Keywords
Diabetes Mellitus; Exocrine Pancreatic Insufficiency; Pancreatic Function Tests; Pancreatitis, Acute Necrotizing; Quality of Life
Abbreviations
ANP: Acute necrotizing pancreatitis; AP: acute pancreatitis; DM: diabetes mellitus; GTT: glucose tolerance test; HOMA: homeostasis model of assessment; MODS: Marshall organ dysfunction system; SF-36: the Medical Outcomes Study – 36- item short form health survey; SOFA: Sequential Organ Failure Assessment
INTRODUCTION
Acute pancreatitis (AP) is a common disease, with annual incidence in Brazil ranging from 15 to 20 cases for 100,000 population [1]. Fortunately, the vast majority of patients presents with mild AP, and undergo complete recovery without specific treatment. However, 20% of episodes are moderate or severe, with higher mortality (10-25%) and include the presence of local complications, such as pancreatic necrosis [2, 3].
Late consequences of acute necrotizing pancreatitis (ANP) have received less attention, since most of the studies lay emphasis on pathogenesis, management, immediate complications, prognostic criteria and experimental models. Nowadays, it is still controversial whether the pancreas fully recovers itself after an episode of AP. It is possible that scar tissue may remain as a consequence of the acute attack, especially if there was pancreatic necrosis or severe inflammation.
The presence of late endocrine and exocrine pancreatic dysfunction following ANP is uncertain, with current report ranging from 10% to 80% [4-19]. Similarly, there are controversies about how prior episodes of ANP may affect long-term wellbeing, leading to impairment in patients’ quality of life (QoL) [20-25]. These conflicting aspects are consequence of different patients with distinct treatment, since studies evaluate both mild and severe cases of AP, as well as using different methods to define pancreatic dysfunction.
Thus, there is discordant information on long-term outcomes of patients with ANP. Hence, this study was proposed to assess long-term exocrine and endocrine pancreatic function, pancreatic morphology and patients’ QoL, after a single episode of ANP.
METHODS
Patients
From January 2002 to April 2012, patients admitted to emergency unit of Santa Casa school of medicine in São Paulo, and diagnosed with AP had their hospitalization data reviewed. There were 530 admissions, of whom 49 (9.2%) cases had pancreatic necrosis and their overall mortality was 22% (11/49).
The diagnosis of AP was made when matched at least two of the following criteria: typical clinical presentation; serum amylase and/or lipase greater than three times the upper limit of normality; radiological features observed on computed tomography (CT) of the abdomen [26].
CT scan was indicated preferably 72 hours after the onset of symptoms and performed in the following situations: abdominal distension or intense abdominal pain; prognostic scores (APACHE II ≥ 8, SOFA ≥ 3 or MODS ≥ 2); C reactive protein above 150 mg/L; non-acceptance of the diet; lack of clinical improvement or evident worsening; and diagnostic uncertainty. CT scans were evaluated according to the Balthazar-Ranson Classification [27, 28]. Pancreatic necrosis was characterized on CT when there was a focal or diffuse hypoperfused glandular tissue, after the use of intravenous iodinated contrast. All patients underwent abdominal ultrasonography in the search of biliary etiology.
Patients who fulfilled the following criteria were included: One single episode of ANP and age between 18 and 70 years. The exclusion criteria were: clinically uncompensated comorbidities, such as congestive heart failure (functional class III/IV of the New York Heart Association), chronic renal failure on dialysis, chronic obstructive pulmonary disease on home oxygen therapy or any disabling physical illness; malignant neoplasm of any organ; illiteracy.
