Key words
end of life, family carers, hospice,Ma¯ori,
New Zealand, palliative care
Introduction
Ma¯ori are indigenous to Aotearoa/New Zealand, and
comprise approximately 15% of the country’s 4.4
million inhabitants (Statistics New Zealand, 2011).
Disparities between Ma¯ori and non-Ma¯ori in morbidity,
mortality and the quality of healthcare services
received are well documented (for example, see Robson
and Harris, 2007). Ma¯ori are less likely to access healthcare
services in general, despite having higher levels of
need (Robson and Harris, 2007). Findings from a
three-year chart review (n = 1293) conducted at a
hospice based in Wellington, the capital city, showed
that between 2006 and 2008 only 6% of patients selfidentified
as Ma¯ori, even though Ma¯ori represent 10%
of the population of this region (Capital Coast District
Health Board, undated). Although this chart review
indicated that the length of time during which individuals
received hospice services and the number of
inpatient unit visits did not differ significantly by
ethnicity, it was found that Ma¯ori patients were
significantly younger and were more likely to die at
home than non- Ma¯ori patients (Taylor et al, 2012).
Many Ma¯ori people express beliefs and practices
with regard to what constitutes health and with regard
to the processes of death and dying which appear quite
distinct from those from other cultural backgrounds
(Cram et al, 2003; Walker et al, 2008; Waldon, 2003).
Specific traditional rituals at the time of death and
bereavement are as unique as those from any culture.
Indeed, they can vary slightly from one Ma¯ori tribe to
another. Traditionally, for example,manyMa¯ori believe
that it is spiritually important to die and be buried at
one’s ancestral home. Bodies are typically returned to
this location if the deceased did not die there. Extended
family and friends gather for 3 to 5 days to
mourn the deceased at the local meeting house. Those
who mourn talk, and even joke or sing, to the deceased
to bring closure to their relationship. Mourners may
sleep in the large meeting house where the deceased
person is lying. At the end of the mourning period, the
deceased person is buried (Schwass, 2005).
Hospices in Aotearoa/New Zealand are striving to
respond to the New Zealand Palliative Care Strategy
(Ministry of Health, 2001) that advocates culturally
sensitive palliative care for all. A recent qualitative study
of Auckland area indigenous and immigrant clinician,
patient, and family perspectives on challenges to hospice
services described several barriers to accessing
hospice care among Asian, Pacific andMa¯ori people in
northern Aotearoa/New Zealand (Frey et al, 2013).
These barriers included unfamiliarity with what hospice
care involves, perceptions of hospices as a place in which to die that costs a lot of money, language
barriers, gatekeeping physicians who assumed that
members of these groups would prefer not to use
hospice services, and fear of discrimination from the
predominantly white hospice clinicians (Frey et al,
2013).
These issues relating to end-of-life care are not
unlike those found among other indigenous peoples,
for example, in Australia, Canada, and the USA. All of
these have been described as often having in common
the following factors that affect end-of-life care (see,
for example, O’Brien et al, 2013; Johnston et al, 2013;
McGrath and Phillips, 2009; Kelly et al, 2009; Hotson
et al, 2004):
• remote homes, resulting in social isolation when
the patient is taken to an urban-based palliative
care service
• beliefs and customs, such as spiritual connection
with the land of one’s heritage, prompting the
desire to die at home
• low economic status and distrust of western medical
care contributing to delayed entry into a
westernised healthcare system
• respect for traditional and spiritual healers and
healing modalities
• the vital importance and involvement of an often
large, extended family
• deference to elders in the community who can
provide knowledge pertinent to end-of-life care
• holistic philosophies about how to live and die,
which include a spiritual component.
Given the known health and healthcare disparities
between Ma¯ori and non-Ma¯ori in Aotearoa/New
Zealand, and the trend among indigenous peoples of
the South Pacific and North America, it is plausible
thatMa¯ori may not receive the same quality of end-oflife
hospice care as non-Ma¯ori patients do. However,
Ma¯ori have the right to high-quality, appropriate care
in all health settings (United Nations, 2007).
With the exception of the study by Frey et al (2013)
which recruited only six Ma¯ori patient or family carer
participants, there is a paucity of documentation about
Ma¯ori perceptions and experiences of receiving endof-
life care from a hospice. A search of six databases
(including CINAHL, PubMed and PsycINFO) revealed
no other report of Ma¯ori patient or family perspectives.
