Eric M Nelsen1, Jeffrey Hubers2, Patrick R Pfau1, Deepak V Gopal1, Mark E Benson1
1Division of Gastroenterology and Hepatology, University of Wisconsin, Madison, Wisconsin
2Department of Internal Medicine University of Wisconsin, Madison, WI
*Corresponding Author:
Eric M Nelsen
Division of Gastroenterology & Hepatology
University of Wisconsin – School of Medicine & Public Health
4th Floor UWMF Centennial Building
Madison, WI; USA
Phone: +608 263-7322/608 265-5677
E-mail: enelsen@uwhealth.org
Received December 25th, 2015-Accepted February 5th, 2016
Keywords
Adenocarcinoma; cytology; Endoscopic ultrasound guided - fine needle aspiration; Pancreas
Abbrevations
EUS-FNA endoscopic ultrasound guided - fine needle aspiration
INTRODUCTION
Pancreatic adenocarcinoma remains a leading cause of cancer death in the United States with a low 5-year survival [1]. Diagnosing pancreatic adenocarcinoma is an evolving field with growth of Endoscopic ultrasound - Fine Needle Aspiration (EUS-FNA). EUS-FNA is highly sensitive and specific for pancreatic masses, with sensitivities as high as 80-95% and specificity in the range of 75-100% [2-5]. Tissue diagnosis of pancreatic masses is a growing area of research; providers are obtaining tissue diagnosis prior to surgery for pancreatic masses, especially when clinical diagnosis is not obvious or when neoadjunctive therapy is being considered. Indeterminate (atypical or suspicious) cytology results are not uncommon in EUS-FNA and can have a significant impact on the sensitivity of EUS-FNA, with one meta-analysis showing if indeterminate categories are included as a positive diagnosis, sensitivity increased from 85% to 94% [6]. Atypical and suspicious categories do not have standard diagnostic criteria and often vary depending on pathologist interpretation. These indeterminate categories create a dilemma for practitioners creating management plans for patients.
Studies have shown wide variance in how often these indeterminate diagnoses are used. One of the larger studies of EUS-FNA for pancreatic masses showed a rate of 6% of atypical and 5% suspicious [5]. On the other hand, a large meta-analysis of 12 studies found a wide range of use of the atypical category ranging from 1% to 14%; this study reported a risk of malignancy of 25% to 100% (mean: 58%; 95% confidence interval, 47%-69). However, these authors did not demonstrate how this risk of malignancy was calculated [7]. Few reports have assessed the true risk of malignancy for indeterminate categories. Recently four institutes examined this issue and found a wide range of indeterminate categories (both atypical and suspicious) among institutes ranging from 8.7-17.9%. This study found that the combined risk of subsequent malignancy was high for both atypical and suspicious categories (79% and 96 %, respectively) [8]. The aim of our study was to determine the long term follow-up and risk of malignancy in patients with atypical or suspicious cytology from pancreatic masses at a single academic tertiary referral center.
METHODS
1215 consecutive inpatient and outpatient EUS-FNAs performed at a single academic tertiary care center from 10/21/2009-12/31/2013 were reviewed. Final cytology from each case was reviewed and recorded by two researchers (EMN, JH). Patients with solid pancreas mass lesions who had “suspicious” or “atypical” final cytology were identified for further review of their clinical outcomes. Rapid onsite cytology evaluation was used in all cases. Individual data from each case was then recorded including patient age, mass size, number of FNA passes, clinical follow-up and any interventions/biopsies performed after index EUS-FNA. Final risk of malignancy was confirmed based on surgical pathology, positive pathology on repeat EUS or a clear clinical diagnosis of malignancy (based on mass characteristics, elevated CA 19-9 and rapid progression of tumor).
Comparison of the risk of malignancy between the atypical and suspicious groups were made using Pearson’s chi square statistic. A p-value of less than 0.05 was considered significant. Relative risk of malignancy was calculated comparing the risk of suspicious to that of atypical.
Risk of having a subsequent diagnosis of malignancy was the primary end point for each group. Secondary end point was relative risk of suspicious cytology as compared to atypical.