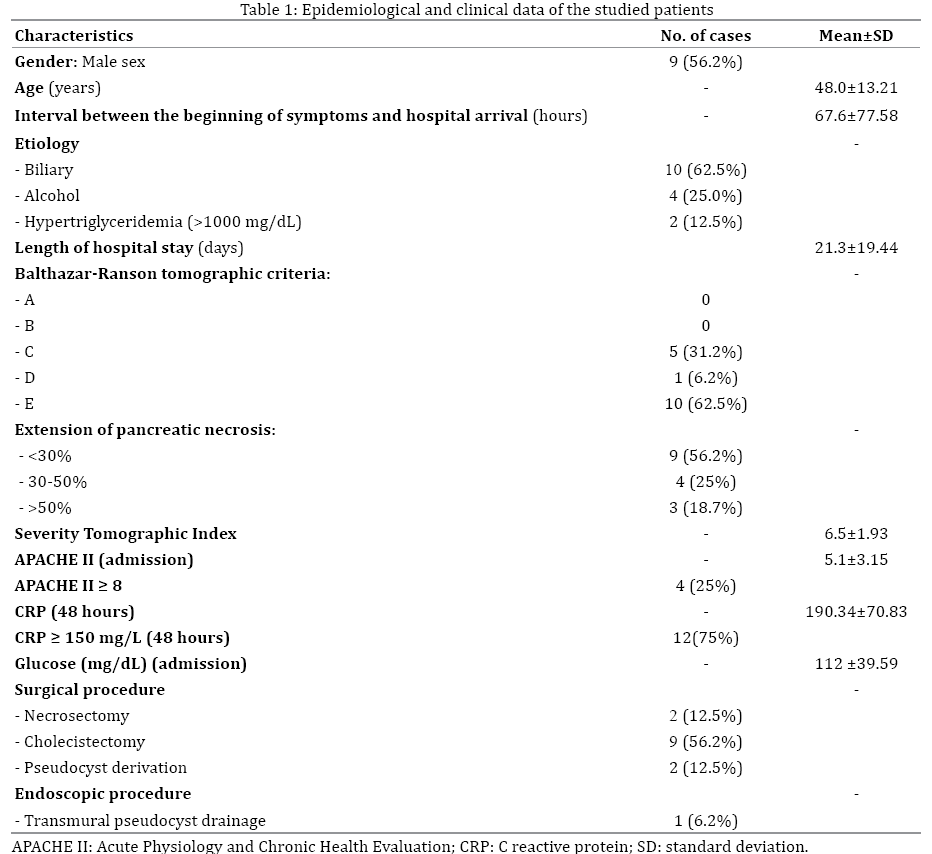
Four patients were excluded (one had intestinal carcinoma and three were older than 85 years), four were not located by telephone or letter, one has died of other causes, 13 were contacted and did not attend. Thus, 16 patients were enrolled in the study and had their medical records reviewed, allowing the description of clinical, demographic, therapeutic and prognostic data (Table 1).
We performed various tests at least 12 months after resolution of ANP. The mean interval between the diagnosis and the study was 2.9 years (range 12 to 90 months). All tests were performed within an interval of 15 days.
No patient was diagnosed with diabetes or pre-diabetes when hospitalized for ANP or was receiving pancreatic enzymes supplementation or insulin therapy at the time of the study.
Exocrine Pancreatic Function
Exocrine function was studied through qualitative fecal fat excretion (Sudan stain). Qualitative fecal fat was considered normal when negative; positive results demonstrated disabsorption.
Endocrine Pancreatic Function
Endocrine function was evaluated by a 2 hours, 75g, glucose tolerance test (GTT), C-peptide and HOMA (homeostasis model assessment).
GTT results were stratified according to the recommendations of the American Diabetes Association (normal: fasting 70-99 mg/dL, 120 minutes < 139 mg/dL; prediabetes: fasting 100-125 mg/dL, 120 minutes 140- 199 mg/dL; diabetes mellitus (DM): fasting: ≥ 126 mg/dL, 120 minutes ≥ 200 mg/dL [29].
HOMA-IR (insulin resistance) and HOMA-beta (beta cell function) were calculated through the following mathematical formulas (to obtain glucose in mmol/L, the result in mg/dL was multiplied by 0.0555): HOMA-IR = fasting insulin (μU/mL) x fasting plasma glucose (mmol/L) / 22.5; HOMA-beta = 20 x fasting insulin (μU/mL) / fasting plasma glucose (mmol/L) – 3.5 [30].
Measurements of C-peptide and HOMA index calculation allow discrimination between beta-cell dysfunction and insulin resistance. Low C-peptide levels (normal levels >0.9 ng/mL) and low HOMAbeta (150-175) indicates failure of pancreatic beta cells, suggesting endocrine pancreatic failure, while high levels HOMA-IR (>3.0) propose insulin resistance [31, 32].
Therefore, endocrine pancreatic insufficiency was defined in this study as hyperglycemic status (prediabetes or DM), associated with decreased HOMA-beta (<150) and/or low C-peptide (<0.9 ng/mL).
Morphology
Pancreatic morphology was examined by contrastenhanced abdominal CT. Reports were made by a single experienced radiologist who was blinded to the results of other tests. Morphological study searched for dysmorphic abnormalities of the pancreas: pancreatic edema, glandular atrophy, calcifications, pseudocysts, dilation of pancreatic duct and densification of peripancreatic fat.
Quality of Life
QoL was measured by the Medical Outcomes Study - 36- item short-form health survey (SF-36), which is a generic instrument, widely used in a large variety of medical conditions. It has been previously validated and culturally adapted for Portuguese speaking population in Brazil [33]. It consists of 36 questions that analyze physical and mental components in eight domains: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional and mental health. Eight results were obtained (one for each domain) and were compared to Brazilian sex- and age-matched normative data [34]. Patients answered the questionnaire through self-administration, in a special room at the hospital environment, supervised by a researcher who had no interference or influence in patients’ answers. The average length of response was 12 minutes.