Therefore the purpose of this pilot study was to
address the following questions. How do Ma¯ori perceive
hospice care? What cultural practices would be
desired if they were receiving care at a hospice? What
aspects of hospice support are appreciated? What are
the barriers to entering hospice services? What could
hospices do to improve care for Ma¯ori patients?
Cultural and philosophical
underpinnings
Hospices provide palliative care for those with a lifelimiting
illness. Palliative care aims to ease suffering
and maintain quality of life by addressing physical,
psychosocial, cultural and spiritual symptoms and
needs (Palliative Care Subcommittee, New Zealand
Cancer Treatment Working Party, 2007). In Ma¯ori
society this care is usually delivered by a multidisciplinary
team, and places patient and familywha¯nau at
the centre of care. The Ma¯ori te whare tapa wha¯ model
of hauora (health) is based on four pillars: wairua
(spiritual well-being), hinengaro (emotional and mental
health), tinana (physical well-being) and wha¯nau (family, including extended family, and the wider
social system) (Durie, 1985; Ministry of Health, 2012).
According to this model, hauora is supported not only
by disease prevention and cure but also by health
promotion that recognises and builds upon existing
assets, such as wha¯nau support.
Both palliative care and theMa¯ori te whare tapa wha¯
model emphasise holistic caring and value the role of
wha¯nau. However, this study aimed to determine
more precisely which aspects of palliative hospice
care are appreciated by Ma¯ori people, and what other
aspects could be improved to ensure that Ma¯ori
patients receive appropriate care.
For an explanation of the te reo Ma¯ori terms that are
used in this paper, see Table 1.
Table 1 :Explanation of te reo Maori terminology
Methodology
Project design
This pilot study was shaped by the Kaupapa Ma¯ori
research paradigm. The Treaty of Waitangi, the founding
document of Aotearoa/New Zealand, sets out the
principles of partnership, self-determination, equity,
and protection for Ma¯ori (www.nzaot.com/downloads/
contribute/TheTreatyofWaitangiAFrameworkfor
MaoriHealth.pdf). Kaupapa Ma¯ori applies these principles
in a research setting for the benefit of Ma¯ori
people, particularly the community in which the
research takes place. KaupapaMa¯ori is oriented towards
restoring justice, reclaiming resources and recovering
histories (Smith, 1999). The Health Research Council of
New Zealand mandates that any research involving
Ma¯ori people must involve consultation with Ma¯ori
and, in particular, Ma¯ori in the community in which
the research will have an impact (Health Research
Council of New Zealand, 2008). Thus Kaupapa Ma¯ori
research is characterised as research byMa¯ori, forMa¯ori
and with Ma¯ori (Health Research Council of New
Zealand, 2008). Although the principal investigator of
this pilot study (EJT) did not identify as Ma¯ori, the coinvestigators
included a university-based health researcher
(SS), the Chief Executive of a hospice (RE),
and a Ma¯ori Liaison from the same hospice (PT), all of
whom identified as Ma¯ori. This project was initiated by
the Ma¯ori chief executive, who requested the hospice’s
non-Ma¯oriResearchDirector to direct it. Te PouTautoko
(meaning the central post supporting a meeting house),
the hospice’s Ma¯ori advisory group, was consulted
throughout the design and implementation of the study.
This group provided affirmation for the design, suggestions
about how to collect data, and recommendations
about who to interview. The Ma¯ori researchers led and
guided all communication and consultation with the
Ma¯ori study participants and Ma¯ori community. They
also ensured that appropriate protocol was adhered to at
meetings and interviews.
The hospice
This study was conducted at Mary Potter Hospice
(MPH), a charitable trust that serves the Wellington
region of Aotearoa/New Zealand. This hospice offers
free multidisciplinary palliative care, primarily in the
home but also in day units and an 18-bed inpatient
unit. Although there was a sense among the MPH staff
that Ma¯ori hospice use was increasing, no empirical
data to substantiate this observation existed.
Participants and recruitment
Participants were recruited in 2010 from two groups,
namely whanau and kauma¯tua.
Wha¯nau
Wha¯nau are family members of Ma¯ori patients who
had utilised the hospice service and who had died
during the 6- to 18-month period prior to the study.
