Keywords
neo adjuvant Therapy; Pancreatic Neoplasms; Radiation
Abbreviations
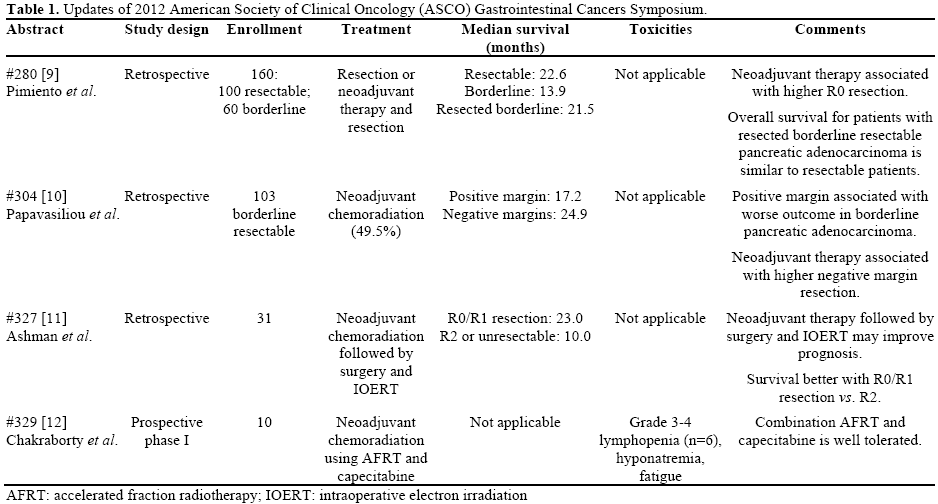
AFRT: accelerated fraction radiotherapy; IOERT: intraoperative electron irradiation
What We Knew About the Management of Borderline Resectable Pancreatic Adenocarcinoma Before the 2012 ASCO GI Cancers Symposium?
During the year 2011, an estimated 44,430 new cases of pancreatic adenocarcinoma were diagnosed in the United States. There were 36,800 deaths that were attributed to pancreatic adenocarcinoma [1]. Pancreatic adenocarcinoma is the fourth most common cause of adenocarcinoma-related death among U.S. men and women [1]. Despite enormous efforts in translational research, the prognosis of pancreatic adenocarcinoma remains extremely poor. The overall 5-year survival rate is less than 5% [2]. To date, the only potentially curative treatment for managing pancreatic adenocarcinoma is surgical resection. However, more than 80% of patients are deemed either unresectable or metastatic upon diagnosis [3].
To improve patient selection for surgery and to increase the likelihood of an R0 resection, an expert consensus group developed criteria to define tumor respectability in 2009 [4]. Using these criteria, tumors are classified as resectable, borderline resectable, or unresectable. Borderline resectable disease is defined as the absence of evidence of peritoneal or hepatic metastases following a thorough radiological assessment. Radiological findings of tumor abutment on the portal vein or superior mesenteric vein with venous deformity, and limited encasement of the mesenteric vein and portal vein represent the extent of venous involvement. Radiological findings suggesting borderline arterial involvement include encasement of a short segment of the hepatic artery, without evidence of tumor extension to the celiac axis and/or tumor abutment of the superior mesenteric artery involving less than 180 degrees of the artery circumference. This is open to the interpretation of the radiologist and the surgeon, because it is usually not based on operative findings.
An initial approach involving neo adjuvant therapy has been preferred, as opposed to immediate surgery, although there is no high-level evidence supporting its use and it is highly debatable in the setting of borderline resectable disease. Furthermore, no standard neo adjuvant treatment regimen exists for borderline resectable pancreatic adenocarcinoma. Similar paradigms as for locally advanced unresectable disease are being used. They include upfront fluoropyrimidinebased or upfront gemcitabine-based chemoradiation [5, 6, 7] or chemotherapy followed by chemoradiation [5, 8].
This highlight article will discuss four abstracts focusing on the management of borderline resectable pancreatic adenocarcinoma published at the 2012 American Society of Clinical Oncol ogy (ASCO) Gastrointestinal Symposium.
What Did We Learn at the 2012 ASCO GI Cancers Symposium?
