Keywords
erlotinib; gemcitabine; Pancreatic Neoplasms
Abbreviations
ECOG: Eastern Cooperative Oncology Group
INTRODUCTION
Treatment of advanced pancreatic cancer remains a challenge in medical oncology given its poor prognosis. In 1996, gemcitabine monotherapy was shown to give a modest improvement in overall survival compared to 5-fluorouracil (5-FU) bolus [1]. However, since then no significant advances have been made in the management of this disease.
Several clinical trials have been carried out using doublets of gemcitabine plus other antineoplastic agents (cisplatin, oxaliplatin, 5-FU, capecitabine and irinotecan) [2, 3, 4] as well as polychemotherapy regimens (cisplatin, gemcitabine, 5-FU, epirubicin, docetaxel) [5, 6] with the aim to improve survival results in patients with advanced pancreatic cancer. Although improvements in response rate and progression-free survival (PFS) were observed with some of the chemotherapy schemes tested, no improvements in overall survival have been yet observed. Studies combining gemcitabine with targeted therapies, such as bevacizumab and cetuximab, demonstrated good efficacy results in phase II trials. However, subsequent phase III trials demonstrated an improvement in progression-free survival but not in overall survival [7, 8, 9].
Epidermal growth factor receptor (EGFR) is one of potential molecular targets in pancreatic adenocarcinoma. When EGFR is activated by its specific ligand, it triggers an intracellular signalling pathway mediated by a tyrosine kinase which ultimately leads to cell migration, proliferation, invasion, angiogenesis and inhibition of apoptosis [10, 11]. EGFR is overexpressed in a high proportion of pancreatic cancer patients which is related to a poor prognosis [12].
Based on this knowledge, Moore et al. conducted in 2007 a randomized phase III trial comparing gemcitabine with gemcitabine plus erlotinib (an inhibitor of the EGFR tyrosine kinase domain) in the treatment of advanced pancreatic cancer. The phase III trial showed a statistically significant improvement in overall survival when gemcitabine was combined with erlotinib [13]. Since then, we adopted this form of therapy in our institution.
In the present study, we evaluated the efficacy and toxicity of the same schedule used by Moore et al. [13] as first-line treatment of unresectable, locally advanced or metastatic pancreatic cancer at our centre.
PATIENTS AND METHODS
We carried out a retrospective study of all consecutive patients with unresectable, locally advanced or metastatic pancreatic cancer who received first-line treatment with a combination of gemcitabine plus erlotinib between October 2007 and October 2010 in our centre. Gemcitabine (1,000 mg/m2) was administered weekly for up to 6 weeks followed by a week of rest and then once weekly for 3 consecutive weeks out of every 4 weeks. The dose of erlotinib was 100 mg per day throughout the treatment period.
ETHICS
According to Spanish legislation, observational studies conducted using entirely medical records files in which the personal identification data of the patients are kept separately from the clinical data (therefore anonymity is ensured) do not need written or oral informed consent. The study was approved by the Ethics Committee of Clinical Research of the Hospital La Fe (Valencia, Spain) and was conducted according to the Declaration of Helsinki for studies in humans.
STATISTICS
Summary statistics were calculated for continuous and categorical variables. Time-to-event data were described with the use of Kaplan-Meier methods. Univariate survival analysis and multivariate Cox regression analysis were carried out to identify independent predictors of overall survival. Data were analyzed by means of the SPSS 21 package (IBM, Armonk, NY, USA). A P value of less than 0.05 was considered statistically significant.
RESULTS
A total of 55 patients were included in the series. The baseline characteristics of these patients are displayed in Table 1. The median number of gemcitabine infusions was 9 (range: 1 to 63); 544 infusions were given in total in the whole population. Gemcitabine infusion was suspended in 218 instances (40.1% of the planned infusions). The most common cause of infusion suspension was afebrile neutropenia (n=196; 89.9%). However, dose reduction was only necessary in 3 patients (5.5%). No toxic deaths were reported. Toxicities led to gemcitabine discontinuation in 4 patients (7.3%). The median time of exposure to erlotinib was 8 weeks (range: 4 to 60 weeks).