Once they had been identified (by a computer search
of hospice patient records), individuals were sent a
letter of invitation and then contacted by telephone by
the Ma¯ori Liaison to discuss participation. Face-toface
or personal contact is preferable in Kaupapa
Ma¯ori research (Smith, 1999). Given the salient role
of wha¯nau support, the researchers chose to allow
multiple members of one wha¯nau to participate.
Opening the invitation to the wider wha¯nau was
considered congruent with Ma¯ori culture.
Kauma¯ tua
Kauma¯tua were invited to take part in interviews.
Kauma¯tua are male or female elders who are selected
by their community for their knowledge of Ma¯ori
customs and their ability to instill this knowledge in
the younger generations (Barlow, 1994). Kauma¯tua may
be called upon to settle disputes or to represent the
community to those outside it.These elders arehonoured
and shown considerable respect. The kauma¯tua, who
were identified by the Ma¯ori advisory group or Ma¯ori
Liaison, were approached by either the Chief Executive
or the Ma¯ori Liaison. Kauma¯tua were selected not
only because they could provide wisdom informed by
a deep knowledge of Ma¯ori culture, but also because
they could represent their communities at large.
Kauma¯tua from diverse iwi (tribes) were selected.
Although this was not planned, all five of them had
had relatives who had received hospice care.
Ethics
The Central Regional Health and Disability Ethics
Committee granted approval for the study. All of the
participants (focus group members and kauma¯tua)
gave their written consent after receiving information
about the study. The consent document advised
participants that if their participation caused distress,
the hospice’s spiritual carers and counsellors would be
available to them.
Methods
Research based on Kaupapa Ma¯ori tends to favour
qualitative methods, as these are based on social
interaction. Two methods were selected:
1 Wha¯nau participants were invited to take part in
one of two focus groups, both of which took place
in a Ma¯ori health clinic adjacent to a meeting hall
(marae). These focus groups were conducted in
accordance with accepted practice, with limited
group size, a pre-set structure for questions and
the meeting, guided by a trained facilitator, with a
secondary researcher in a supportive role (Ruff et al,
2005).
2 Kauma¯tua were interviewed privately in their
homes.
Both the focus groups and interviews followed Ma¯ori
protocol relating to mihi (introductions), and were led
by the Ma¯ori researcher, with the non-Ma¯ori principal
investigator taking a secondary role. The Ma¯ori language,
te reo, was encouraged if participants chose to
speak it. Each participant used a number of Ma¯ori
words and idioms, and one elder chose to conduct
most of the interview in te reo Ma¯ori. (Translation of
the occasional word or phrase was done by a Ma¯ori
member of the research team after the transcription.
The interview in te reo was transcribed by the Ma¯ori
research team member who had conducted the interview,
and was then translated by a professional language
translation service.) Following each focus group,
wha¯nau participants were acknowledged with kai
(food), which is central to Ma¯ori gatherings, and
kauma¯tua were thanked with a gift voucher for
NZ$30.
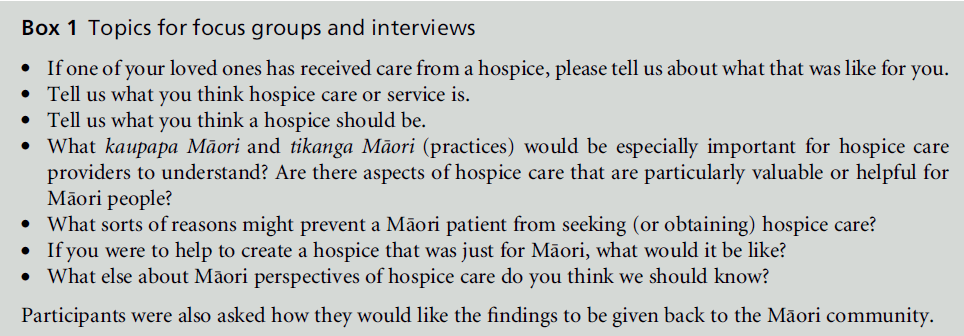
The focus groups and interviews ranged from 1 to 2
hours in length and addressed the same topics (see Box
1). If the participants agreed, interviews and focus
groups were audio-recorded. One kauma¯tua requested
that his voice should not be recorded, but agreed that
notes could be taken. The recorded focus groups and
interviews were all transcribed by either a professional
service or a hospice employee.