Borderline Resectable Patients (Abstract #280 [9]
Pimiento et al. examined the outcome of multimodality therapy of patients with borderline resectable pancreatic adenocarcinomas. They retrospectively looked at 160 patients with operable pancreatic ductal adenocarcinoma. Among this cohort, 60 patients had borderline resectable tumors. All patient with borderline resectable tumors received neo adjuvant therapy and ultimately 58% received resection. The authors found that the median overall survival was 13.9 months for borderline resectable patients, inferior to 22.6 months for resectable patients. However, the median overall survival was 21.5 months among borderline resectable patients who received resection, similar to resectable patients.
neo adjuvant Therapy and Margin Status (Abstract #304 [10])
Papavasiliou et al. studied the influence of margin status and neo adjuvant chemoradiation therapy for borderline resectable pancreatic adenocarcinoma patients. They reviewed 103 patients with borderline resectability. Approximately half of this cohort received neo adjuvant chemoradiation therapy. From the entire cohort, microscopic margin status was positive in 54% of patients. Patients with microscopic positive margins had inferior median overall survival compared with microscopic negative margins (17.2 months vs. 24.9 months, respectively). Patients who received neo adjuvant therapy had a higher rate of negative margin resection than those who did not receive neo adjuvant chemoradiation (61.7% vs. 38.3%, respectively). The authors concluded that patients with positive margins had worse outcomes and that neo adjuvant chemoradiation was associated with higher rates of negative margin resection.
Intraoperative Electron Irradiation (Abstract #327 [11])
Ashman et al. reported their experience treating borderline resectable and unresectable pancreatic adenocarcinoma patients using neo adjuvant chemoradiation followed by surgery with intraoperative electron irradiation. Thirty-one patients who underwent resection were included in this analysis. Median overall survival was 19 months. Patients with R0/R1 resection had a better median overall survival than R2 and unresectable tumors (23 months vs. 10 months). The authors concluded that prognosis was associated with resection margin status. They also suggested performing prospective studies with the use of intraoperative electron irradiation.
Accelerate Fraction Radiotherapy with Capecitabine (Abstract #329 [12])
Chakraborty et al. reported a phase I study looking at novel neo adjuvant therapeutic approach using accelerated fraction radiotherapy with concomitant capecitabine for borderline resectable pancreatic adenocarcinoma. With 10 patients enrolled thus far, the authors showed moderate degrees of toxicity, primarily lymphopenia. Other toxicities include hyponatremia and fatigue. The authors concluded that accelerated fraction radiotherapy with capecitabine is relatively safe. Subsequent phase II studies will examine molecular mechanisms of treatment resistance.
The details of these four studies are summarized in Table 1.
Discussion
Management of borderline resectable pancreatic adenocarcinoma remains challenging and requires multi-disciplinary effort. This subgroup of pancreatic adenocarcinoma patients are determined to be potentially resectable. To achieve a favorable longterm outcome, it is critical to identify borderline resectable pancreatic adenocarcinoma and to treat preoperatively to maximize the potential for resection.
An important addition to the National Comprehensive Cancer Network (NCCN) guidelines [13] is a revised set of criteria based on a consensus of the panel members which defines borderline resectable pancreatic adenocarcinoma [4]. There are fewer problems for the conduct of neo adjuvant strategies in borderline resectable tumors, as the consensus is reached upon definition of resectability on imaging and margin positivity by expert radiologists and surgeons. With currently available surgical techniques, patients with borderline resectable pancreatic head adenocarcinoma are at high risk for a margin-positive resection. Therefore, the approach for these patients is to use preoperative systemic therapy and local-regional chemoradiation to maximize the potential for an R0 resection and to avoid R2 resections. In general, patients with favorable responses to preoperative therapy (radiographic evidence of tumor regression and improvement in serum tumor marker levels) are the subset of patients who have the best chance for an R0 resection and a favorable long-term outcome. NCCN guidelines [13] also further underline the importance of upfront systemic therapy prior to administration of chemoradiation therapy as upfront systemic therapy provides for disease control and allows selection of those patients most likely to benefit from subsequent chemoradiation.
Ashman et al. reported that neo adjuvant chemoradiation followed by surgery with intraoperative electron irradiation (IOERT) demonstrated promising survival benefit and showed an association of prognosis and resection margin status (Abstract #327 [11]). Survival was superior among patients for whom R0 or R1 resection was achieved (median survival 23 months vs. 10 months for R2 or unresected tumors. A study by Papavasiliou et al. showed that neo adjuvant chemoradiation was associated with higher rate of negative margin resection (62% vs. 38%, P=0.02) and better outcomes when compared to patients without neo adjuvant treatment (Abstract #304 [10]). A single institutional review study by Pimiento et al. demonstrated an improved overall survival for borderline resectable patients when treated with a multimodality therapy (Abstract #280 [9]). In this study, 58% of treated patients were ultimately resected. These patients had a similar median overall survival compared with resectable patients (21.5 months vs. 22.6 months, respectively). Though small in patient number, the resection rate was higher than previously reported (58% of 60 patients vs. 40% of 2,148 patients in a meta-analysis of 19 cohort studies [14]). One may argue that the respectability rate is heavily dependent on what patients are included and how aggressive the surgeons are willing to be. Centers that are willing to resect and reconstruct major vascular structures usually have a higher resectability rate. In this study, not only the resectability rate was high but also the R0 resection rate was higher than previously reported (56% vs. 31- 35%) [15, 16]. This result suggests that the multimodality therapy is promising and warrants further investigation.