STATISTICS
Data were reported as mean ± standard deviation, frequencies and interquartile range. To evaluate the association between endocrine dysfunction and the presence of morphological alterations with the extent of necrosis during ANP, Fisher's exact test was performed. QoL results were compared with normative data through interquartile range. Kruskal-Wallis test was applied to compare QoL between different etiologies of AP. Spearman's correlation analysis was used to verify the relationship of QoL with prognostic variables. A significance level of 5% (P<0.05) was adopted. Statistical analysis was performed by means of SPSS® version 21.0 software (Statistical Package for Social Sciences, Inc., Chicago, IL, USA).
ETHICS
This research was approved by the Committee on Research Ethics of the Surgery Department of the Santa Casa of São Paulo and was carried out according to the Helsinki Declaration of the World Medical Association. All patients signed the free informed consent form.
RESULTS
Only one patient (6.2%) showed signs of steatorrhea (positive result of Sudan stain). Four patients (25.0%) exhibited normal glucose levels and 12 subjects (75.0%) showed hyperglycemic status (43.7% had prediabetes and 31.3% were diabetic). Among those with impaired glucose profile, 8 patients demonstrated endocrine pancreatic insufficiency (50.0% of overall sample and 66.0% of those with abnormal glucose levels), all of whom showed HOMA-beta <90 and none with C-peptide below 0.9 ng/mL (Table 2). No statistically significant correlation was found between pancreatic endocrine dysfunction and the extent of necrosis during ANP (P=0.999).

Morphological pancreatic abnormalities were found in 62.5% (10 subjects): 31.2% had dilation of the pancreatic duct; 31.2% had glandular atrophy; 18.7% had pseudocysts; 18.7% had densification of peripancreatic fat; 12.5% had calcifications. There was a statistically significant association between the presence of morphological changes and the extent of necrosis during ANP (P=0.011). There were no cases of morphologically normal pancreas in patients with extensive necrosis (≥30%) during ANP.
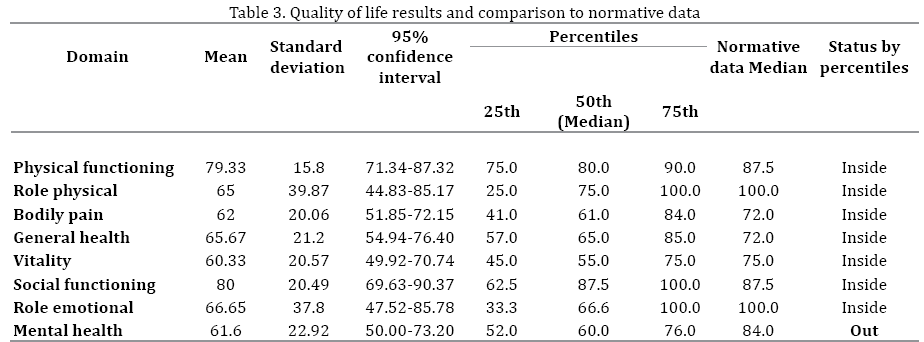
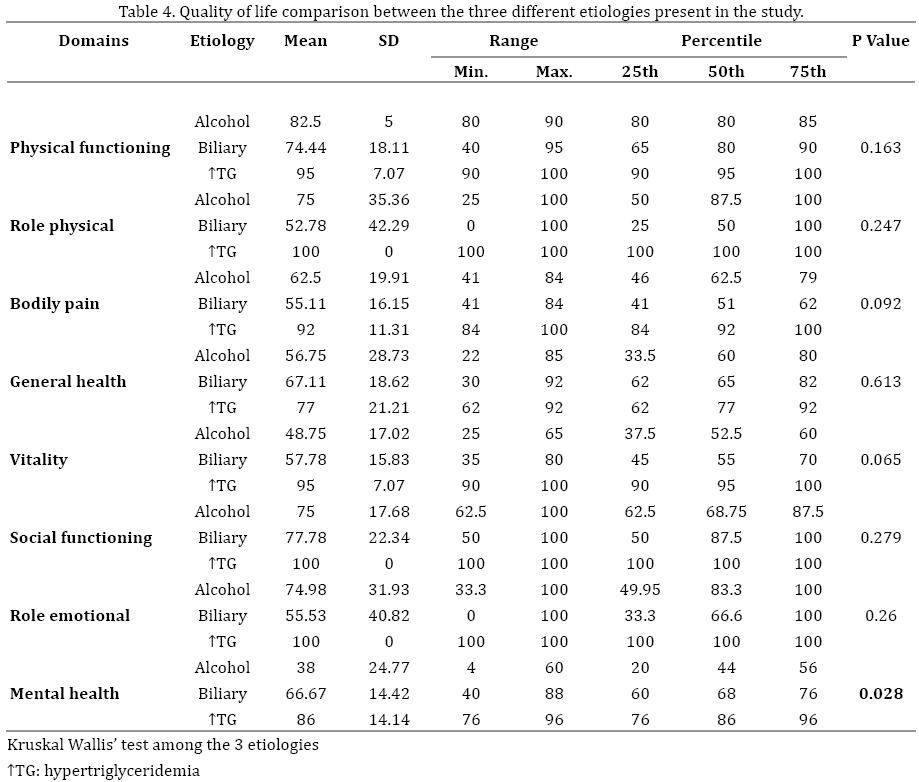
QoL results were expressed in Table 3, as well as comparison with healthy controls. Impairment was found exclusively in mental health domain. QoL was compared between the three etiologies of AP, revealing greater impairment of mental health domain in alcoholic etiology, followed by biliary and hypertriglyceridemia, with significant differences (P=0.028). There was no significant difference between the three etiologies in the remaining seven domains (Table 4). The analysis of the relationship between QoL and prognostic variables, such as extent of necrosis, C reactive protein and APACHE II demonstrated no significant association.