Various strategies were used to ensure the trustworthiness
of the findings (Lincoln and Guba, 1985).
These included prolonged in-depth engagement with
participants for at least 1 hour, creating an audit trail (audio recordings or notes of data collected and documentation
about the analysis process), peer debriefing
with project team members during regular meetings,
and obtaining validation for the findings from a nonresearch
team member who was an expert in Ma¯ori
perspectives on hospice care.
Analysis
An inductive thematic analysis (Patton, 2002) was
completed by the two researchers who conducted the
interviews. This analysis involved extracting from the
transcriptions the data that were relevant to the study
questions. These data were then condensed into themes,
keeping with them pertinent illustrative data. The
themes were clustered mostly around how hospice
care was perceived, what was appreciated or desired at
a hospice, possible barriers to using hospice services,
and miscellaneous observations about how the Ma¯ori
participants related to death and dying. Although the
findings were written by the non-Ma¯ori project team
leader (EJT), they were reflective of separate analyses
performed by both herself and theMa¯ori co-researcher
(SS). During this final stage of the analysis, these
researchers discussed their respective perspectives on
the data to ensure reliability and cultural sensitivity;
this discussion revealed only minor discrepancies.
Findings
A total of 35 wha¯nau were identified as eligible to take
part in the study. However, when the Ma¯ori Liaison
attempted to contact them it was found that either
they were either no longer contactable by the telephone
number listed in the deceased patient’s chart,
they were not Ma¯ori themselves, they did not have
transport, they did not have a family member to
accompany them, they were afraid to participate, or
they declined to participate for an unstated reason.
The Ma¯ori Liaison perceived that this was evidence of a fear of talking about death. Finally, seven wha¯nau
(one man and six women, aged 34–74 years) agreed to
take part in the focus groups. They were the husband,
daughter, mother and wives of the deceased persons.
Each individual brought a relative who also participated,
sharing their own stories of living with a loved
one who had received hospice care. These whanau,
who represented the experiences of three hospice
patients, all became study participants (n = 7). Five
kauma¯tua (four women and one man, aged 62–79
years) were approached, all of whom granted interviews.
They were the spouses or parents of the deceased
persons.
Theme 1: How do Ma¯ ori people
perceive hospice care?
Although some of the participants described receiving
a hospice nurse’s care for their loved one at home, they
all equated hospice care with the inpatient unit (IPU).
A few referred to it as being like a hospital, a place
where ‘they have their rules ... [and] they are in
charge’, and consequently ‘you don’t have the freedom
you do at home ... you are a guest there ... it isn’t
your space’ (kauma¯tua participant). Several participants
were aware of the hospice as a place of care for
those with cancer and also for elderly people, inferring
that younger people or those with terminal nonmalignant
diseases may receive care elsewhere.
The hospice was most frequently perceived as a
place that ‘you don’t leave alive.’ It is where one dies:
‘the last ride out’, ‘the end, doom and gloom!’
(kauma¯tua participant and wha¯nau participant, respectively).
The participants stated that most Ma¯ori
people whom they knew shared this perception. However,
they added that their personal experiences did
not support this perception, and that they now recognised
the hospice as a place for respite care and
symptom management. A wha¯nau participant described
how she came to realise that hospice care for
her loved one meant that ‘it wasn’t just the end ... there
was more that could be done.’ One kauma¯tua participant
went further than this, stating that hospice care
could prolong life ‘at least a few days as its eases pain
and suffering.’ This elder posited that wha¯nau who do
not take their suffering, dying loved one to a hospice
‘are selfish to themselves and not caring about the
sick.’
What aspects of hospice care do
Ma¯ ori appreciate?