A novel neo adjuvant approach using accelerated fraction radiotherapy with concomitant capecitabine in a phase I study has showed the tolerability (Abstract #329 [12]). A subsequent phase II study of this modality is underway to investigate the efficacy. To date, no randomized phase III trials have yet evaluated the approach of neo adjuvant therapy in borderline resectable disease compared to the approach of taking these patients to surgery upfront. The best regimens to use in the setting of borderline resectable disease remain unknown. Prospective studies of novel agents or combination regimen are needed in the setting of borderline resectable disease.
Conflict of interest
The authors have no potential conflicts of interest
References
- Siegel, R., et al. Cancer statistics, 2011: the impact of eliminating socio economic and racial disparities on premature cancer deaths. CA Cancer J Clin. 61(4): p. 212-36.
- Jemal, A., et al. Cancer statistics, 2009. CA Cancer J Clin, 2009.59(4): p. 225-49.
- Li, D., et al. Pancreatic cancer. Lancet, 2004. 363(9414): p.1049-57.
- Callery, M.P., et al. Pretreatment assessment of resectable and borderline resectable pancreatic cancer: expert consensus statement. Ann Surg Oncol , 2009. 16(7): p. 1727-33.
- Hassan, M.M., et al. Risk factors for pancreatic cancer: case control study. Am J Gastroenterol, 2007. 102(12): p. 2696-707.
- Arnold, L.D., et al. Are racial disparities in pancreatic cancer explained by smoking and overweight/obesity? Cancer Epidemiol Biomarkers Prev, 2009. 18(9): p. 2397-405.
- Jemal, A., et al., Cancer statistics, 2010. CA Cancer J Clin.60(5): p. 277-300.
- Lynch, S.M., et al. Cigarette smoking and pancreatic cancer: apooled analysis from the pancreatic cancer cohort consortium. Am J Epidemiol, 2009. 170(4): p. 403-13.
- Jose mario Pimiento, T.H., Jill M. Weber, Manish Patel, Pamela Joy Hodul, Michael Chuong, Gregory Springett, et al. Multimodality therapy for borderline resectable pancreatic cancer: A single institution experience. J Clin Oncol 2012. supple 4; abstr 280.
- Pavlos Papavasiliou, J.R.P., Rodrigo Arrangoiz, Kathryn T Chen, Fang Zhu, Yun Shin Chun, John Parker Hoffman. Marginstatus and neo Adjuvant chemoradiation in patients with borderline resectable pancreatic cancer. J Clin Oncol 2012. 30(suppl 4; abstr304).
- Jonathan Ben Ashman, A.A.M., Matthew D. Callister, Kunam S Reddy, David C Mulligan, Leonard L. Gunderson, Mitesh J. Boradneo Adjuvant chemoradiation and intraoperative electron irradiation for locally unresectable/borderline resectable pancreas adenocarcinoma. J Clin Oncol 2012. 30(suppl 4; abstr 327).
- Samhita Chakraborty, T.W.B., Monica M Morris, Erin Yarde, J Thomas Parsons, Reid B Adams, Hanna Kelly Sanoff. Accelerated fraction radiotherapy with concomitant capecitabine as neo adjuvant therapy of borderline resectable pancreatic cancer. J Clin Oncol 2012. 30(suppl 4; abstr 329).
- National Comprehensive Cancer Network. pancreatic adenocarcinoma (Version 2.2012). In: NCCN Clinical Practice Guidelines in Oncol ogy.
- Laurence, J.M., et al. A systematic review and meta-analysis ofsurvival and surgical outcomes following neo adjuvant chemoradiotherapy for pancreatic cancer. J Gastrointest Surg 15(11):p. 2059-69.
- McClaine, R.J., et al. neo adjuvant therapy may lead tosuccessful surgical resection and improved survival in patients with borderline resectable pancreatic cancer. HPB (Oxford). 12(1): p. 73-9.
- Stokes, J.B., et al. Preoperative capecitabine and concurrent radiation for borderline resectable pancreatic cancer. Ann Surg Oncol . 18(3): p. 619-27.