RESULTS
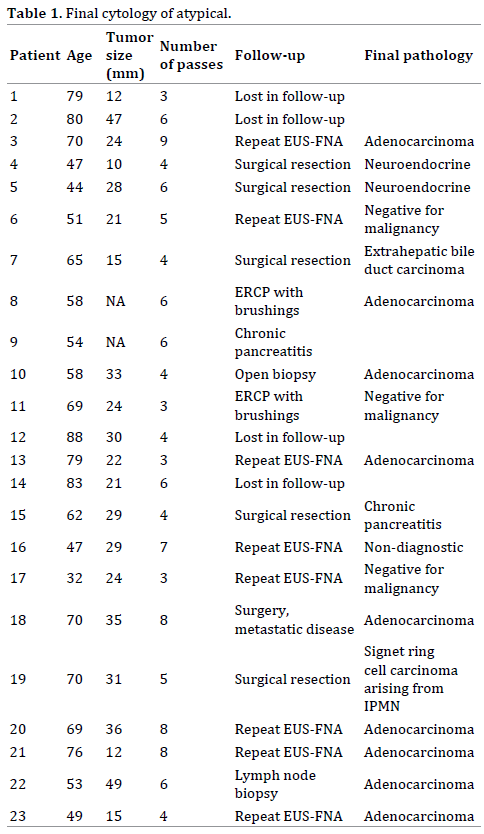
Of the 1215 patients with pancreas mass lesions, 45 (3.7%) were given an indeterminate cytologic diagnosis with 23 atypical and 22 suspicious for malignancy. Of the 23 patients with atypical cytology, 4 were lost to follow up after the index procedure. Of the remaining 19 patients with atypical cytology, 13 (68%) had subsequent diagnosis of malignancy. In the negative group, one patient was given a clinical diagnosis of chronic pancreatitis, one had a non-diagnostic repeat study, one had a surgical resection with benign pathology results and 3 patients had repeat EUS-FNA that was negative for malignancy. Eight of the 9 patients who underwent surgical resection in the atypical group had a diagnosis of malignancy. The one benign case undergoing surgical resection showed a final pathology of chronic pancreatitis. Average number of FNA passes in this group was 5.3 (Table 1).
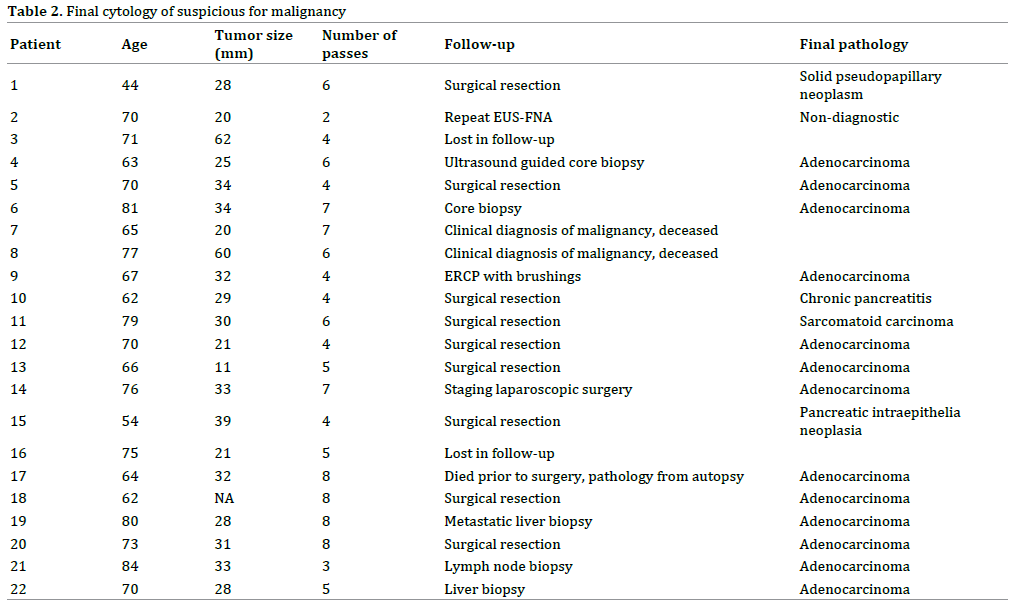
In the group of patients with suspicious cytology, 2 were lost to follow-up. Of the 20 patients with follow-up, 18 (90%) had a subsequent diagnosis of malignancy. Two of the cases of malignancy were clinical diagnosis (both patients died within months of index procedure). The two benign cases were chronic pancreatitis and one intraductal mucinous neoplasm. Eight of the 9 patients with suspicious cytology who underwent surgical resection had a diagnosis of malignancy. The one benign surgical resection was the patient with chronic pancreatitis. Average number of FNA passes in this group was 5.5 (Table 2).