The participants’ views provide insights into what
Ma¯ori people value. Those who had witnessed respite
care for a loved one found it an extremely positive
experience: ‘for my children and family if I’m at Mary Potter, leave me there. [Be]cause I do know the strain
on the family’ (wha¯nau participant). Others perceived
benefits of hospice care included the quietness in
the IPU, which allowed the ‘spirit to settle’ (wha¯nau
participant), patient care equipment for use at home,
information about how to care for the patient and
what was happening, counselling and ‘someone to talk
to’ (wha¯nau participant), follow-up bereavement care,
the presence of spiritual carers (clergy) and the availability
of a chapel, a non-denominational memorial
service, and the availability of and feeling comfortable
with asking staff for help. One kauma¯tua participant
described a visit to support someone at their death
with karakia (prayer), and experienced the nurses as
culturally ignorant and disrespectful. However, all of
the other participants enthused about the compassion
that they experienced from hospice staff. For at least
one individual, the hospice IPU could create a comforting
sense of community: ‘There is a sense of
everybody knowing ... it’s like we’re all wha¯nau even
though you are all strangers. ... I was able to go there,
not just to be with [my husband], but with the people
that are around, that are just sitting there, just to be
part of ... if they wanted ... have a talk ... I like it in there’
(kauma¯tua participant).
What aspects of Ma¯ ori culture are
desired in hospice care?
Wha¯nau-centred care was of vital importance to the
participants. They appreciated being allowed to visit
and stay at any time, being ‘free to come and go’
(wha¯nau participant). Wha¯nau carers wanted staff
support so that they could continue to provide care
such as bathing, and wished that staff would ask their
permission to provide care for their loved one.
Wha¯nau also emphasised the importance of letting
their loved ones spend their final days at home. Elders
in particular preferred to die at home. The reasons for
wanting to go home for the final days of life were
varied, and included the following: ‘Ma¯ori take care of
their own ... it’s better, more flexible, they prefer their
own space’ (kauma¯tua participant); ‘[my mum] didn’t
want to die in somebody else’s bed’ (wha¯nau participant);
‘their own home is their roots, it’s everything—
tu¯rangawaewae [a place where one has the right to
observe one’s own protocols for behaviour, and freedom
to express one’s emotions and opinions; this
place is linked to kinship and genealogy]’ (wha¯nau
participant). The importance attached to dying at
home could create internal conflict when the wha¯nau
carers became exhausted. The hospice’s respite service
was welcomed both as an option when this occurred,
and for those patients who did not have local wha¯nau
support: ‘It takes people in to give the family a break’
(kauma¯tua participant).
What caring practices do Ma¯ ori
people use?
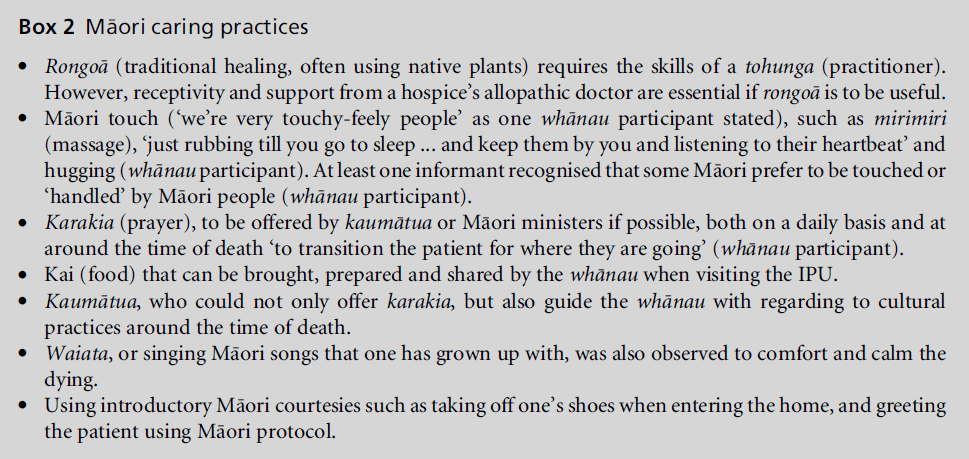
The participants identified a range of tikanga Ma¯ori
(cultural practices) (see Box 2). Speaking te reo Ma¯ori
(Ma¯ori language) to those who spoke te reo ‘got
through’ and ‘settled’ them (wha¯nau participant). Te
reo ‘language is important ... it’s much nicer and much
softer in your own language’ (kauma¯tua participant).
This same participant recommended that nurses learn
some te reo, especially greetings and farewells, and the
everyday terms such as the words for eating, toileting
and bathing.