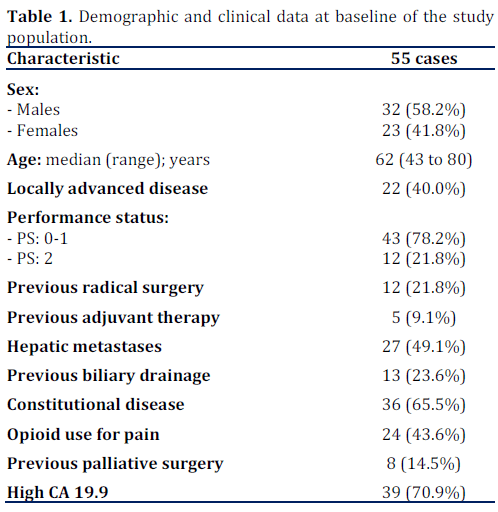
Table 2 describes the toxicity observed in the series. The combination of gemcitabine plus erlotinib was generally well tolerated with a low incidence of grade 3-4 adverse events. The most frequent adverse event was fatigue (37 cases, 67.3% of patients), grade 3 fatigue was observed in 8 patients (14.5%). Hematological toxicity was frequent: anemia in 29 patients (52.7%), thrombocytopenia in 17 patients (30.9%) and neutropenia in 15 patients (27.3%), although grade 3-4 toxicity was rare (n=6, 10.9%). No febrile neutropenia episodes were seen. Diarrhea was reported in 12 patients (21.8%), although only 2 patients (3.6%) had grade 3-4. It was also noteworthy the occurrence of up to 11 episodes of deep vein thrombosis (20.0%), 3 of which also had a pulmonary thromboembolism (5.5%).
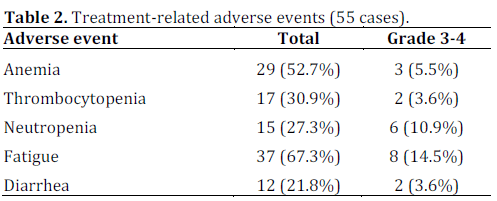
As for toxicity related to erlotinib, the most frequent adverse event observed in the series was acne-like rash (18 cases, 32.7% of patients). Most cases were of mild intensity, and severe cases (grade 3-4) were only reported in 2 patients (3.6%). Other adverse events related to erlotinib were mild hepatic toxicity, seen in one case (1.8%), and interstitiallike pneumonitis, seen in 3 patients (5.5%). Erlotinib was withdrawn in 10 patients (18.2%; including all cases reporting interstitial-like pneumonitis) due to tolerability issues, mainly fatigue.
Overall disease control rate (i.e., complete responses plus partial responses plus stable disease) was 47.3% (26 cases). Partial response was observed in 20.0% of patients (11 cases; according to Response Evaluation Criteria in Solid Tumors (RECIST) criteria) and in 21.8% of patients (12 cases) stable disease was reported. Disease progression was observed in 43.6% of the patients (24 cases). It is worth noting that the 5.5% (3/55) of cases in which a complete radiological response was achieved were treated for locally advanced forms of the disease.
Twenty patients in the series (36.4%) received a second-line of chemotherapy. The most widely used regimen was capecitabine plus oxaliplatin (used in 14 cases, 70.0% of patients receiving a second line). Other regimens used were the combination of 5-FU, leucovorin and oxaliplatin (FOLFOX), capecitabine and the combination of gemcitabine plus capecitabine. The median number of second-line chemotherapy cycles administered was 4 (range: 1 to 6). Overall disease control rate was remarkably lower with second-line treatment (20.0%, 4/20 cases). Partial response was reported in one case (5.0%) and stable disease in three cases (15.0%). Disease progression was reported in two thirds of patients (13 cases, 65.0%) receiving second-line treatment.
The median follow-up of the series was 21 months (range: 1 to 53 months). Median overall survival was 8.3 months (95% CI: 5.1 to 11.4 months). Oneyear survival was 34.2% and decreased to 9.7% after two years of follow-up (Figure 1).
Figure 1. Overall survival in the whole series.