Risk of subsequent malignancy was higher in the suspicious group than the atypical group; however, this was not significant (p=0.06) (Figure 1). The relative risk of malignancy for the suspicious group when compared to the atypical group is 1.31 (95% CI: 0.9375 to 1.8455).
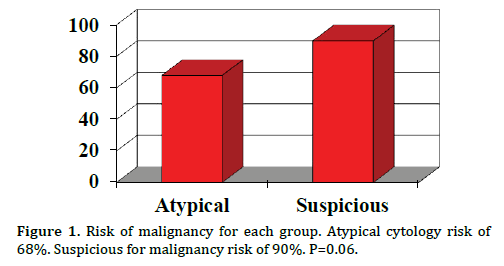
Figure 1. Risk of malignancy for each group. Atypical cytology risk of 68%. Suspicious for malignancy risk of 90%. P=0.06.
DISCUSSION
EUS-FNA has become the biopsy method of choice for pancreatic masses with high sensitivities and specificities [2-4]. Indeterminate categories of “atypical” and “suspicious” create a clinical dilemma for practitioners as a management plans are difficult to create with this level of ambiguity in the diagnosis of malignancy. Cytologists often use these indeterminate categories to reflect their level of uncertainty in diagnosis. These indeterminate categories may be helpful as they raise the likelihood that malignancy is present. Knowing the true risk of malignancy for these categories would be highly valuable for providers performing such procedures as it would guide the level of follow-up needed. Previous studies have shown a large range in use of these indeterminate categories among institutions, which likely correlates with a large range in the true risk of malignancy as each cytologist would have variability in what is atypical or suspicious [8]. Interestingly, Savides et al. found that institutes with lower rates of ‘‘positive for diagnostic yield’’ had higher rates of suspicious or atypical cytology [5]. This shows that certain cytologists are more likely to use indeterminate categories rather than labeling cytology positive for malignancy. Additionally it is possible that a sample labeled as atypical or suspicious by one pathologist may be read as positive for malignancy by another. Generally atypical cytology in the pancreas can be seen from of the following conditions: reactive changes, cytologic preparation artifacts, chronic pancreatitis, stent effect, and uncommon malignant neoplasms [7]. Atypical cytology is not unique to the pancreas, thyroid FNA samples are also commonly given atypical cytology results with ranges from 6-12%, however in these samples, atypical cytology is often more likely from benign lesions [9-11].
When compared to prior studies, our study had a much lower number of indeterminate category pathology at 3.7% [5, 8]. This strengthens the argument that pathologist effect the rate of indeterminate categories. At our institute, the risk of subsequent malignancy is high for both atypical and suspicious lesions (68% and 90 %, respectively). This high risk for future malignancy is similar to the prior study on this issue [8]. Given the high rate of subsequent malignancy in this study and previous studies of indeterminate cytology, repeat EUS-FNA would be advisable for patients with atypical or suspicious final cytology results. Based on our data, it would also be appropriate to refer patients with suspicious cytology results for surgical resection at our institute, given the exceedingly high risk of malignancy. Additionally, we have are working with our pathology department to implement an automatic second review by pathology when an indeterminate diagnosis is given. Currently our institute does not have access to any targeted gene studies to increase yield of diagnosis, this is a growing research area and its use in everyday practice may evolve in the future. Ultimately clinical interpretation with the combination of imaging, biomarkers and cytology results is superior to cytology results alone, thus clinical judgement remains of utmost importance. Using the combination of all modalities should limit the number of unnecessary procedures and surgeries for benign lesions.
Additionally, we found that EUS-FNA was more likely to be repeated in patients with atypical cytology. This is a sensible approach as the risk of malignancy appears to be slightly lower in this group when compared to suspicious although not significant. The percentages of patients who underwent a surgical operation were similar between in both categories. Only two patients in this entire cohort underwent surgical resections for benign disease, both were for chronic pancreatitis.
The limitations to this study are inherent to its retrospective nature. Our total number of indeterminate pathology was low, making it difficult to make broad conclusions; however, our data was collected from a large endoscopy database with all patients having long term follow-up to determine the true risk of subsequent malignancy. There were only few cases where patient follow-up was not known. Unlike other studies where electronic searches of cytology databases were used to find subjects, we individually searched each EUS-FNA endoscopy report to be sure all cases were included. Numbers of passes were similar between each group; given rapid onsite evaluation was used for both groups, number should not affect rate of how often an indeterminate diagnosis was made.