DISCUSSION
The vast majority of published researches on AP prioritize immediate aspects of the disease, complications, treatment aspects, prognostic criteria and experimental models. What happens after the climax of the inflammatory process and pancreatic necrosis is yet controversial.
Late-outcomes studies on AP attempt to determine whether there is impairment of pancreatic function and morphology and QoL of patients. There are controversies about the recovery of the pancreas and the possible impact on its function and morphology. It has been suggested that pancreatic function recovers completely after mild but not after severe AP [35]. The indiscriminate use of diagnostic tests and lack of systematization between the diagnosis of AP and studies can lead to different conclusions [4-17, 19]. Endocrine pancreatic dysfunction prevalence after AP can be improper if authors do not discern pancreatic (type 3c) and type 2 DM [5, 8, 14, 19]. QoL can be incorrectly interpreted when included elderly individuals, as results can be adversely affected by their limitations due to associated comorbidities [8, 20]. Some published series include both edematous and necrotizing AP, which can guide to erroneous interpretation [12, 13, 15]. Others assess individuals in recovery after surgical procedures performed during AP (i.e, necrosectomy) [10, 36]. However, some of them share the same limitation: small number of patients enrolled [8, 21].
Usually, most medical centers in our country do not perform a long-term follow-up of patients with AP. Thus, patients had to be reconvened, which lead to a considerable reduction of the number of subjects included. In the present study, many individuals that did not attend when summoned had prior alcoholic pancreatitis. Elevated proportions of those who consume alcohol in Brazil report a high risk pattern (abuse and dependence) that commonly reduces self-care and concerns with health and wellbeing, resulting in noncompliance [37].
It was chosen to investigate late effects of pancreatic necrosis and not late-outcomes of severe pancreatitis (which could have caused misinterpretation by including patients with edematous pancreatitis). Thus, only four patients had APACHE II ≥ 8. APACHE II can overstate the severity of the disease, especially in patients over 65 years old; likewise, it is known that there is not always a correlation between local severity of AP and the presence of the organic failure [38]. Moreover, in the present series, 12.5% of subjects underwent necrosectomy, which could be a potential bias of this study. However, none of the patients who underwent necrosectomy revealed signs of exocrine or endocrine pancreatic insufficiency, and morphologically normal pancreas with only unspecific findings on CT (mild thickening of anterior pararenal fascia and perigastric collaterals in a patient who presented with splenic vein thrombosis during ANP).
Only one patient (6.2%) had steatorrhea, suggesting exocrine pancreatic insufficiency. This low prevalence can be explained by the large pancreatic functional reserve (where there is evidence of malabsorption only when pancreatic enzyme secretion decreases to less than 10% of normal) and the low sensitivity of this indirect method for detecting mild to moderate exocrine pancreatic failure, diagnosing only severe dysfunction [39].
Unfortunately, despite the fact that our institution is a public reference center for treatment of AP in a developing country, we face financial difficulties which prevented the use of more specific tests for pancreatic exocrine function. Similarly, previous studies described no significant exocrine pancreatic dysfunction after AP, although the some of the tests used have low specificity (serum vitamins A and E) and limited sensitivity for mild dysfunction (fecal elastase-1) [5, 6, 7, 40]. Furthermore, Uomo et al. did not find significant signs of steatorrhea in a long follow up period, and also suggested an initial transient period of exocrine insufficiency [14]. This may imply that our patients might have shown improvement in exocrine function by the time of the research performance, carried out at least twelve months after ANP.