The following variables were analyzed by univariate analysis as potential independent predictors of overall survival: age, sex, performance status (measured by the ECOG scale), locally advanced or metastatic disease, previous adjuvant treatment, presence of liver metastases versus no hepatic metastases, presence of systemic symptoms (constitutional syndrome), presence of pain, previous biliary drainage, presence of acne-like rash and the development of deep vein thrombosis. The results are shown in Table 3. Good performance status, locally advanced disease, the absence of hepatic metastases, and no previous biliary drainage were shown to be significant prognostic factors in the analysis. Univariate analysis also indicated that the development of acne-like rash during gemcitabine plus erlotinib treatment was related to a higher overall survival compared to patients that did not develop this adverse event. Median overall survival in patients who developed acne-like rash was 12.0 months compared to 5.2 months in patients who did not presented acne-like rash (P=0.025) (Figure 2). Moreover, univariate analyses indicated that patients who presented deep vein thrombosis had a significantly lower overall survival. Thus, median overall survival in patients who presented deep vein thrombosis was 4.7 months compared to 9.9 months in patients who did not develop this adverse event (P=0.013).
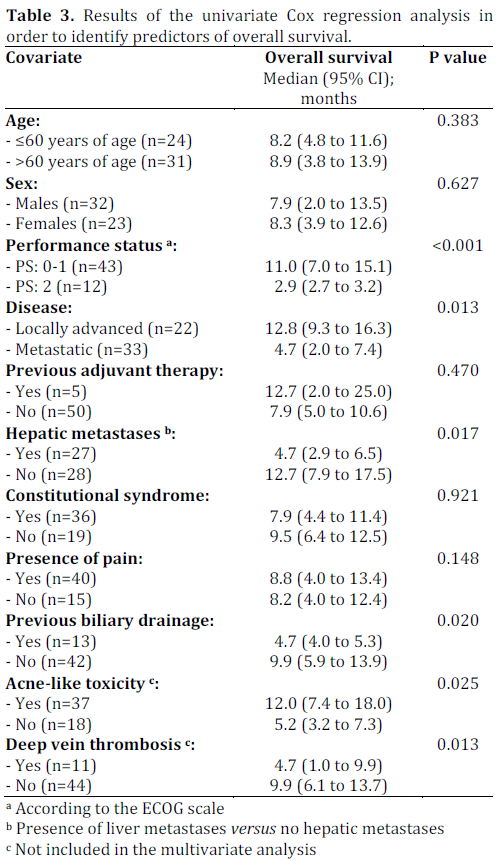
Figure 2. Overall survival according to the development of acne-like
rash during the treatment with gemcitabine plus erlotinib.
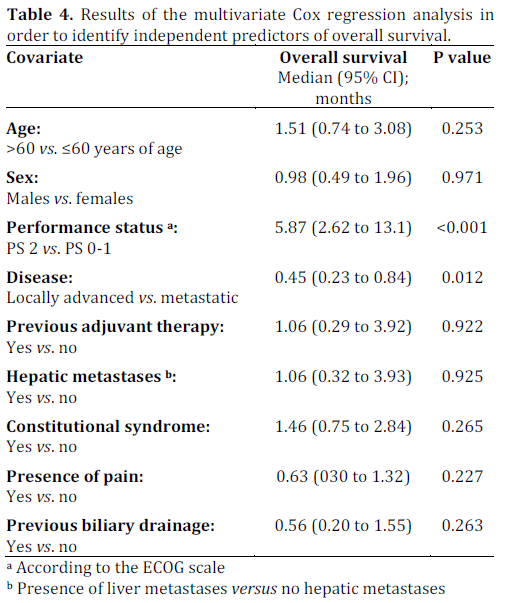
All the previous factors were included in the multivariate Cox regression analysis, except the acne-like rash and the development of deep vein thrombosis as we decided to only include prognostic factors that were present before the treatment with gemcitabine-erlotinib. Results are shown in Table 4. Only two of the nine variables analysed were statistically significant in the multivariate analysis and, therefore, could be considered as independent predictors of overall survival. These two variables were a good performance status (PS 0 or 1) and locally advanced disease.
