Sushil K Ahlawat
Division of Gastroenterology, University of Medicine and Dentistry of New Jersey. Newark, NJ, USA
- *Corresponding Author:
- Sushil K Ahlawat
UMDNJ-New Jersey Medical School
MSB H-534 185 South Orange Ave Newark
NJ 07103 USA
Phone: +1-973.972.2954
Fax: +1-973.972.3144
E-mail: sushilka@aol.com
Received November 9th, 2007 - Accepted January 14th, 2008
Keywords
Biopsy, Cytology; Fine-Needle; Cysts; Endosonography; Pancreas; Pancreatic Cyst
Abbreviations
LEC: lymphoepithelial cyst
Dear Sir
endoscopic ultrasound-guided fined needle aspiration (EUS-FNA) of pancreatic lesions is now well accepted in clinical practice since it allows for a definitive diagnosis of most pancreatic lesions. EUS-FNA is used increasingly for patients with pancreatic cystic lesions to distinguish lesions that must be resected from lesions that can be managed expectantly. Lymphoepithelial cysts (LECs) of the pancreas are extremely rare, benign, nonneoplastic cysts that can simulate cystic neoplasms clinically and radiographically. Endosonographic as well as cytologic features of LECs are poorly defined because of their rarity. We conducted a systematic review of MEDLINE/PubMed to identify patients with LEC reported in the English language literature that were diagnosed with a CT- or EUS-guided FNA to study the role of EUSFNA in differentiating pancreatic LECs from other cystic lesions of the pancreas.
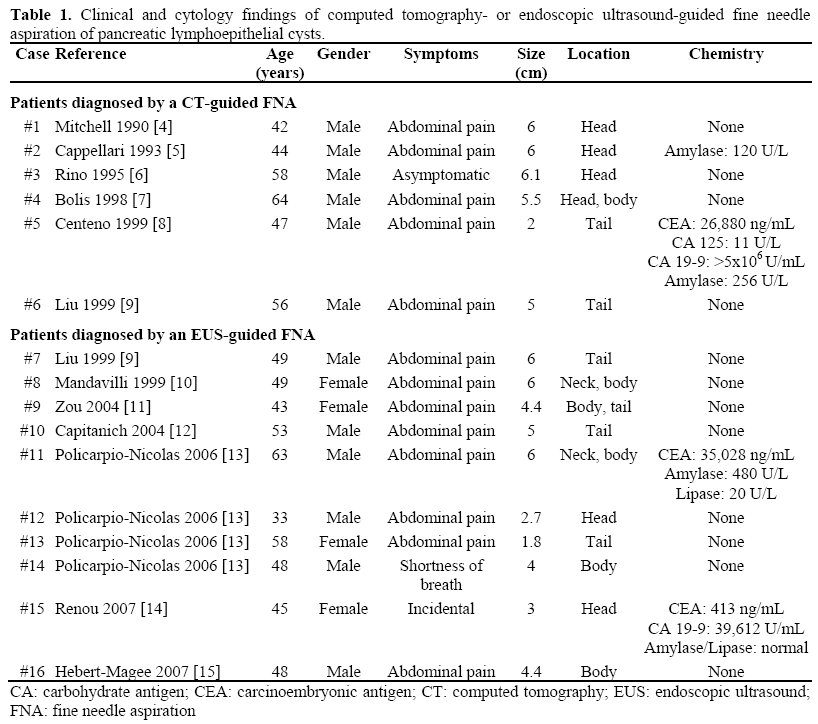
The systematic search of MEDLINE/PubMed database from 1950 to 2007 was conducted using the MeSH terms “pancreas” and “cyst”. The search was limited to “Humans” and “English” language. The search revealed a total of 1,988 articles, each article was reviewed. The bibliography of the relevant articles was also searched to identify additional studies. A total of 16 patients with lymphoepithelial cyst diagnosed by a CT or EUS guided FNA were identified and are summarized in Table 1.
The term “LEC of the pancreas” was proposed by Truong et al. in 1987 [1]. The morphologic findings are distinctive and were first described by Luchtrath and Schriefers, who noted the histologic similarity to brachial cleft cyst of the lateral neck [2]. The etiopathogenesis as well as histogenesis of LECs remain unclear; however, the lesions are not believed to be neoplastic and to date no metastatic behavior has been reported. The largest series in the literature was reported by Adsay et al. [3], which included a total of 12 patients. LECs occur in both genders at any age, but more commonly in the middle-age man. The lesion may appear either intrapancreatic or peripancreatic and may be either uniloculated or multiloculated containing keratinous debris.
