded, a thorough laparotomy to assess the rest of the abdomen can proceed.
The intraoperative features suggestive of pancreatic trauma include blood in lesser sac, retroperitoneal hematoma in the upper abdomen, peripancreatic hematoma and injury to the second part of the duodenum [7, 16]. Should pancreatic injuries be suspected, optimal visualization and mobilization is mandatory.
Entry into the lesser sac by detaching the greater omentum from the transverse colon is one of the key steps in visualizing the pancreas. Kocherisation of the duodenum and mobilization of the hepatic flexure and transverse colon should be performed if injuries of the duodenum, or the pancreatic head or neck are suspected. However, if injuries to the tail of the pancreas are suspected, adequate mobilization of the spleen may be required.
Integrity of the main pancreatic duct is one of the most important factors in determining the outcome of patients with pancreatic injuries [6, 7]. Patients with pancreatic duct injuries are associated with an increased incidence of pancreatic-related complications, especially pancreatic fistulae and pseudocysts [6]. Non-operative evaluation, using a CT scan, ERCP and MRCP, has already previously been discussed. Intraoperatively, there are several approaches for evaluating the condition of the pancreatic duct. The easiest approach is to perform an intraoperative cholangiogram through the cystic duct, common bile duct or even through the gallbladder [6, 16]. However, if this is unsuccessful, cannulation of the pancreatic duct via a transduodenal approach, through the transected tail of the pancreas or by concomitant ERCP are also possible [6, 16]. In situations wherein injury to the distal pancreatic duct is suspected, distal pancreatectomy without definitive proof of ductal injury is a recognized treatment option [17]. However, caution must be taken in performing these invasive investigative procedures in view of the possible complications as was seen in one of our patients.
First and foremost, any trauma surgeons must realize that any definitive pancreatic surgery must be balanced against the patient’s hemodynamic stability, associated injuries and the implications of lengthy, extensive and complicated reconstructive pancreatic surgery. Some of the considerations which determine the type of pancreatic surgery performed would include the degree and exact location of the parenchymal injury and the integrity of the main pancreatic duct.
For grade I and II injuries, adequate hemostasis, debridement and external drainage are usually sufficient [16, 18]. Adequate drainage will reduce the risk of both pancreatic abscesses and fistulae. Nonoperative management has also been shown to be successful without significant complications [2]. While some advocate repair of a capsular laceration, others have shown that closure would lead to the formation of a pancreatic pseudocyst and hence is not advised. Distal pancreatic transection is most commonly managed with a distal pancreatectomy using a stapling device which is effective and rapid [7, 16, 17]. Although preservation of the spleen is ideal, the benefits in spleen preservation in adults are not as significant as compared to children. In addition, elaborate maneuvers to save the spleen are not recommended in a trauma setting. However, in situations when the major pancreatic duct is lacerated, drainage alone would not be adequate as it invariably leads to a fistula and possibly to a peripancreatic abscess. If identification of the duct was performed pre-operatively and the injury was amenable to stenting, ERCP-guided stenting would be a practical option so as to avoid major surgery. However, if the diagnosis is only achieved intra-operatively, the site of the injury would be instrumental in the procedure adopted. Options then would include intra-operative ERCP-guided stenting for ductal injuries at the head without much pancreatic head disruption whereas distal pancreatectomy using a stapling device would suffice for injuries of the body or tail. Any surgery for pancreatic head ductal injuries is a major undertaking; surgical options would then include pancreaticoduodenectomy or a Roux-en-Y pancreaticojejunal loop with external drainage.
The intimate connections between the duodenum, common bile duct and pancreatic head make management of massive pancreatic head disruption extremely challenging. More often than not, patients with massive pancreatic head disruption are frequently have other life-threatening injuries and merit an initial damage control approach with packing and external drainage [8, 16].