Given the wide range of rates atypical or suspicious cytology at institutes, it may be difficult to apply our results to other institutes. This study highlights the importance of internal reviews of indeterminate categories at endosonographers’ own institutes. Understanding how often these indeterminate cytology diagnoses are used at each institute performing these procedures and the true risk of malignancy is valuable information for providers. Further research is needed to know the true risk of malignancy in indeterminate cytology groups. However, based on the results of our study and other recent studies, the risk appears to be high. Lastly, further consensus guidelines are needed among pathologist to help uniform these indeterminate categories across institutions.
CONCLUSION
Risk of subsequent malignancy is high for both atypical and suspicious lesions. Repeat EUS-FNA should be considered for atypical cytology. Surgical resection of suspicious lesions may be warranted given the high risk for subsequent malignancy. Further research is needed to know the true risk of malignancy in indeterminate cytology groups.
Conflict of interest
The authors declare that there are no conflicts of interest.
References
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin 2009; 59: 225-49. [PMID: 19474385]
- Afify AM, al-Khafaji BM, Kim B, Scheiman JM. Endoscopic ultrasound-guided fine needle aspiration of the pancreas. Diagnostic utility and accuracy. Acta Cytol 2003; 47:341-8. [PMID: 12789912]
- Eloubeidi MA, Varadarajulu S, Desai S, Shirley R, Heslin MJ, Mehra M, Arnoletti JP,et al. A prospective evaluation of an algorithm incorporating routine preoperative endoscopic ultrasound-guided fine needle aspiration in suspected pancreatic cancer. J Gastrointest Surg 2007; 11:813-9. [PMID: 17440790]
- Turner BG, Cizginer S, Agarwal D, Yang J, Pitman MB, Brugge WR. Diagnosis of pancreatic neoplasia with EUS and FNA: a report of accuracy. Gastrointest Endosc 2010; 71:91-8. [PMID: 19846087]
- Savides TJ, Donohue M, Hunt G, Al-Haddad M, Aslanian H, Ben-Menachem T, Chen VK,et al. EUS-guided FNA diagnostic yield of malignancy in solid pancreatic masses: a benchmark for quality performance measurement. Gastrointest Endosc 2007; 66:277-82. [PMID: 17643700]
- Hewitt MJ, McPhail MJ, Possamai L, Dhar A, Vlavianos P, Monahan KJ. EUS-guided FNA for diagnosis of solid pancreatic neoplasms: a meta-analysis. Gastrointest Endosc 2012; 75:319-31. [PMID: 22248600]
- Abdelgawwad MS, Alston E, Eltoum IA. The frequency and cancer risk associated with the atypical cytologic diagnostic category in endoscopic ultrasound-guided fine-needle aspiration specimens of solid pancreatic lesions: a meta-analysis and argument for a Bethesda System for Reporting Cytopathology of the Pancreas. Cancer Cytopathol 2013; 121:620-8. [PMID: 23881871]
- Layfield LJ, Schmidt RL, Hirschowitz SL, Olson MT, Ali SZ, Dodd LL. Significance of the diagnostic categories "atypical" and "suspicious for malignancy" in the cytologic diagnosis of solid pancreatic masses. Diagn Cytopathol 2014; 42:292-6. [PMID: 24578254]
- Nayar R, Ivanovic M. The indeterminate thyroid fine-needle aspiration: experience from an academic center using terminology similar to that proposed in the 2007 National Cancer Institute Thyroid Fine Needle Aspiration State of the Science Conference. Cancer 2009; 117:195-202. [PMID: 19382174]
- Jo VY, Stelow EB, Dustin SM, Hanley KZ.Malignancy risk for fine-needle aspiration of thyroid lesions according to the bethesda system for reporting thyroid cytopathology. Am J Clin Pathol 2010; 134:450-6. [PMID: 20716802]
- Shi Y, Ding X, Klein M, Sugrue C, Matano S, Edelman M, Wasserman P. Thyroid fine-needle aspiration with atypia of undetermined significance: a necessary or optional category? Cancer 2009; 117:298-304. [PMID: 19711470]