Other tikanga reflected Ma¯ori beliefs about people,
places and conditions being either tapu (sacred or
restricted) or noa (unrestricted or ordinary). For example,
when a person died, the room and the body of
the deceased became tapu. Sprinkling water provided
spiritual cleansing, and karakia [prayer] was used to
mark the transition of the person from one state to the
other. When visitors arrived to view the deceased
person, they washed their hands when entering and
leaving the room. Karakia and sprinkling of water in
the hospice room after the deceased person had been
removed was regarded as essential before that room
could be used again. Other examples concerned the
use of linen, care of personal valuables, disposal of
body tissue, and types of food and drink. One family
was displeased with the lack of privacy afforded them
when they accompanied their deceased loved one
from the IPU room to the undertaker’s room, which
is regarded as a very sacred moment.
Several kauma¯tua recognised the requisite of institutional
support of tikanga Ma¯ori practices if they
were to occur. Policies supporting tikanga Ma¯ori, staff
cultural training, and the employment of Ma¯ori staff
who are respected and in leadership positions were seen as contributing to positive hospice experiences
for Ma¯ori people. The lack of staff knowledge was
evident in one poignant negative experience: ‘We did
our karakia [in this case sung] and we were strong, but
the nurses were just a nuisance with their applauding
and wandering around. They didn’t realise that tikanga
Ma¯ori was taking place’ (kauma¯tua participant).
What are the barriers to accessing or
receiving hospice care?
Many of the problems that the participants encountered
with hospice care were also considered to be
reasons that discouragedMa¯ori people from accessing
hospice services. The most frequent and salient response
to queries about these barriers was the perception
of hospice care as the ‘end of the line’ (wha¯nau
participant). One kauma¯tua participant believed that
the denial of death prevented people from learning
about and using hospice care. The other major reason
thought to prevent Ma¯ori people from using hospice
care was the cultural imperative around ‘caring for
our own’ (wha¯nau participant). There is a perception
among many Ma¯ori that ‘there are no options given to
wha¯nau who want to look after their own’ (kauma¯tua
participant). Elders in particular do not want to leave
their own space, and the grandchildren they may have
raised, in order to enter an institution likened to a
hospital. The struggle to care for one’s own was
sometimes intensified by this imperative. Those who
accepted respite care in the IPU for their loved one
recognised that they ‘just couldn’t do any more’, and
stated that receiving respite care at the hospice was ‘a
release’ (wha¯nau participant).
Other problems or barriers to receiving hospice care
included difficulties with transportation and parking, and wishing that the hospice was closer to the pa¯
(Ma¯ori settlement), particularly if one was ‘the only
brown face’ (kauma¯tua participant), as the presence of
other Ma¯ori people allowed one to feel more comfortable
and understood. Medical jargon and the lack of
open communication were not helpful: ‘I got really
annoyed about [the staff] giving people false hope
when the truth is they’re going to die’ (wha¯nau participant).
An additional issue was the lack of privacy:
‘We went in there and there were two or three
[patients] in the room. ... Here we were going to
look at my nephew, to weep for him, and to say ‘The
time has come for you to leave, but your path is clear
before you.’ How could we weep? How could we show
our grief in that room when others were there?’
(kauma¯tua participant).
These factors led participants to offer the following
specific suggestions about how to counteract these
challenges:
• offering better support for tikanga, such as providing
a place for kauma¯tua to carry out cultural
practices, and training staff about tikanga
• offering better support for whanau, such as providing
facilities for kai preparation, childcare for
visiting young children, a laundry service, encouraging
the family to appoint a spokesperson to
interface on their behalf with clinicians, and addressing
transportation and parking limitations
• improving the environment, moving closer to the
pa¯, and making the hospice more like a marae
[Ma¯ori meeting house]
• counteracting misperceptions of hospice care by
providing information seminars within the Ma¯ori
community and advertisements about hospice
care, encouraging Ma¯ori patients and wha¯nau to
share their positive stories of receiving hospice
care, and changing the term ‘hospice.’
These suggestions were offered in the hope that other
Ma¯ori people would similarly come to benefit from
hospice care.
The participants all recognised that their culture
was changing in terms of how it perceived end-of-life
care should be. It was acknowledged that some individuals,
especially older people, were more observant
of tikangaMa¯ori, while others were less aware of their
culture’s beliefs and practices with regard to end-oflife
care. For example, some might want rongoa¯,
mirimiri or karakia, while others might not.
