Keywords
Carcinoembryonic Antigen; Cysts; Pancreas
Abbreviations
CEA carcinoembryonic antigen; CECT contrastenhanced
computed tomography; EUS Endoscopic Ultrasound; LEC
lympho epithelial cysts
INTRODUCTION
Lympho Epithelial Cysts of the pancreas are benign,
slow growing lesions in the pancreas. Due to their rarity,
they have been described most often in individualised case
reports in medical literature. The aim of this article is to
analyse these rare cysts in detail so as to form meaningful
conclusions for further treatment and management.
OUR CASE
A thirty-three-year-old female patient presented with
history of vague abdominal pain and backache for 6 months
duration. The pain was confined to the epigastric region
with no radiation of pain. There were no other symptoms.
Patient had previous history of emergency splenectomy
done 20 years back for trauma. Other medical records
pertaining were unavailable. CECT abdomen (Figures 1,
2) done revealed a homogenous cystic lesion at the tail
of the pancreas. Ultrasound guided aspiration of the cyst
revealed a paucicellular, straw coloured infiltrate, negative
for malignant cells. Fluid CEA-2ng/mL (N<2.5 ng/mL), F. CA19-9 was 148 IU/mL (N-<37 IU/mL). Serum CA19-9
and S.CEA were normal. In view of persistent abdominal
pain and increased fluid CA19-9, it was decided to proceed
with surgery. Intraoperatively, 5 cm smooth walled cystic
lesion was seen in the tail of pancreas. As the lesion was
adherent to the tail of the pancreas without a clear plane
of separation from the pancreas and as malignancy could
not be conclusively ruled out, it was decided to proceed
with distal pancreatectomy (Figure 3). Cut section of
the cyst revealed a thick greasy material with smooth
wall. Histopathology of cyst revealed stratified squamous
epithelium with overlying layer of lymphoid tissue. This
was consistent with a diagnosis of lymphoepithelial cyst of
pancreas. Post operative course was uneventful.
Figure 1. Cect showing 5 × 5 cm homogenous cystic lesion (arrow) adherent to the tail of pancreas Note the post splenectomy status.
Figure 2. Cect showing eccentric unilocular cyst ( arrow) at the tail of pancreas.
Figure 3. Intraoperative showing distal pancreatectomy specimen with cyst(arrow) attached to tail of pancreas.
METHODOLOGY
All cases of lymphoepithelial cysts described in
literature were analysed after a thorough search of medical
literature and databases like PUBMED. Though most cases
described are case reports, there are a few recent case
series of the same also. All reports were divided into three
periods based on two landmark publications by Adsay et al. [1] in 2002 and by sekwani et al. [2] in 2010.
Our aim was to analyse the incidence, geographical
location, patient variables like age, sex, symptoms,
location of cyst in pancreas including type, treatment
offered and follow up of Lymphoepithelial cysts (LEC)of
pancreas based on the three periods to observe for changes
in management over time.
Based on our study, we analysed a total of 235 cases
(including our case) which were divided into (Figure 4)
Figure 4. Scheme of study.
Till 2002 (till Adsay et al.) - 82 cases
2003-2010 (till Sekwani et al.) - 69 cases
2011- till date (after Sekwani et al. -till date) - 84
cases(including our case)
Over time, it is seen that a there is an increasing trend
towards increased non operative “wait and watch” which
is made possible due to increased accuracy in diagnosis of
LEC. Further information on the methodology and cases
considered is in annexure 1.
Inclusion Criteria
All cases of lymphoepithelial cysts in the pancreas
and peripancreatic area were included in the study. The
diagnosis of LEC in operated cases rested on histopathology
which showed a cystic lesion lined by stratified squamous
epithelium surrounded by lymphoid tissue in the absence of
skin appendages like hair. Though some cases were described
previously in literature as “epidermoid cyst derived from
an accessory spleen in the pancreas” or “accessory splenic
epidermoid cyst”, the pathologic description and illustrations
for these cases were suggestive of a lymphoepithelial cyst [3, 4, 5, 6, 7, 8, 9, 10, 11].
Exclusion Criteria
Other cystic lesions of pancreas including malignancy,
benign lesions like dermoid cyst and some early cases
reported with incomplete information were excluded.