With regard to the endocrine function, some studies evaluated it based only on the values of fasting glucose and GTT, and did not prove that endocrine dysfunction is a direct consequence of diminished insulin secretion by pancreatic beta cells [5, 8, 14, 19]. Changes in glucose metabolism may have different pathophysiological mechanisms, such as insulin resistance and pancreatic failure. And these aspects should be valued due to the growing obesity epidemic, which can increase insulin resistance and prevalence of metabolic syndrome. Thus, to define the mechanisms involved in the hyperglycemia, it was chosen to conduct the investigation through GTT, C-peptide and HOMA-beta. Similar methodology has previously been applied by Andersson et al. who showed a tendency of serum C-peptide to be lower in diabetic patients after severe AP as compared to mild AP. However, HOMA-beta was not taken into consideration [13]. The use of HOMA beta with C peptide is a very useful method employed to determine severity of relative beta cell function. This discrimination of endocrine parameters is strength in the present study, especially showing that major mechanism involved in glucose metabolism was insulin resistance and not primarily pancreatic failure.
Pancreatic DM (type 3c DM) is a clinically significant condition known to be underappreciated and misdiagnosed (mostly as type 2 DM) [41]. Studies regarding its prevalence hardly exist. In a report from Germany, type 3c DM accounted for approximately 9% of all diabetics and only half of the cases were classified correctly, suggesting underdiagnoses [42]. To our knowledge, pancreatic DM prevalence is not available for Brazilian population. The right classification of DM is important, as type 3c DM has a unique pattern of hormonal and metabolic characteristics, distinct from type 1 and type 2 DM. The predominant mechanism is insulin deficiency, but hyperglycemia is also a result of persistent hepatic glucose production. Hypoglycemia can be particularly problematic, due to enhanced peripheral insulin sensitivity and deficiency of pancreatic glucagon secretion. Its course can be affected by a high risk for the development of pancreatic carcinoma. Hence, its management has peculiar features. Insulin therapy should be cautious, in order to avoid iatrogenic hypoglycemia. This anti-diabetic treatment also increases the risk of developing pancreatic malignancy, like the use of sulfonylurea [43-45].
In the assessment of the glycemic profile, 75% of the total sample was diagnosed as pre-diabetic and diabetic. Of these, we diagnosed as pancreatic insufficient (type 3c DM) those who presented with low HOMA-beta: 66% of those which altered glucose levels or 50% of the total casuistry. But they still had some residual function, characterized by appropriate C-peptide. Furthermore, in the other 34% of the patients with elevated glucose levels, the major mechanism involved in glucose metabolism was insulin resistance, and not primary pancreatic failure. These patients developed type 2 DM, which can occur independently of their previous pancreatic disease.
The relationship between pancreatic endocrine dysfunction and the extent of necrosis has not been proved in this study. However, it is not possible to exclude this relationship due to the small number of subjects included. Vujasinovic et al. described the prevalence of both exocrine and endocrine insufficiency after AP (including all etiologies and severities) in the largest number of patients enrolled so far [19]. The interval between the attack and the study was 2.7 years, which is somewhat similar to the present study, and exocrine insufficiency was found in 21% of patients. We had lower prevalence of exocrine insufficiency probably because of the method applied in this study. On the contrary, endocrine insufficiency was revealed in 14% and type 3c DM was defined exclusively by GTT results [19]. In a recent meta-analysis, Das et al. learned that the prevalence of exocrine dysfunction after AP is lower than newly pre-diabetes and DM (29% and 43%, respectively) [46]. Nevertheless, it has been described that the prevalence of concomitant exocrine dysfunction in patients with DM decreases over time, suggesting that pancreatic exocrine function recovers with time [46]. Indeed, this may justify our final results (prevalence of exocrine and endocrine dysfunction, respectively, 6.2% and 50%).
Regarding pancreatic morphology, all of 37.5% who showed no late abnormality had necrosis < 30% during the ANP, most likely because the smallest area of the pancreas affected by ischemic tissue provides more appropriate recovery of the organ. The statistically significant relation found between the presence of late abnormalities and the extent of necrosis is relevant and should be highlighted: it suggests that in extensive necrosis settings, patients should be routinely assessed in search of morphological changes in order to initiate appropriate therapy promptly. We believe this practice should be stimulated even in nonalcoholic ANP cases, since 75% of the present data presented biliary or metabolic etiology. The presence of pancreatic calcifications had a direct relationship with alcoholic etiology, and there was no association with the extent of necrosis. Reszetow et al. had described similar data, which may favor the hypothesis that alcoholic AP can be actually an episode of exacerbation of a subclinical chronic pancreatitis [11].