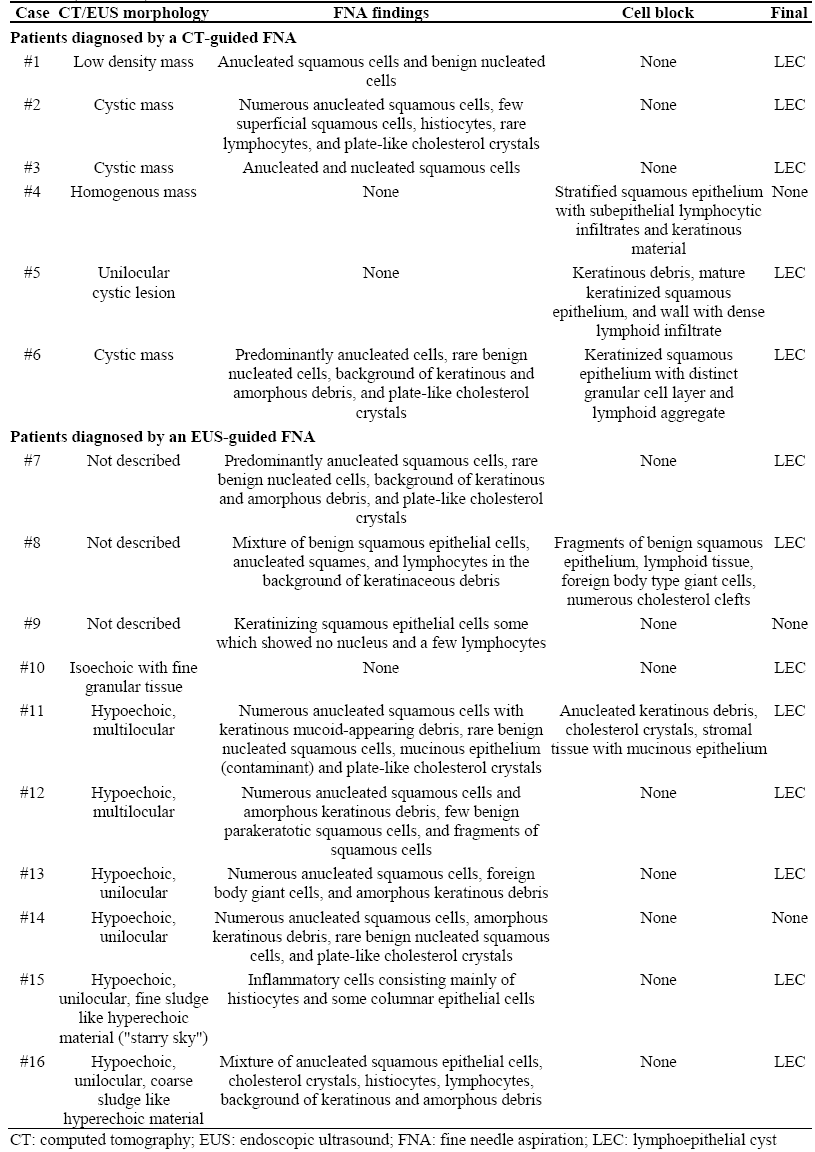
The first description of cytologic findings of LECs was published by Mitchell in 1990 [4]. However, the definite criteria for cytologic diagnosis of LECs are not available likely because of rarity of this clinical condition. To our knowledge, 16 patients with LECs have been reported who were diagnosed by CT- or EUS-guided FNA (Table 1). The FNA specimens typically showed abundant anucleated squamous cells with few benign appearing nucleated squamous cells; keratinous and amorphous debris; occasional multinucleated giant cells; and plate-like cholesterol crystals. The presence of lymphocytes was variable in FNA specimens likely because of sampling error, aspiration of cyst content as opposed to cyst wall aspiration. The occasional presence of mucinous epithelium suggests contamination with duodenal or gastric epithelium.
LECs appears hypoechoic, uniloculated (Figure 1) or multiloculated on EUS. Occasionally, fine or coarse sludge like hyperechoic echo architecture is also seen likely due to the debris within the cyst (Figure 1). Differential diagnosis of LEC may include pseudocyst or cystic neoplasm of the pancreas such as mucinous cystic neoplasm and intraductal papillary mucinous neoplasm. Squamous epithelium should not be seen in aspirates from pseudocyst and amylase levels are usually elevated markedly, whereas CEA levels are usually lower [8]. Aspirates from mucinous cysts usually show background extracellular mucus with or without mucinous epithelium. However, the degenerated squamous material of LEC may be misinterpreted as mucoid material [10, 13]. Chemical analysis of pancreatic LECs fluid has been reported rarely (Table 1). Normal or slightly increased amylase levels and high CEA and CA 19-9 have been reported [8, 13, 14]. Significant increase in CEA and CA 19-9 can be misinterpreted leading to a false diagnosis of mucinous neoplasm especially because EUS-guided FNA samples may show both squamous and glandular contaminant. However, the presence of abundant anucleated squamous epithelium should favor a diagnosis of pancreatic LEC.
Figure 1. Endosonographic view showing the
hypoechoic lesion (arrow) with hyperechoic sludge
like material likely representing debris (arrowheads);
the lesion was resected and confirmed to be a
lymphopithelial cyst on histopathology.