RESULTS
The following inference could be made on the data
analysed.
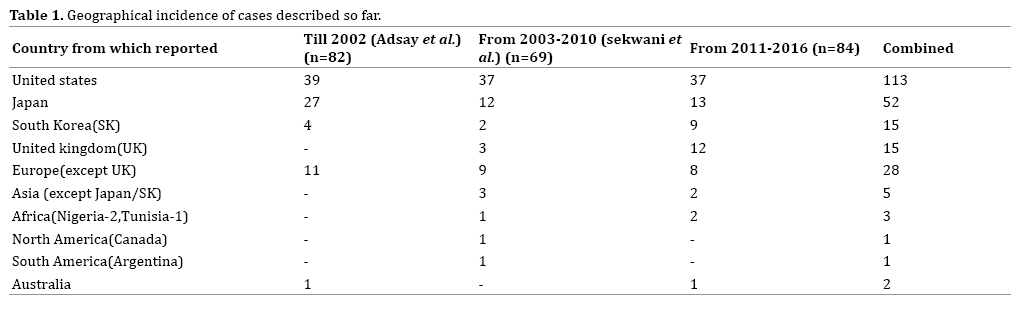
Incidence
LEC are probably worldwide in distribution with most
cases (70.2%) being reported from the United States
(n=113, 48.8%) and Japan (n=52, 22.1%) (Table 1). The
term “lymphoepithelial cyst” was coined by Troung in
1987 [12]. However, cases suggestive of lymphoepithelial
cysts have been described in literature since 1980. The
data has been increasing annually over time with most
cases reported so far in 2006 (31 cases) (Figure 5). The
vast majority (N=108) (45.9%) of reported cases are single
case reports with some large case series being reported
recently. The largest case series reported so far is by Dalal et al. (16 cases) [13], followed by Adsay et al. [1] (12 cases)
with Nasr et al. [14] and Raval et al. (9 cases each) [15].
Figure 5. LEC cases described by year.
Patient Variables
LEC are most commonly seen in the middle aged with
a male preponderance of 4:1 (n=189, 80.4%). Overall,
LEC are frequently symptomatic (50.2%) (Table 2). The
number of asymptomatic cases (40.85%) is rising steadily
in world literature due to better accuracy in radiological
investigations (Table 3). Among those symptomatic, the
most common symptom was abdominal pain (77.9%) in
92 patients followed by weight loss (Figure 6). LEC are
usually solitary (n=228) and eccentrically situated within
the pancreas (99.1%) (Table 4). The most common
pancreatic site is distal to the pancreatic neck where it
is most common in the tail (n=98, 41.7%) followed by the body (66, 28.1%) and head (n=64, 27.2%) (Figure 7).
Mean size of the cysts is 4.7 cm. Symptomatic cysts had larger
diameter compared to asymptomatic cysts (5.2 vs. 4.8 cm)
and patients treated by intervention had significantly larger
size to those cysts treated by conservative non operative
management (4.9 vs. 4 cm) (Table 5). Most common
morphological pattern seen is multilocular (48.9%) followed
by unilocular cysts (43.8%) (Figure 8).



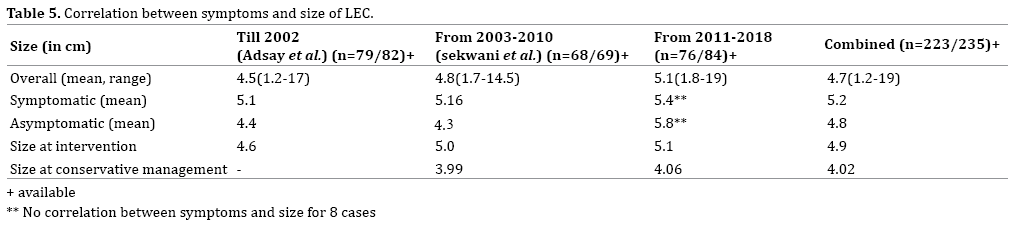
Figure 6. Symptomatology of LEC.
Figure 7. Location of LEC.
Figure 8. Morphology of LEC.