In the evaluation of QoL, SF-36 was chosen because it was validated for the Brazilian population, and has good responsiveness and degree of discernment [33]. Evidently, no data regarding QoL prior to the episode of ANP is available to allow confrontations, so we compared to normative scores [34], procedure that has formerly been adopted by other authors [8, 11, 13, 20, 21, 23]. QoL was preserved in seven of the eight domains studied by the SF- 36 (physical functioning, role physical, bodily pain, general health, vitality, social functioning and role emotional), showing that, in general, there was no impairment of QoL in patients with prior ANP. When an individual experiences a serious illness, with real perception of threat to his life, he can change his thoughts about what it is really important in the life, which may explain the favorable results obtained, despite possible adversities in daily life [20]. In addition, patients can change their concepts about life, adapting themselves to their symptoms and limitations.
Mental health domain was the only impaired domain. As a generic instrument was used, there might have been biases, such as environmental factors and stressful life events. The study involved the participation of chronic alcoholics, which may also be the one responsible for the impairment in mental health domain. It is well established co-occurrence of psychoactive substances dependence and mental health disorders such as depression and anxiety. There is evidence that even infrequent use of small doses of drugs can cause more serious consequences and are associated to more negative effects on mental health [47]. This hypothesis is supported by the difference found in the mental health domain between the three etiologies included in the study, with more evident prejudice among patients who had alcoholic ANP. There was no significant association between QoL and extent of necrosis, C reactive protein and APACHE II presented during ANP, suggesting that although suitable for predicting the severity of the disease, they were not related to long-term QoL outcomes.
Pendharkar et al., in a recent systematic review and metaanalysis, revealed impairment exclusively in general health (by 11%) and vitality (by 5%) domains in patients after AP [25]. Likewise, in our research vitality domain showed a tendency to be impaired. But the Australian group described limitations: all included studies were observational; QoL was assessed by different questionnaires as a “diseasespecific” is not yet available; various follow-up periods and the broad age range of patients included, as elderly population might have restrictions affecting baseline QoL. We also faced these limitations, except the age inconvenience as we excluded patients older than 70 years old to avoid bias in our results. Advanced age alone may affect baseline QoL by way of compounding comorbidities. Moreover, it has been previously described that geriatric population might have limitations in basic activities of daily living, and these aspects could lead to impairment in QoL, especially physical components. It is important to highlight that the three patients excluded according to our age criteria were older than 85 years old. Furthermore, one of the parameters studied in our manuscript was pancreatic morphology through contrast-enhanced abdominal CT. Elderly patients have higher risk of developing contrastinduced nephropathy.
The two major limitations of this study were the low number of patients and the test performed to evaluate pancreatic exocrine function. A great problem in the studies of AP is the small number of patients with particular manifestations such as pancreatic necrosis. Thus, any statistic result should be observed with attention. The use of a more sensitive method for exocrine function evaluation, such as fecal elastase-1, would be more precise and accurate to appropriately evaluate the prevalence of exocrine insufficiency after ANP. Financial difficulties related to a developing country prevented the use of this test in most of patients. Moreover, there may have been an unplanned selection of patients. The ones included in the study could have been motivated, as they voluntarily attended when contacted. On the contrary, individuals who did not attend could feel well enough, judging they did not need health service assistance. There is no way to confirm or discard these associations.
CONCLUSION
In conclusion, this study shows that patients exhibit good pancreatic exocrine function and QoL in longterm outcomes. However, they should be followed up by prolonged period, due to the risk of untreated DM as endocrine pancreatic function may be affected in 50% of cases. Special attention ought to be given to extensive necrosis, since morphology may be damaged. Although QoL is not compromised, measures to improve the patients’ mental health should be adopted, besides fighting alcoholism.
Conflict of Interest
Authors declare to have no conflict of interest.
References
- Rasslan S, de Campos T. Pancreatite Aguda. In: Pancreatite Aguda. 1st ed. São Paulo: Atheneu, 2013:1-6.