Discussion
This small study presents the perceptions held by some
Ma¯ori wha¯nau about hospice care. The findings demonstrate
how the holistic Ma¯ori framework for well being is compatible with the perceptions of and
preferences for end-of-life care for Ma¯ori patients
and wha¯nau (Ministry of Health, 2012). The physical
and mental health of the individual, their spiritual
well-being and spiritual realities were all of concern to
Ma¯ori people. Central to the quest for hauora is
wha¯nau ora, family well-being, and support for and
by members of the wider family. Encompassing these
perspectives is tikanga Ma¯ori (Ma¯ori cultural practices).
Indeed, these findings demonstrate how many
practices, such as te reoMa¯ori, mihi, waiata and uses of
kai, continue to be highly valued in the culture and are
therefore vital to culturally sensitive care at the end of
life (Barlow, 1994).
All of the participants identified various barriers
that could prevent Ma¯ori people from using hospice
services, and these were similar to the findings of Frey
et al (2013) and Bray and Goodyear-Smith (2013).
However, positive personal encounters with the hospice
changed their perceptions. Patients could enter
and leave the IPU, which meant that more could be
done to help. Respite care allowed families to have a
break but still remain as involved as they wished.
Hospice clinicians generally showed them compassion
and respect. These factors, taken together, led most of
the participants to endorse hospice care.
Hospices could provide better support with end-oflife
care for Ma¯ori people. Marketing hospices as
resources that support wha¯nau as they care for their
loved one with a terminal illness at home or within the
hospice would help to address negative perceptions of
hospice care (Bray and Goodyear-Smith, 2013). There
was also a need to counteract misperceptions of
hospice care as shortening life, and to make it clear
that hospice care could ease unnecessary distress, and
potentially prolong life (Temel et al, 2010).
The participants recognised that their culture was
changing and that therewas a diversity ofMa¯ori beliefs
and practices. Given the extraordinarily dynamic nature
of Ma¯ori culture, it is important to continue to study
how best to support Ma¯ori people at the end of life,
and to exercise flexibility. Clinicians must be prepared
to cater for diverse expressions and experiences of
Ma¯ori culture and incorporate tikanga Ma¯ori practices
with sensitivity.
Study limitations
This study has some limitations that will affect the
extent to which the findings can be generalised. It was
a very small study, with only 12 participants from the
Wellington region, so it cannot be assumed that the
perceptions held by these participants are reflective of
all Maori patients and wha¯nau. The perspectives of
Ma¯ori people from the south end of the North Island or other regions of the country were not included. In
addition, the study focused on those who had experienced
hospice care at one particular hospice, and the
results are therefore inevitably specific to this particular
service.
Conclusion
This exploration of the perspectives of Ma¯ori people
about end-of-life care in a hospice shows how one
indigenous people’s knowledge and praxis in this
regard interfaces with a Eurocentric approach to care.
Although the concept of hospice care reflects a western
paradigm, these findings suggest that there are aspects
of holistic hospice care that could be readily aligned
with the Ma¯ori hauora framework and used by palliative
care professionals to provide culturally safe care.
ACKNOWLEDGEMENTS
The authors are grateful to the New Zealand Health
Research Council for funding this Ma¯ori Seeding
Grant, as well as Mary Potter Hospice’s Maori advisory
group Te Pou Tautoko, the wha¯nau and kauma¯tua
who shared their personal knowledge for this study,
and Katherine Reweti-Russell, Project Facilitator,
Ma¯ori Health Development Group, Capital and Coast
District Health Board, Wellington, New Zealand.
References
- Barlow C (1994) TikangaWhakaaro: key concepts in MaÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡Ãâïori culture. Auckland: Oxford University Press.
- Bray Y and Goodyear-Smith F (2013) Patient and family perceptions of hospice services: ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âI knew they werenÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢t like hospitals.ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ Journal of Primary Health Care 5:206ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â13.
- Capital Coast District Health Board (undated) Maori Health Action Plan. Te Plan II: 2007ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â2012. www.ccdhb.org.nz/ Planning/Maori_Health/docs/Te_plan2_web.pdf (accessed 30 August 2013).
- Cram F, Smith L and Johnstone W (2003) Mapping the themes of MaÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡Ãâïori talk about health. New Zealand Medical Journal 116. www.nzma.org.nz/journal/116ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â1170/357 (accessed 5 January 2013).