Even though one of our patients survived an emergency pancreaticoduodenectomy, this procedure often carries a prohibitive high mortality and morbidity rate and is best reserved for the severe case of destruction of the head of the pancreas and duodenum in an extremely hemodynamically stable patient [7, 19]. A two-stage procedure could also be performed after an initial damage control laparotomy with drainage. In minor pancreaticoduodenal injuries, primary duodenal repair and pancreatic drainage may be adequate. However, in other situations where severe pancreaticoduodenal injuries are encountered, options such as pyloric exclusion with gastrojejunostomy and duodenal diverticulization can be performed with pyloric exclusion being the preferred procedure [7, 16].
Outcome
The mortality rate after pancreatic trauma has been reported to be as high as 46% and is usually caused by the associated injuries. In our series, although the rate was only 12.5%, it was nonetheless a small series with a predominant prevalence of grade I and II injuries. The main morbidities from pancreatic trauma typically arise from pancreatic-specific complications. The risks of developing these complications correspond to the grades of injury [20, 21] and especially if injuries were not detected. Thus, there must be a low threshold for performing a CT scan, MRCP or even ERCP if there is a clinical or biochemical suspicion of these complications.
which results from pancreatic duct injury which was not identified or properly dealt with initially [16, 20]. Although most pancreatic fistulae resolve spontaneously and resolve within 1-2 weeks after injury, adequate external drainage and nutritional support must be ensured. Definitive management of these fistulae would include ERCP stenting, surgical intervention if stenting failed or was not appropriate, or when the fistula has a persistently high output [6, 7]. A distal pancreatectomy is recommended for fistulae of the body and tail while a Roux-en-Y gastrojejunostomy may be required for pancreatic head ductal injuries.
Pancreatic abscesses are not uncommon and targeted antibiotics with drainage via operative, radiologic or endoscopic modalities are often adequate [6, 7]. While mild pancreatitis is often self-limiting, life threatening situations may arise should hemorrhage pancreatitis develop. Erosions of the surrounding vessels may occur from auto-digestion and options would then include angiographic embolization or surgical intervention [6, 7].
Pancreatic pseudocyst formation may present weeks to months after the initial insult. Definitive management depends on the integrity of the pancreatic duct. If the pancreatic duct is intact, percutaneous drainage is usually adequate. However, if disruption of the pancreatic duct is diagnosed, options include endoscopic stenting or surgery [16].
In certain instances, late complications of undetected pancreatic trauma may present months to years after the initial insult and these can be difficult to diagnose [20, 21]. Some of the presentations include chronic pancreatitis, pancreatic fistulae, abscesses or pseudocysts. A careful history and clinical examination followed by radiological investigations such as CT scan, ERCP or MRCP is often required. Definitive surgery is often required to avoid further complications.
Limitations
There were several limitations in the present study. This small series of patients was enrolled from a single institution and the data were retrospectively reviewed. Although these limitations are significant, this study highlights the numerous issues surrounding blunt traumatic pancreatic injuries which are not commonly discussed in the literature.
CONCLUSION
Blunt pancreatic trauma continues to pose significant diagnostic and therapeutic challenges. In view of the numerous associated injuries, priority must be given tostabilizing the patient before any definitive management of the pancreatic injury. Mortality in these patients is usually a result of the magnitude of their associated injuries.