- Bradley EL III. A clinically based classification system for acute pancreatitis: Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga., September 11 through 13, 1992. Arch Surg 1993; 128: 596-90. [PMID: 8489394]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al., Classification of acute pancreatitis – 2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013; 62: 102-11. [PMID: 23100216]
- Migliori M, Pezzilli R, Tomassetti P, Gullo L. Exocrine pancreatic function after alcoholic or biliary acute pancreatitis. Pancreas 2004; 28: 359-63. [PMID: 15097850]
- Pelli H, Lappalainen-Lehto R, Piironen A, Järvinen S, Sand J, Nordback I. Pancreatic damage after the first episode of acute alcoholic pancreatitis and its association with the later recurrence rate. Pancreatology 2009; 9: 245-51. [PMID: 19407478]
- Pareja E, Artigues E, Aparisi L, Fabra R, Martínez V, Trullenque R. Exocrine pancreatic changes following acute attack of biliary pancreatitis. Pancreatology 2002; 2: 478-83. [PMID: 12378116]
- Ibars EP, Sanchéz de Rojas EA, Quereda LA, Ramis RF, Sanjuan VM, Peris RT. Pancreatic function after biliary acute pancreatitis: does it change? World J Surg 2002; 26: 479-86. [PMID: 11910484]
- Symersky T, van Hoorn B, Masclee AA. The outcome of a long-term follow-up of pancreatic function after recovery from acute pancreatitis. JOP 2006; 7: 447-53. [PMID: 16998241]
- Boreham B, Ammori BJ. A prospective evaluation of pancreatic exocrine function in patients with acute pancreatitis: correlation with extent of necrosis and pancreatic endocrine insufficiency. Pancreatology 2003; 3: 303-8. [PMID 12890992]
- Tsiotos GG, Luque-De Léon E, Sarr G. Long term outcome of necrotizing pancreatitis treated by necrosectomy. Br J Surg 1998; 85: 1650-53. [PMID: 9876068]
- Reszetow J, Hac S, Dobrowolski S, Stefaniak T, Wajda Z, Gruca Z et al. Biliary versus alcohol-related infected pancreatic necrosis similarities and differences in the follow-up. Pancreas 2007; 35: 267-72. [PMID: 17895849]
- Pezzilli R, Simoni P, Riccardo C, Morselli-Labate AM. Exocrine pancreatic function during the early recovery phase of acute pancreatitis. Hepatobiliary Pancreat Dis Int 2009; 8: 316-19. [PMID: 19502175]
- Andersson B, Pendse ML, Andersson R. Pancreatic function, quality of life and costs at long-term follow-up after acute pancreatitis. World J Gastroenterol 2010; 16: 4944-51. [PMID: 20954281]
- Uomo G, Gallucci F, Madrid E, Miraglia S, Manes G, Rabitti PS. Pancreatic functional impairment following acute necrotizing pancreatitis: Longterm outcome of a non-surgically treated series. Dig Liver Dis 2010; 42: 149-52. [PMID: 19836318]
- Yasuda T, Ueda T, Takeyama Y, Shinzeki M, Sawa H, Nakajima T et al. Long-term outcome of severe acute pancreatitis. J Hepatobiliary Pancreat Surg 2008; 15: 397-402. [PMID: 18670841]
- Pezzilli R, Morselli-Labate AM, Campana D, Casadei R, Brocchi E, Corinaldesi R. Evaluation of patient-reported outcome in subjects treated medically for acute pancreatitis: a follow-up study. Pancreatology 2009; 9: 375-82. [PMID: 19451747]
- Wu D, Xu Y, Zeng Y, Wang X. Endocrine pancreatic function changes after acute pancreatitis. Pancreas 2011; 40: 1006-11. [PMID: 21705952]
- Das SLM, Singh PP, Philips ARJ, Murphy R, Windsor JA, Petrov MS. Newly diagnosed diabetes mellitus after acute pancreatitis: a systematic review and meta-analysis. Gut 2014; 63: 818-31. [PMID: 23929695]
- Vujasinovic M, Tepes B, Makuc J, Rudolf S, Zaletel J, Vidmar T et al. Pancreatic exocrine insufficiency, diabetes mellitus and serum nutritional markers after acute pancreatitis. World J Gastroenterol 2014; 20: 18432- 38. [PMID: 25561813]
- Hochman D, Loule B, Bailey R. Determination of patient quality of life following severe acute pancreatitis. Can J Surg 2006; 49: 101-6. [PMID: 16630420]
- Bosscha K, Rejinders K, Jacobs MH, Post MW, Algra A, van der Werken C. Quality of life after severe bacterial peritonitis and infected necrotizing pancreatitis treated with open management of the abdomen and planned re-operations. Crit Care Med 2001; 29: 1539-43. [PMID: 11505122]
- Wright SE, Lochan R, Imrie K, Baker C, Nesbitt ID, Kilner AJ et al. Quality of life and functional outcome at 3, 6 and 12 months after acute necrotizing pancreatitis. Intensive Care Med 2009; 35: 1974-8. [PMID: 19685037]
- Broome AH, Eisen GM, Harland RC, Collins BH, Meyers WC, Pappas TN. Quality of life after treatment for pancreatitis. Ann Surg 1996; 223: 665-72. [PMID: 8645040]
- Soran A, Chelluri L, Lee KKW, Tisherman SA. Outcome and quality of life of patients with acute pancreatitis requiring intensive care. J Surg Res 2000; 91: 89-94. [PMID: 10816356]
- Pendharkar SA, Salt K, Plank LD, Windsor JA, Petrov MS. Quality of life after acute pancreatitis: A Systematic review and meta-analysis. Pancreas 2014; 43: 1194-1200. [PMID: 25333403]
- Tenner S, Baillie J, DeWitt J, Vege SS. American College of Gastroenterology Guideline: Management of acute pancreatitis. Am J Gastroenterol 2013; 108: 1400-15. [PMID: 23896955]
- Balthazar EJ, Ranson JH, Naidich D, Megibow AJ, Caccavale R, Cooper MM. Acute pancreatitis: prognostic value of CT. Radiology 1985; 156: 767-72. [PMID: 4023241]
- Balthazar EJ, Robinson DL, Megibow AJ, Ranson JH. Acute pancreatitis: value of CT in establishing prognosis. Radiology 1990; 174: 331-6. [PMID: 2296641]
- American Diabetes Association. Diagnosis and classification of Diabetes Mellitus. Diabetes Care 2013; 36: S67-74. [PMID: 23264425]
- Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis Model Assessment: insulin resistance and betacell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985; 28: 412-19. [PMID: 3899825]
- Buse JB, Polonsky KS, Burant CF. Disorders of carbohydrates and metabolism. In: Melmed: Williams Textbook of Endocrinology. 12th ed. Philadelphia: Elsevier, 2011: 1371-435.