DISCUSSION
The understanding of the molecular mechanisms that trigger and regulates tumor growth is leading to more appropriate therapeutic approaches for cancer patients with improved results and lower toxicities.
Several signalling pathways are activated in pancreatic adenocarcinoma that promotes cell proliferation and apoptosis inhibition. One of the best understood pathways activated in pancreatic adenocarcinoma is that involving EGFR 1. That receptor is activated by specific ligands triggering an intracellular signalling pathway mediated by Ras which in turn leads to activation of the Raf/MEK/ERK and PI3K/Akt/mTOR pathways. Activation of these pathways leads to cell migration, proliferation, invasion, angiogenesis and inhibition of apoptosis [14]. EGFR is overexpressed in the majority of pancreatic adenocarcinomas which is associated with a poor prognosis [15]. Ras is a protein that plays a key role in the intracellular signalling cascade triggered by EGFR. Most pancreatic adenocarcinomas have a Ras mutation in codon 12 of KRAS. Point mutations in KRAS have been suggested as early events in the development of ductal adenocarcinoma [16]. These mutations result in a constitutive activation of the signalling cascade mediated by Ras. Moreover, the activation of the PI3K/Akt/mTOR pathway, also mediated by Ras, has been detected in approximately half of pancreatic adenocarcinomas and has been associated with a worse prognosis [17]. Poor prognosis related to such activation is partially explained by the fact that it is also considered as a potential mechanism of gemcitabine resistance. PTEN is a tumor suppressor gene that inhibits the PI3K/Akt/mTOR pathway. Mutations in PTEN lead to a loss of cellular control over this pathway [18].
Another pathway involved in pancreatic adenocarcinoma is that of the vascular-endothelial growth factor (VEGF) ligand, which acts on two tyrosine-kinase receptors VEGF-1 and VEGF-2. Activation of these receptors leads to increased cell growth and angiogenesis [19]. In addition, elevated serum levels of VEGF have been associated with a decreased survival [20]. All these intracellular signalling pathways represent potential targets for new drugs such as erlotinib, an inhibitor of the tyrosine kinase domain of EGFR.
As mentioned previously, the gemcitabine plus erlotinib regimen, which was analyzed in our series, is based on that used in the Moore et al. trial conducted in 2007 comparing gemcitabine alone to gemcitabine plus erlotinib [13]. The primary endpoint of the Moore et al. trial was overall survival. A total of 569 patients with locally advanced unresectable or metastatic pancreatic cancer were randomized to two arms: gemcitabine plus erlotinib versus gemcitabine plus placebo. Overall survival was significantly higher in the gemcitabine plus erlotinib arm with a hazard ratio (HR) of 0.82 (95% CI: 0.69 to 0.99; P=0.038) and a median survival of 6.24 months versus 5.91 months. One-year survival was also higher in the gemcitabine plus erlotinib arm (23% versus 17%, P=0.023). Progression-free survival was significantly higher with the doublet therapy with a HR of 0.77 (95% CI: 0.64 to 0.92; P=0.004). No differences in the objective response rate were observed between the two arms. However, there was a higher rate of disease stabilization in the gemcitabine plus erlotinib arm. Toxicity was higher with the doublet chemotherapy, especially skin toxicity, but in most cases this was of mild intensity (grade 1-2). The authors concluded that the optimal dose of erlotinib in combination with gemcitabine should be 100 mg/day.
There were some remarkable differences in the baseline characteristics of the patients included in our retrospective series and the population enrolled in the Moore et al. clinical trial. Thus, in our retrospective series there were a higher proportion of patients with locally advanced disease (40% vs. 23%). This might partly explain the higher response rate obtained in our study (25% vs. 9%). It is also noteworthy that reported episodes of interstitiallike pneumonitis observed in our study were more than double that seen in the Moore et al. trial (5.5% vs. 2.4%). These findings are difficult to be explained.
This higher rate of interstitial-like pneumonitis of our study could be due to a much smaller number of patients. Finally, overall survival observed in our study was longer than in the Moore et al. clinical trial. The high proportion of patients with locally advanced disease (which is related to a higher survival than metastatic disease) might explain the greater survival and the higher response rate observed in our study.