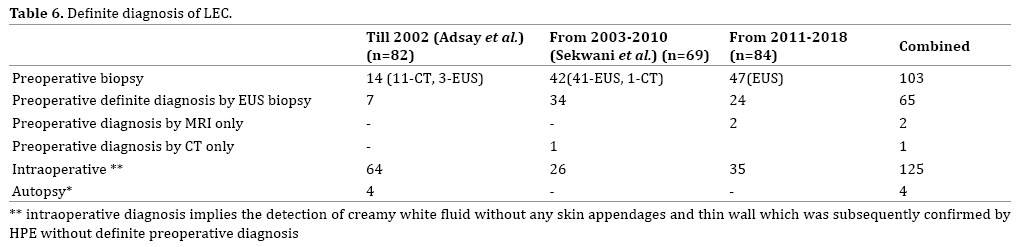
DIAGNOSIS OF LEC
Interventional Biopsy and Fluid Analysis (EUS/CT
Guided)
Most cases of LEC are diagnosed preoperatively by EUS
guided biopsy and analysis of fluid for tumour markers.
Though the incidence of preoperative biopsy is increasing,
only 43.8% (N=103) underwent a preoperative biopsy as
part of management, with most recent cases undergoing
EUS guided biopsy (Table 6). LEC are characteristically
acellular, clear, straw –yellow or cheesy white with keratin
debris and cholesterol or fat deposition. Jian et al. suggests that FNA helps in accurate diagnosis obviating unnecessary
surgery [16]. It is seen that though EUS guided biopsy
helps to conclusively diagnose LEC, it may be inconclusive
in many. EUS guided trucut biopsy has been suggested for
those with equivocal results on EUS FNA to increase the
yield [17].
The findings on EUS may be suggestive of LEC,
suspicious of malignancy or inconclusive (Table 7).

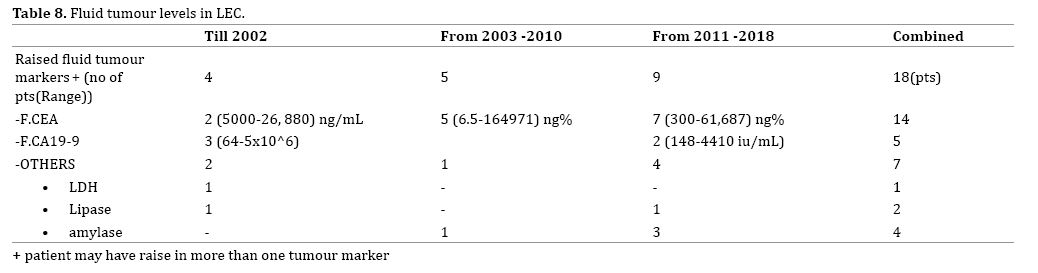
Fluid CEA levels are the most commonly elevated fluid
tumour marker where a tumour marker of the fluid was
done (Table 8). CEA levels may often be elevated due to
goblet cells or the aberrant immunoreactive squamous
epithelial lining [15]. Therefore an algorithmic approach
for diagnosis of mucinous neoplasm with no solid
component on EUS and cyst fluid CEA level of more than
200ng/mL, may not hold good if LEC is also borne in mind
[18].
CT Imaging
CT imaging is associated with varied presentations.
This may range from characteristic well circumscribed,
low attenuating masses with enhancing rims to lobulated, non-enhancing and sharply demarcated lesions with focal
calcifications. Most lesions are often associated with the
absence of pancreatic ductal dilatation or atrophy [19].
Some lesions may also show variability like unilocularity
with clear wall enhancements, regions of fat attenuation,
papillary projections, small solid components, wall
calcification or thin wall enhancement on conventional CT
imaging [19, 20].
This variation has led to the argument that threedimensional
computed tomography (3D-CT) scan, rather
than the conventional scan, may be better suited to
differentiate lymphoepithelial cysts from other lesions of
the pancreas [21] primarily because of their predominantly
extra-pancreatic 3D location and higher precontrast CT
attenuation. Moreover, it is to be noted that LEC are seen
to be smaller and more frequently micro lobulated than
mucinous cystadenomas [22].