- Wallace TM, Levy JC, Matthews DR. Use and abuse of HOMA Modeling. Diabetes Care 2004; 27: 1487-95. [PMID: 15161807]
- Ciconelli RM, Ferraz MB, Santos W, Meinão I, Quaresma MR. Traduçãopara a línguaportuguesa e validação do questionáriogenérico de avaliação de qualidade de vida SF-36 (Brasil SF-36). Rev Bras Reumatol 1999; 39: 143-50.
- Cruz LN, Fleck MPA, Oliveira MR, Camey SA, Hoffmann JF, Bagattini AM et al. Health-related quality of life in Brazil: Normative data for the SF-36 in a general population sample in the south of the country. Ciênc Saúde Colet 2013; 18: 1911-21. [PMID: 23827895]
- Aoun E, Slivka A, Papachristou DJ, Gleeson FC, Whitcomb DC, Papachristou GJ. Rapid evolution from the first episode of acute pancreatitis to chronic pancreatitis in human subjects. JOP 2007; 8: 573- 78. [PMID: 17873461]
- Connor S, Alexakis N, Raraty MG, Ghaneh P, Evans J, Hughes M et al. Early and late complications after pancreatic necrosectomy. Surgery 2005; 137: 499-505. [PMID: 15855920]
- Laranjeira R, Pinsky I, Sanches M, Zaleski M, Caetano R. Alcohol abuse patterns among Brazilian adults. Rev Bras Psiquiatr 2010; 32: 231-41. [PMID: 19918673]
- de Campos T, Cerqueira C, Kuryura L, Parreira JG, Soldá S, Perlingeiro JAG et al. Morbimortality Indicators in Severe Acute Pancreatitis. JOP 2008; 9: 690-97. [PMID: 18981549]
- Forsmark CE. Chronic pancreatitis. In: Feldman: Sleisenger and Fordtran’s. Gastrointestinal and Liver Diseases: Pathophysiology, Diagnosis, Management. 9th ed. Philadelphia: Elsevier, 2010: 985-1015.
- Naruse S, Ishiguro H, Ko SB, Yoshikawa T, Yamamoto T, Yamamoto A et al. Fecal pancreatic elastase: A reproducible marker for severe exocrine pancreatic insufficiency. J Gastroenterol 2006; 41: 901-8. [PMID: 17048055]
- Ewald N, Bretzel RG. Diabetes mellitus secondary to pancreatic diseases (type 3c) – are we neglecting an important disease? Eur J Intern Med 2013; 24: 203-06. [PMID: 23375619]
- Ewald N, Kaufman C, Raspe A, Kloer HU, Bretzel RG, Hardt PD. Prevalence of diabetes mellitus secondary to pancreatic diseases (type 3c). Diabetes Metab Res Rev 2012; 28: 338-342. [PMID: 22121010]
- Cui YF, Andersen DK. Pancreatogenic diabetes: special considerations for management. Pancreatology 2011; 11: 279-94. [PMID: 21757968]
- Ewald N, Hardt PD. Diagnosis and treatment of diabetes mellitus in chronic pancreatitis. World J Gastroenterol 2013; 19: 7276-81. [PMID: 24259958]
- Andersen D. The practical importance of recognizing pancreatogenic or type 3c diabetes. Diabetes Metab Res Rev 2012; 28: 326-28. [PMID: 22279014]
- Das SLM, Kennedy JIC, Murphy R, Phillips ARJ, Windsor JA, Petrov MS. Relationship between the exocrine and endocrine pancreas after acute pancreatitis. World J Gastroenterol 2014; 20: 17196-205. [PMID: 25493036]
- Kessler RC, Nelson CB, McGonagle KA, Edlund MJ, Frank RG, Leaf PJ. The epidemiology of co-occurring addictive and mental disorders: implications for prevention and service utilization. Am J Orthopsychiatry 1996; 66: 17-31. [PMID: 8720638]