In our study, multivariate Cox regression analysis indicated that poor performance status is the most important prognostic factor of overall survival. In addition, locally advanced forms of disease were related to better prognosis. Therefore, there are some patients (with good performance status and no metastatic staging at diagnosis) who could benefit more from a gemcitabine plus erlotinib regimen as first line of treatment of advanced pancreatic cancer.
The univariate analysis of prognostic factors indicated a statistically significant association between the occurrence of venous thrombosis or acne-like rash during treatment with overall survival. Patients in the series that develop venous thrombosis have a worse survival compared to those who did not presented this adverse event. Moreover, patients who developed acne-like rash toxicity that is related to erlotinib administration, presented a prolonged survival. Other authors have confirmed this finding [21].
As noted earlier, the activity of second-line chemotherapy in the series is reduced. Regimens used in our centre were mainly based on fluoropyrimidines in monotherapy or associated with oxaliplatin. Those patients with good performance status (PS 0-1) potentially benefit more from second-line chemotherapy. Thus, it could be advisable to offer this therapeutic option in this group of patients. However, symptomatic treatment should be reserved for patients with poor performance status (PS 2 or higher) due to the small benefit obtained with second-line regimens.
Recently, a phase III trial has been published with the combination of 5-FU, irinotecan and oxaliplatin (FOLFIRINOX). This trial indicated that patients with metastatic disease at diagnosis who received this chemotherapy regimen presented a greater survival compared to those patients who received gemcitabine [22]. The results of this trial could lead to a change in the first line treatment of advanced pancreatic cancer. However, since most of the patients included in the trial had a very good performance status and no previous biliary drainage, patients who could benefit from this chemotherapy should be carefully selected.
Our results indicated that gemcitabine plus erlotinib doublet is active in our series of patients with advanced pancreatic cancer. This study provides efficacy and safety data similar to those of the pivotal phase III clinical trial that tested the same combination [13]. Similar results have been reported by other groups [21].
Financial disclosure
Financial support for this research was provided by Roche (Basel, Switzerland)
Conflict of interest statement
There are no conflicts of interest
References
- Burris HA, Moore MJ, Andersen J Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as first line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997; 15:2403- 13.
- Poplin E, Feng Y, Berlin J, Rothenberg ML, Hochster H, Mitchell E, et al. Phase III randomized study of gemcitabine and oxaliplatin versus gemcitabine (fixed-dose-rate-infusion) compared with gemcitabine (30-min infusion) in patients with pancreatic carcinoma. E6201: a trial of ECOG. J Clin Oncol 2009; 27:3778-85.
- Herrmann R, Bodoky G, Ruhstaller T, Glimelius B, Bajetta E, Schüller J, et al; Swiss Group for Clinical Cancer Research; Central European Cooperative Oncology Group. Gemcitabine plus capecitabine compared with gemcitabine alone in advanced pancreatic cancer: a randomized, multicenter, phase III trial of the Swiss Group for Clinical Cancer Research and the Central ECOG. J Clin Oncol 2007; 25:2212-7.
- Colucci G, Giuliani F, Gebbia V, Biglietto M, Rabitti P, Uomo G, et al. Gemcitabine alone or with cisplatin for the treatment of patients with locally advanced and/or metastatic pancreatic carcinoma: a prospective, randomized, phase III study of the Gruppo Oncologia dell’Italia Meridionale. Cancer 2002; 94:902-5.
- Fine RL, Fogelman DR, Schreibman SR, Desai M, Sherman W, Strauss J, et al. The gemcitabine, docetaxel and capecitabine (GTX) regimen for metastatic pancreatic cancer: a retrospective analysis. Cancer Chemother Pharmacol 2008; 61:167-75.
- Reni M, Cordio S, Milandri C, Passoni P, Bonetto E, Oliani C, et al. Gemcitabine versus cisplatin, epirubicin, fluorouracil and gemcitabine in advanced pancreatic cancer: a randomized controlled multicentre phase III trial. Lancet Oncol 2005; 6:369-76.