Conflict of interest The authors have no potential conflicts of interest
References
- Miller PR, Croce MA, Bee TK, Malhotra AK, Fabian TC. Associated injuries in blunt solid organ trauma: implications for missed injury in nonoperative management. J Trauma 2002; 53:238- 42. [PMID 12169928]
- Duchesne JC, Schmieg R, Islam S, Olivier J, McSwain N. Selective nonoperative management of low-grade blunt pancreatic injury: are we there yet? J Trauma 2008; 65:49-53. [PMID 18580509]
- Moore EE, Cogbill TH, Malangoni MA, Jurkovich GJ, Champion HR, Gennarelli TA, et al. Organ injury scaling, II: Pancreas, duodenum, small bowel, colon, and rectum. J Trauma 1990; 30:1427-9. [PMID 2231822]
- Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974; 2:81-4. [PMID 4136544]
- Akhrass R, Yaffe MB, Brandt CP, Reigle M, Fallon WF Jr, Malangoni MA. Pancreatic trauma:a ten-year multi-institutional experience. Am Surg 1997; 63:598-604. [PMID 9202533]
- Kao LS, Bulger EM, Parks DL, Byrd GF, Jurkovich GJ. Predictors of morbidity after traumatic pancreatic injury. J Trauma 2003; 55:898-905. [PMID 14608163]
- Lin BC, Chen RJ, Fang JF, et al. Management of blunt major pancreatic injury. J Trauma 2004; 56:774-8. [PMID 15187739]
- Fleming WR, Collier NA, Banting SW. Pancreatic trauma:Universities of Melbourne HPB Group. Aust N Z J Surg 1999; 69:357-62. [PMID 10353551]
- Buechter KJ, Arnold M, Steele B, Martin L, Byers P, Gomez G, Zeppa R, Augenstein J. The use of serum amylase and lipase in evaluating and managing blunt abdominal trauma. Am Surg 1990; 56:204-8. [PMID 1694634]
- Takishima T, Sugimoto K, Hirata M, et al. Serum amylase level on admission in the diagnosis of blunt injury to the pancreas:its significance and limitations. Ann Surg 1997; 226:70-6. [PMID 9242340]
- Poletti PA, Mirvis SE, Shanmuganathan K, Takada T, Killeen KL, Perlmutter D, et al. Blunt abdominal trauma patients: can organ injury be excluded without performing computed tomography? J Trauma 2004; 57:1072-81. [PMID 15580035]
- Wong YC, Wang LJ, Fang JF, Lin BC, Ng CJ, Chen RJ. Multidetector-row computed tomography (CT) of blunt pancreatic injuries: can contrast-enhanced multiphasic CT detect pancreatic duct injuries? J Trauma 2008; 64:666-72. [PMID 18332806]
- Thomas H, Madanur M, Bartlett A, Marangoni G, Heaton N, Rela M. Pancreatic trauma--12-year experience from a tertiary center. Pancreas 2009; 38:113-6. [PMID 19002020]
- Kim HS, Lee DK, Kim IW, Baik SK, Kwon SO, Park JW, Cho NC, Rhoe BS. The role of endoscopic retrograde pancreatography in the treatment of traumatic pancreatic duct injury. GastrointestEndosc 2001; 54:49-55. [PMID 11427841]
- Fulcher AS, Turner MA, Yelon JA, McClain LC, Broderick T, Ivatury RR, Sugerman HJ. Magnetic resonance cholangiopancreatography (MRCP) in the assessment of pancreatic duct trauma and its sequelae: preliminary findings. J Trauma 2000; 48:1001-7. [PMID 10866243]
- Degiannis E, Glapa M, Loukogeorgakis SP, Smith MD. Management of pancreatic trauma. Injury 2008; 39:21-9. [PMID 17996869]
- Cogbill TH, Moore EE, Morris JA Jr, Hoyt DB, Jurkovich GJ, Mucha P Jr, et al. Distal pancreatectomy for trauma: a multicenter experience. J Trauma 1991; 31:1600-6. [PMID 1749029]
- Canty TG Sr, Weinman D. Management of major pancreatic duct injuries in children. J Trauma 2001; 50:1001-7. [PMID 11428378]
- Heimansohn DA, Canal DF, McCarthy MC, Yaw PB, Madura JA, Broadie TA. The role of pancreaticoduodenectomy in the management of traumatic injuries to the pancreas and duodenum. Am Surg 1990; 56:511-4. [PMID 2375554]
- Leppäniemi A, Haapiainen R, Kiviluoto T, Lempinen M. Pancreatic trauma:acute and late manifestations. Br J Surg 1988; 75:165-7. [PMID 3349308]
- Stawicki SP, Schwab CW. Pancreatic trauma:demographics, diagnosis, and management. Am Surg 2008; 74:1133-45. [PMID 19097525]