MRI
MRI has been proposed as an accurate investigatory
tool in case of equivocal findings on EUS. This is primarily
due to its characteristic, high signal intensity on T1 and low signal intensity on T2 weighted imaging. Definite MRI
characteristics include “cheerio’s ”appearance of multiple
central hypo intensity with peripheral hyper intensity in
T2 phase [22], profound water restriction on Diffusion
weighted imaging (DWI) [23], or slight signal reduction
in out-of-phase when compared to in-phase, because of
intraregional variations in fat and water [24].
ERCP
ERCP is not useful to diagnose LEC. It is mostly done
when other cystic lesions like IPMN are suspected. Most
were described in older case reports where an ERCP failed
to show any associated abnormality or communication in
the pancreatic duct.
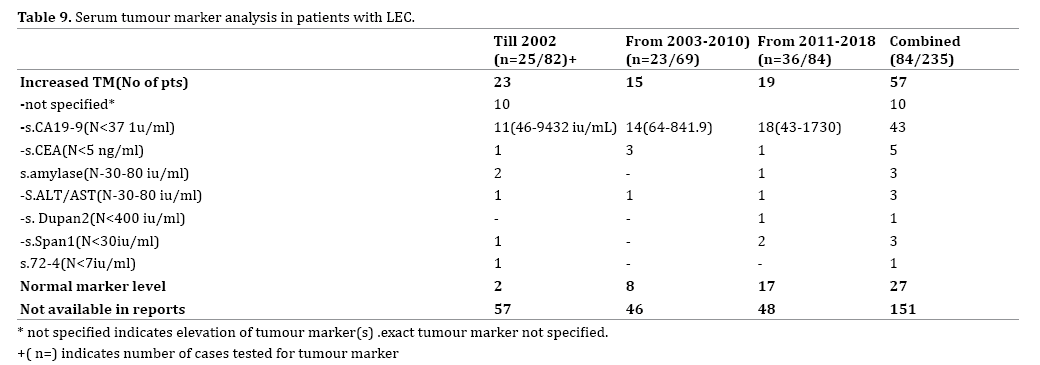
Serum Tumour Markers
LEC is associated with increased serum and fluid
tumour markers which cause diagnostic dilemma
especially in equivocal cases. 34.8% (n=82) of cases had
serological tumour markers (S.CEA, S.CA19-9 or DUPAN-2)
done, of whom 67.07% (n=55) had at least one marker
increased beyond normal limits. S. CA19-9 levels were the
most common tumour markers elevated with a wide range
of values (range-43- 9432 iu/mL). It occurred in 72.7%
(n=40) of those with elevated tumour markers followed by
S.CEA (range- 5-1582 ng/mL) (Table 9). It is interesting
to note that there is a fall in most cases of CA19-9 after
surgical excision in patients with elevated CA19-9 levels.
Treatment
Though a conservative approach is the ideal treatment
in asymptomatic preoperatively diagnosed cases of LEC,
it was done in only 11.5% of cases (n=27) overall. Most
cases of LEC were offered surgery. The indications for
surgery include previously diagnosed LEC cysts becoming
symptomatic over time, diagnostic uncertainty or
suspicion of malignancy. From our analysis, it is seen that
local excision of the cyst alone (n=90, 38.2%) and distal
pancreatic resection (n=90, 38.2%) were the common
procedures performed for symptomatic cysts (Table 10).