- Durie MH (1985) A MaÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡Ãâïori perspective of health. Social Science and Medicine 20:483ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â6.
- Frey R, Gott M, Raphael D et al (2013) ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âWhere do I go from hereÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢? A cultural perspective on challenges to the use of hospice services. Health and Social Care 21:519ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â29.
- Health Research Council of New Zealand (2008) Guidelines for Researchers on Health Research involving MaÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡Ãâïori. Auckland, New Zealand: Health Research Council of New Zealand.
- Hotson KE, Macdonald SM and Martin BD (2004) Understanding death and dying in select first nations communities in northern Manitoba: issues of culture and remote service delivery in palliative care. International Journal of Circumpolar Health 63:25ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â38.
- Johnston G, Vukic A and Parker S (2013) Cultural understanding in the provision of supportive and palliative care: perspectives in relation to an indigenous population. BMJ Supportive and Palliative Care 3:61ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â8.
- Kelly L, Linkewich B, CromartyHet al (2009) Palliative care of First Nations people: a qualitative study of bereaved family members. Canadian Family Physician 55:394ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â5.e7.
- Lincoln YS and Guba EG (1985) Naturalistic Inquiry. Newbury Park, CA: Sage. McGrath P and Phillips EL (2009) Insights from the Northern Territories on factors that facilitate effective palliative care for Aboriginal peoples. Australian Health Review 33:636ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â44.
- Ministry of Health (2001) The New Zealand Palliative Care Strategy. Wellington, New Zealand: Ministry of Health. www.health.govt.nz/publication/new-zealand-palliativecare- strategy (accessed 1 September 2013).
- Ministry of Health (2012) MaÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡Ãâïori Health Models ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â TeWhare Tapa WhaÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡Ãâï. www.health.govt.nz/our-work/populations/ maori-health/maori-health-models/maori-health-modelste- whare-tapa-wha (accessed 5 January 2013).
- OÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢Brien AP, Bloomer MJ, McGrath P et al (2013) Considering Aboriginal palliative care models: the challenges for mainstream services. Rural and Remote Health 13:2339.
- Palliative Care Subcommittee, New Zealand Cancer Treatment Working Party (2007) New Zealand Palliative Care: a working definition. www.health.govt.nz/system/files/ documents/publications/nz-palliative-care-definitionoct07. pdf (accessed 30 August 2013).
- Patton MQ (2002) Qualitative Research and Evaluation Methods, 3rd edn. Thousand Oaks, CA: Sage. Robson B and Harris R (2007) Hauora: MaÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡Ãâïori standards of health IV. Wellington, New Zealand: TeRoÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡ÃâïpuÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡Ãâï RangahauHauoraaEruPoÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡Ãâïmare.
- Ruff CC, Alexander IM and McKie C (2005) The use of focus group methodology in health disparities research. Nursing Outlook 53:134ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â40.
- Schwass M (2005) Last Words: approaches to death in New ZealandÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s cultures and faiths. Wellington, New Zealand: Bridget Williams Books.
- Smith LT (1999) Decolonizing Methodologies: research and indigenous peoples. London: Zed Books. Statistics New Zealand (2011) QuickStats about Culture and Identity. www.stats.govt.nz/Census/2006CensusHome Page/QuickStats/quickstats-about-a-subject/culture-andidentity/ ethnic-groups-in-new-zealand.aspx (accessed 5 January 2013).
- Taylor EJ, Ensor B and Stanley J (2012) Place of death related to demographic factors for hospice patients in Wellington, Aotearoa New Zealand. Palliative Medicine 26:342ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â9.
- Temel JS, Greer JA, Muzikansky A et al (2010) Early palliative care for patients with metastatic non-smallcell lung cancer. New England Journal of Medicine 363:733ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â42.
- United Nations (2007) United Nations Declaration on the Rights of Indigenous Peoples. www.un.org/esa/socdev/ unpfii/documents/DRIPS_en.pdf (accessed 4 June 2012).
- Waldon J (2003) OrangaKaumaÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡Ãâïtua: perceptions of health in older MaÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡Ãâïori people. Pacific Health Dialogue 10:79ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â86.
- Walker T, Signal L, RussellMet al (2008) The road we travel: MaÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡Ãâïori experience of cancer. New Zealand Medical Journal 121:27ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â35.


