Keywords
Loneliness; Anxiety; Anxiety sensitivity; Avoidance
Introduction
Loneliness has been associated with a variety of clinical and social constructs including anxiety [1]; depression [2]; low self-esteem [3] and; low self-efficacy [4], among numerous others. The present study sought to deepen this understanding while simultaneously broadening the lens of loneliness research by adding Anxiety Sensitivity (AS) to the literature. Whilst a greater clinical focus has been highlighted in loneliness research [5], a broader social focus has been around AS research [6]. This study heeds to both of these calls by bridging the fields of loneliness and AS.
Concepts of Loneliness
According to human’s right from infancy [7], strive to maintain proximity to their primary caregiver and have a strong need to belong [8]. Unmet belongingness needs invariably result in such negative affectivity as depression, anxiety, and loneliness. Loneliness, then, is a universal experience [9] defined as an aversive state experienced when a deficit is perceived in one’s current relationships, as compared with one’s desired relationships [10]. It is also referred to as perceived social isolation [11] and associated with feeling of emptiness and rejection. Two main typologies for loneliness are suggested [12]: social isolation and emotional isolation.
Nevertheless, researchers are in agreement that loneliness entails a relationship deficit, characterized by negative affect [5]. Further it is significantly associated with greater sensitivity to 2 main emotions, sadness and fear such that the lonely are more vigilant toward facial cues related to negative emotions [13]. Cultural differences in the experience of loneliness have recently been found. For example, collectivist-oriented communities are more sensitive to social exclusion than individualistic communities [14]. Consistent with evolutionary research, [15] suggests that irrespective of age, the lonely are driven to connect with others, but in their endeavors to avoid socially threatening situations, they are more inclined to disengage from the self.
What is Anxiety Sensitivity?
Expectancy theory [16,17] suggests the motivation to avoid feared stimuli to be dependent on the interaction of two constructs: expectation and sensitivity; that is, fear entails an understanding of both what a person thinks will happen, and why they are afraid of this event. Individuals with low levels of AS are likely to consider the sensations associated with anxiety (increased respiration or rapid heartbeat) essentially harmless. However those who are high on AS are likely to consider these sensations as harmful [17]. Thus AS can be defined as the “fear of anxiety-related symptoms that results from belief that these symptoms have harmful somatic, social, or psychological consequences” [18]. Put simply, AS is the fear of fear [16]. Further AS, an established risk factor may lead to various forms of psychopathology. It has physical, social, and cognitive aspects, with indications that these components may have differential adverse outcomes [19].
AS has been shown to differ from trait anxiety both theoretically and empirically [20]. For example, trait anxiety is predictive of fearful responses to stressors [21], whereas AS is predictive specifically of fearful responses to the symptoms of anxiety; it is a better predictor of panic attacks than trait anxiety [22-24]; avoidance behaviours [25], including other psychopathologies [26]. Although trait anxiety and AS are inextricably correlated [17], the precise nature of this relationship is not yet established [27]. Therefore routinely controlling for trait anxiety in the measure of AS is recommended [28,29].
Loneliness and Anxiety Sensitivity
Early research posits loneliness as an important evolutionary construct. It is contended [12] that “loneliness…may once have contributed to the survival of the species”. Concurrent with attachment theory posits [7,12] loneliness as a drive to establish and conserve significant relationships. Hence loneliness can be seen as a useful emotion. According to [12], “the lonely are driven to find others”. This position supports observations [30] that lonely individuals are driven to overcome even severe anxiety in order to integrate socially. Subsequent research indicates that lonely individuals are more likely to avoid social interaction [5]. As compared with the nonlonely, lonely individuals are less sociable [3], identify few as their friends [11,31] and are less assertive [32]. Avoidance appears to be a common behavioural component of loneliness [5].
So, how is it that lonely individuals can be at once driven to find others, yet also likely to avoid interacting with others? AS may be useful in understanding this apparent behavioural anomaly of loneliness. For example, the more lonely were more cautious and distrustful of others and more likely to perceive threat in everyday life events than the less lonely [4]. Further threat perception linked with AS may be predictive of avoidant behaviour [33] and emotional avoidance [34]. It is stated elsewhere [3] that anxiety is a less important correlate of loneliness than emotional and behavioural disengagement. These findings support the case for a relationship between loneliness and AS. Further, [35] found that regardless of participants’ level of trait anxiety (low, moderate, or high), elevated AS was associated with higher behavioural avoidance. So, to find high AS among behaviourally avoidant, lonely individuals would be less surprising than to find high trait anxiety among the same group. Lonely individuals’ increased threat perception [4] may also be a function of AS. Further, participants’ Anxiety Sensitivity Index (ASI) scores predict threat-related cognitive biases [27].