If the patients is asymptomatic and EUS-FNA firmly establishes the diagnosis of LEC based on cytological examination of the cyst fluid, surgery can be avoided and then patient may be followed with serial cross-sectional imaging of the upper abdomen [16]. However, the absence of LEC cytological proof does not definitely rule out LEC diagnosis, even if high CEA and CA 19-9 levels are recorded in the cyst fluid [8, 13, 14]. Several types of surgical treatment options are available in patients who are symptomatic and these include simple enucleation or pancreatectomy (distal or pancreaticoduodenectomy).
In conclusion, LECs of pancreas are extremely rare, nonneoplastic cysts of the pancreas. Definite pre-operative diagnosis may be possible based on clinical and cytologic features and thus allowing conservative management. However, clinician should be aware of certain pitfalls of cyst fluid analysis (elevated CEA and CA 19-9 in some patients) that may prevent a correct preoperative diagnosis. In such patients surgery is a reasonable option for definitive diagnosis.
Conflict of interest
The author has no potential conflicts of interest
References
- Truong LD, Rangdaeng S, Jordan PH Jr. Lymphoepithelial cyst of the pancreas. Am J Surg Pathol 1987; 11:899-903. [PMID 3674287]
- Luchtrath H, Schriefers KH. A pancreatic cyst with features of a so-called branchiogenic cyst.
Pathologe 1985; 6:217-9. [PMID 4048076]
- Adsay NV, Hasteh F, Cheng JD, Bejarano PA, Lauwers GY, Batts KP, et al. Lymphoepithelial cysts of the pancreas: a report of 12 cases and a review of the literature. Mod Pathol 2002; 15:492-501. [PMID 12011254]
- Mitchell ML. Fine needle aspiration biopsy of peripancreatic lymphoepithelial cysts. Acta Cytol 1990; 34:462-3. [PMID 2343707]
- Cappellari JO. Fine-needle aspiration cytology of a pancreatic lymphoepithelial cyst. Diagn Cytopathol 1993; 9:77-81. [PMID 8458289]
- Rino Y, Morohoshi T, Funo K, Imada T, Yamamoto Y, Jojima T, et al. Lymphoepithelial cyst of the pancreas: a preoperatively diagnosed case based on an aspiration biopsy. Surg today 1995; 25:1043-6. [PMID 8645938]
- Bolis GB, Farabi R, Liberati F, Macciò T. Lymphoepithelial cyst of the pancreas. Report of a case diagnosed by fine needle aspiration biopsy. Acta Cytol 1998; 42: 384-6. [PMID 9568141]
- Centeno BA, Stockwell JW, Lewandrowski KB. Cyst fluid cytology and chemical features in a case of lymphoepithelial cyst of the pancreas: A rare and difficult preoperative diagnosis. Diagn Cytopathol 1999; 21:328-30. [PMID 10527479]
- Liu J, Shin HJ, Rubenchik I, Lang E, Lahoti S, Staerkel GA. Cytologic features of lymphoepithelial cyst of the pancreas: two preoperatively diagnosed cases based on fine-needle aspiration. Diagn Cytopathol 1999; 21:346-50. [PMID 10527483]
- Mandavilli SR, Port J, Ali SZ. Lymphoepithelial cyst (LEC) of the pancreas: cytomorphology and differential diagnosis on fine-needle aspiration (FNA). Diagn Cytopathol 1999; 20:371-4. [PMID 10352910]
- Zou XP, Li YM, Li ZS, Xu GM. Lymphoepithelial cyst of the pancreas: a case report. Hepatobiliary Pancreat Dis Int 2004; 3:155-7. [PMID 14969862]
- Capitanich P, Iovaldi ML, Medrano M, Malizia P, Herrera J, Celeste F, et al. Lymphoepithelial cysts of the pancreas: case report and review of the literature. J Gastrointest Surg 2004; 8:342-5. [PMID 15019932]
- Policarpio-Nicolas ML, Shami VM, Kahaleh M, Adams RB, Mallery S, Stanley MW, et al. Fine-needle aspiration cytology of pancreatic lymphoepithelial cysts. Cancer 2006; 108:501-6. [PMID 17063496]
- Renou C, Giovannini M, Monges G, Rifflet H, Muller P, Harafa A, et al. Pitfalls of cyst fluid findings obtained by endoscopic ultrasonography fine-needle aspiration on a pancreatic lymphoepithelial cyst. Am J Gastroenterol 2007; 102:213-5. [PMID 17278274]
- Hebert-Magee S, Garvin D, Ahlawat SK, Haddad N, et al. Lymphoepithelial cyst of the pancreas with sebaceous differentiation: Cytomorphology and diagnosis on fine-needle aspiration. Diagn Cytopathol 2008 (In press).
- Anagnostopoulos PV, Pipinos II, Rose WW, Elkus R. Lymphoepithelial cyst in the pancreas: a case report and review of the literature. Dig Surg 2000; 17:309-14. [PMID 10867475]