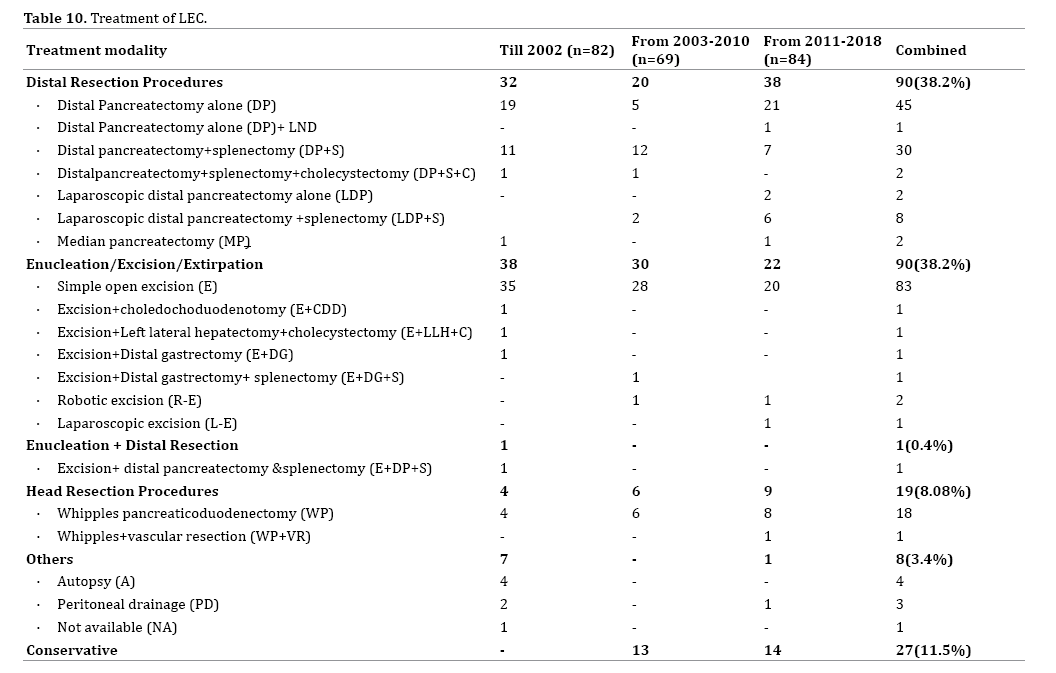
Pancreas preserving procedures like local excision,
in patients with a definite diagnosis, obviate the need
for morbid pancreatic resection. Newer approaches like
laparoscopy and robotic surgery have been tried in an
effort to further reduce the morbidity of these procedures.
Post Treatment Follow Up
Of all patients on a non-operative “wait and watch”
approach, data of the follow up was available for 51.8%
(n=14) of these patients with a mean follow up of 26.14
months (range-3-62months). Most of the patients (85.7%)
who were on conservative wait and watch reported no
increase in size. However, very rarely, increase in size of
cyst resulting in symptoms necessitating surgery was seen
as was spontaneous resolution [17, 25]. Follow up reports
after surgery was available for 39% (n=78) of patients with a median follow up of 7.5 months (range-1 day -125
months). Most common complications after pancreatic
resection included pulmonary complications, pancreatic
fistula (most common after a distal pancreatectomy) which
was usually self-limiting, bleeding, pseudocyst of pancreas,
and cyst spillage during surgery.
HISTOLOGY
The gold standard for diagnosis of LEC is histopathology
which is quite characteristic with its cheesy, white, greasy
porridge like material contained by multiple septations
and a thin wall of squamous epithelium with surrounding
lymphoid follicles. Microscopy usually reveals absence of
skin appendages like hair which is vital to differentiate it from dermoid cyst. Sebaceous differentiation of the
epithelium may be present, but is rare [26, 27]. The
organism S. Heidelberg et al. has been found in the cyst
[28] raising speculation on the presence of infection as a
causative factor. However, its exact role is unknown and is
not reported in other reports (Figure 9).
Figure 9. Treatment algorithm for LEC.
AETIOLOGY
Though the exact aetiology of these cysts is unclear, the
following hypotheses are considered. Troung’s hypothesis
on the histogenesis of LEC include the following [29]:
Proliferation of the ectopic remnant of a brachial cyst
in the pancreas. This theory is highly unlikely due to the
intraabdominal nature of lesion.
Squamous metaplasia of an obstructed pancreatic duct
followed by protrusion into the peripancreatic lymph
nodes.
Squamous metaplasia of ectopic pancreatic tissue in a
peripancreatic lymph node. This theory is most likely and is
supported by evidence [6] including the eccentric location
at the pancreas [7] and the occurrence in peripancreatic
lymph nodes [10, 29].
Epithelial antigen attraction by lymphocytes induces
the differentiation into squamous cells with surrounding
lymphocytes [30, 31].
There has been an active interest into whether an
association with various viruses like EBV, HIV etc. is
present. So far, though there are some case reports of
occurrence of LEC in HIV patients, further evidence is
lacking [31, 32].
CONCLUSION
Based on our findings and other reports, a reasonable
treatment algorithm for lymphoepithelial cysts of pancreas
would be as in figure 9 [15].