- Kindler HL, Friberg G, Singh DA, Locker G, Nattam S, Kozloff M, et al. Phase II trial of bevacizumab plus gemcitabine in patients with advanced pancreatic cancer. J Clin Oncol 2005; 23:8033-40.
- Xiong HQ, Rosenberg A, LoBuglio A Schmidt W, Wolff RA, Deutsch J, et al. Cetuximab, a monoclonal antibody targeting the epidermal growth factor receptor, in combination with gemcitabine for advanced pancreatic cancer: a multicenter phase II Trial. J Clin Oncol 2004; 22:2610-6.
- Kindler HL, Niedzwiecki D, Hollis D, Oraefo E, Schrag D, Hurwitz H, et al. A double-blind placebo-controlled, randomized phase III trial of gemcitabine (G) plus bevacizumab (B) versus gemcitabine plus placebo (P) in patients (pts) with advanced pancreatic cancer (PC): A preliminary analysis of Cancer and Leukemia Group B (CALGB) 80303. Presented at: 2007 ASCO Gastrointestinal Cancers Symposium; January 17-21, 2007; Orlando, Florida. Abstract 108.
- Lemoine NR, Hughes CM, Barton CM, Poulsom R, Jeffery RE, Klöppel G, et al. The epidermal growth factor receptor in human pancreatic cancer. J Pathol 1992;166:7-12.
- Tzeng CW, Frolov A, Frolova N, Jhala NC, Howard JH, Vickers SM, et al. EGFR genomic gain and aberrant pathway signaling in pancreatic cancer patients. J Surg Res 2007; 143:20-6.
- Fujita H, Ohuchida K, Mizumoto K, Itaba S, Ito T, Nakata K, et al. High EGFR mRNA expression is a prognostic factor for reduced survival in pancreatic cancer after gemcitabine-based adjuvant chemotherapy. Int J Oncol 2011; 38:629-41.
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al.; National Cancer Institute of Canada Clinical Trials Group. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 2007; 25:1960-6.
- Xiong HQ. Molecular targeting therapy for pancreatic cancer. Cancer Chemother Pharmacol 2004; 54:S69-77.
- Ueda S, Ogata S, Tsuda H, Kawarabayashi N, Kimura M, Sugiura Y, et al. The correlation between cytoplasmic overexpression of epidermal growth factor receptor and tumor aggressiveness: poor prognosis in patients with pancreatic ductal adenocarcinoma. Pancreas 2004; 29:1-8.
- Furukawa T. Molecular pathology of pancreatic cancer: implications for molecular targeting therapy. Clin Gastroenterol Hepatol 2009; 7:35-9.
- Schlieman MG, Fahy BN, Ramsamooj R, Beckett L, Bold RJ. Incidence, mechanism and prognostic value of activated AKT in pancreas cancer. Br J Cancer 2003; 89:2110-5.
- Asano T, Yao Y, Zhu J, Li D, Abbruzzese JL, Reddy SA. The PI-3-kinase/Akt signaling pathway is activated due to aberrant PTEN expression and targets transcription factors NF-kB and c-myc in pancreatic cancer cells. Oncogene 2004; 23:8571-80.
- Korc M. Pathways for aberrant angiogenesis in pancreatic cancer. Mol Cancer 2003; 2:8.
- Karayiannakis AJ, Bolanaki H, Syrigos KN, Asimakopoulos B, Polychronidis A, Anagnostoulis S, et al. Serum vascular endothelial growth factor levels in pancreatic cancer patients correlate with advanced and metastatic disease and poor prognosis. Cancer Lett 2003; 194:119-24.
- Aranda E, Manzano JL, Rivera F, Galán M, Valladares-Ayerbes M, Pericay C, et al. Phase II open-label study of erlotinib in combination with gemcitabine in unresectable and/or metastatic adenocarcinoma of the pancreas: relationship between skin rash and survival (Pantar study). Ann Oncol 2012; 23:1919-25.
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al.; Groupe Tumeurs Digestives of Unicancer; PRODIGE Intergroup. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364:1817-25.