Conflict of Interest
Authors declared no conflict of interest and financial
disclosure.
References
- Adsay NV, Hasteh F, Cheng JD, Bejarano PA, Lauwers GY, BattsKP, et al. Lymphoepithelial cyst of the pancreas: a report of 12 cases and a review of the literature. Mod Pathol 2002; 15:492–501. [PMID: 12011254]
- Sewkani A, Purohit D, Singh V, Jain A, Varshney R, Varshney S. Lymphoepithelial cyst of the pancreas: a rare case report and review of literature. Indian J Surg 2010; 72:427–432. [PMID: 22131649]
- Davidson ED, Campbell WG, Hersh T. Epidermoid splenic occurring in an intrapancreatic accessory spleen. Dig Dis Sci 1980; 25:964-967. [PMID: 7449592]
- Yamada K, Murao S, Yoshida H, Nakajima T, Yoshii M, Kimujra M, et al. A case of accessory splenic epidermoid cyst [in Japanese]. Nippon Nuiku Gakkai Zusshi 1981; 70:1007-1011. [PMID: 7288251]
- Jibu T, Nagai H, Senba D, Wada Y, Kuroda A, Moriyoka Y, et al. A case of epidermoid cyst occurringin an intrapancreatic accessory spleen [in Japanese]. Nihon Shokakibyo Gakkai Zasshi 1987; 84:1859-1862. [PMID: 3323581]
- Carr RF, Tang CK, Carrozza MJ, Rodriguez FC. Unusualcystic epithelial choristoma in a celiac lymph node. Hum Pathol 1987; 18:866–869. [PMID: 3610139]
- Takiguchi Y, Wada K, Matsuno H, Nakashima M. Effect of diabetes on photochemically induced thrombosis in femoral artery and platelet aggregation in rats. Thromb Res; 63:445-456. [PMID: 1754997]
- Horie Y, Taguchi K, Akagi T, Ohta T. Lymphoepithelial cyst in per pancreatic lymph node. J Okayama Surg Pathol Assoc 1990; 27:53–57.
- Morohoshi T, Hamamoto T, Kunimura T, Yoshida E, Kanda M, Funo K, et al. Epidermoid cyst, derived from an accessory spleen in the pancreas: a case report with literature survey. Acta Pathol Jpn1991; 41:916-921. [PMID: 1785350]
- Arai T, Kino I, Nakamura S, Ogawa H. Epidermal inclusion in abdominal lymph nodes. Acta Pathol Jpn 1992; 42:126–129. [PMID: 1561883]
- Ohta T, Nagakawa T, Fukushima W, Ueno K, Kayahara M, Kanno M, et al. Carbohydrate Antigen 19-9-Producing Lymphoepithelial Cyst of the Pancreas: A Case Report with an Immunohistochemical Study. Dig Surg 1992; 9:221–225.
- Maass CJ, Fronticelli ML, Macrì D, Regge A, Sapino A, Veltri. Lymphoepithelial cyst of the pancreas:radiological and pathological findings. Eur Radiol 1995; 5:448-450.
- Dalal KS, DeWitt JM, Sherman S, Cramer HM, Tirkes T, Al-Haddad MA. Endoscopic ultrasound characteristics of pancreatic lymphoepithelial cysts: A case series from a large referral center. Endosc Ultrasound 2016; 5:248-253. [PMID: 27503157]
- Nasr J, Sanders M, Fasanella K, Khalid A, McGrath K. Lymphoepithelial cyst of the pancreas: an EUS case series.Gastrointest Endosc 2008; 68:170–173. [ PMID: 18513719]
- Raval JS, Zeh HJ, Moser AJ, Lee KK, Sanders MK, Navina S, et al. Pancreatic lymphoepithelial cysts express CEA and can contain mucous cells: potential pitfalls in the preoperative diagnosis. Mod Pathol 2010; 23:1467–1476. [PMID: 20802468]
- Jian B, Kimbrell HZ, Sepulveda A, Yu G. Lymphoepithelialcysts of the pancreas: endosonography-guided fine needle aspiration. Diagn Cytopathol 2008; 36:662–665. [ PMID: 18677749]
- Ali S, Wilkinson N, Jensen CS, Gerke H. EUS-guided Trucut biopsies may enable the diagnosis of lymphoepithelial cysts of the pancreas. Report of two cases. JOP 2009; 10:409–412. [PMID: 19581745]
- Vignesh S, Brugge WR. Endoscopic diagnosis and treatment of pancreatic cysts. J Clin Gastroenterol 2008; 42:493–506. [PMID: 18344889]
- Kim WH, Lee JY, Park HS, Won HJ, Kim YH, Choi JY, et al. Lymphoepithelial cyst of the pancreas: comparison of CT findings with other pancreatic cystic lesions. Abdom Imaging 2013; 38:324–330. [PMID: 22610041]
- Policarpio-Nicolas ML, Shami VM, Kahaleh M, Adams RB, Mallery S, Stanley MW, et al. Fine-needleaspiration cytology of pancreatic lymphoepithelial cysts. Cancer 2006; 108:501–506. [PMID: 17063496]
- He´bert-Magee S, Garvin D, Ahlawat S, Haddad N. Lymphoepithelial cyst of the pancreas with sebaceous differentiation: cytologic diagnosis byfine-needle aspiration. Diagn Cytopathol 2009; 37:937– 939. [PMID: 19795493]
- Matrone A, Russo M, Mollica C, Lombardi D, Lombardi G, Maurea S, et al. Lymphoepithelial pancreatic cyst: an atypical benign pancreatic mass presenting with a ‘cheerios-like’ appearance. JOP 2010; 11:170–172. [PMID: 20208329]
- Nam SJ, Hwang HK, Kim H, Yu JS, Yoon DS, Chung JJ, et al. Lymphoepithelial cysts in the pancreas: MRI of two cases with emphasis of diffusion-weighted imaging characteristics. J Magn Reson Imaging 2010; 32:692–696. [PMID: 20815068]
- Kudo D, Hashimoto N, Toyoki Y, Narumi S, Hakamada K. Usefulness of in-phase and out-of-phase magnetic resonance imaging for the detection of pancreatic lymphoepithelial cyst. Hepatogastroenterology 2011; 58:1403–1405. [PMID: 21937416]
- Bédat B, Genevay M, Dumonceau JM, Frossard JL, Forget J, Morel P, et al. Association between lymphoepithelial cysts of the pancreas and HIV infection. Pancreatology 2012; 12:61–64. [PMID: 22487477]
- Fitko R, Kampmeier PA, Batti FH, Benjoya RA, Rao SM. Lymphoepithelial cyst of the pancreas with sebaceous differentiation. Int J Pancreatol 1994; 15:145–147. [PMID: 8071572]
- Fujiwara H, Kohno N, Nakaya S, Ishikawa Y. Lymphoepithelial cyst of the pancreas with sebaceous differentiation. J Gastroenterol 2000; 35:396–401. [PMID: 10832677]
- Worrall NK, Drebin JA. Pancreaticoduodenectomy for lymphoepithelial cyst of the pancreas. Am Surg 2000; 66:732–734. [PMID: 10966028]
- Younus S, Bleibel W, Bleibel H, Hernady N. Lymphoepithelial cyst of the pancreas. Dig Dis Sci 2007; 52:3136–3139. [PMID: 17909972]
- Arai T, Kino I, Nakamura S, Ogawa H. Epidermal inclusion in abdominal lymph nodes. Acta Pathol Jpn 1992; 42:126–129. [PMID: 1561883]
- Sako S, Isozaki H, Hara H, Tsutsumi A, Tanigawa N. Cystic lymphoepithelial lesions of the pancreas and peripancreatic region: report of two cases. Surg Today 1999; 29:467–471. [PMID: 10333422]
- Capitanich P, Lovaldi ML,Medrano M, Malizia P, Herrara J,Celeste F et al. Lymphoepithelial cyst of the pancreas: a case report and review of the literature. J Gastrointest Surg 2004; 8:342–345. [PMID: 15019932]
- Schwarz RE, Weiss LM. Lymphoepithelial cyst of the pancreas. No evidence for Epstein-Barr virus-related pathogenesis. Int J Pancreatol 1999; 25:223–227. [PMID: 10453424]