Chronically lonely individuals recorded elevated mean salivary cortisol levels during the course of a day, indicating both an increased production of Corticotrophin-Releasing Hormone (CRH), and an increased activation of the Hypothalamic-Pituitary- Adrenocortical Axis (HPA) [3]. In other words, lonely individuals experienced stress in greater severity and frequency than the nonlonely and consistently recorded lower basal heart rates and heart rate reactivity than did normal or socially embedded across a range of tasks including social and non-social speeches [3]. Their inference that lonely individuals are socially and emotionally withdrawn is warranted. It seems reasonable to suggest that some lonely individuals may present with emotional and behavioural disengagement in an attempt to suppress physiological responses that they perceive as threatening. As such, lonely individuals should then endorse higher levels of AS than nonlonely. Such a possibility has been relatively unexplored in the literature.
Some light on avoidance associated with loneliness has been found. Utilising the four-category attachment typology [36,37] found a positive relationship between loneliness and fearful attachment; to a lesser degree, dismissing and preoccupied styles were also associated with loneliness. Further, [37] found a significantly high positive association between dismissing attachment and social loneliness. Similarly, a positive relationship between loneliness and insecure attachment is reported [38]. This is not surprising; indeed, anxiety is one of two primary dimensions (anxiety and avoidance) posited to underpin attachment [39]. More recently the role of attachment anxiety and avoidance has been highlighted [40] to affect loneliness. Recent findings [41] indicate that loneliness is experienced irrespective of age and that adolescents, who experience chronic loneliness, are more likely to report depression, deficits in social skills and tendency toward suicide.
So it appears that both AS [42] and loneliness [37] can entail a negative model of self and others, and may present with concurrent high or low trait anxiety. That the putative relationship between these two constructs remains under investigated constitutes a significant gap in the literature. However findings of an association between AS and avoidance [25,33,34], regardless of level of trait anxiety [35], suggest AS may provide further insights into loneliness beyond those provided by trait anxiety alone.
The present study aimed to explore (1) The relationship between loneliness and AS (2) Differences in trait anxiety, AS, and behavioural avoidance as a function of differential levels of loneliness. The following three hypotheses were tested:
First, it was predicted that the lonely would endorse higher levels of trait anxiety, AS, and avoidance than participants in normal or socially embedded group. Moreover, as trait anxiety, AS, and avoidance are related theoretically and empirically [16,17,26], their combined multivariate effect was expected to differentiate lonely participants from participants labeled either normal or socially embedded. Second, while trait anxiety is inextricably correlated with AS [20,28,29,43], it was anticipated that AS would predict differences in loneliness after controlling for trait anxiety as a covariate. Finally it was hypothesised that after controlling for trait anxiety and AS, avoidance would contribute uniquely to group differences such that the lonely group would endorse higher avoidance than the normal, and socially embedded groups. This study sought to test whether behavioural avoidance could predict significant differences between groups beyond those represented by trait anxiety and AS. Following recommendations [3], the normal group was included to investigate whether group differences varied monotonically between the socially embedded and lonely groups, or whether (as has been hypothesised) the greatest effects for AS and avoidance occurred at the pathological ends of their respective scales.
Method
Participants
The total sample comprised 506 first year undergraduate psychology students (108 males and 398 females) at a university in Sydney, Australia. As this study aimed at a non-clinical sample, participants currently seeking help for anxiety or depression related disorders were screened, reducing the sample by 5. Consistent with previous research [3], the 501 participants were further screened on their total scores on the R-UCLA scale such that participants scoring in the 1st (total score ≤ 28), 3rd (total score ≥ 33 and ≤ 39), and 5th (total score ≥ 46) quintiles were included. The final retained sample of 319 comprised 79 male (M=22.54 years, SD=7.22) and 240 female participants (M=21.04 years, SD=6.05). Though males were older than females, this difference was not significant, t (317)=1.96, p>0.05.
Design
The independent variable was level of loneliness operationalised as the 1st, 3rd, and 5th quintile of participants’ R-UCLA loneliness scale [44] scores, and respectively formed the socially embedded, normal, and lonely groups. The dependent variables were trait anxiety, AS, and behavioural avoidance. This study utilised a one-way multivariate analysis of variance conducted on the linear combination of all three dependent variables. The planned posthoc procedure was a Roy-Bargmann stepdown analysis [45]. The a priori order of dependent variables assigned first priority to trait anxiety, second to AS, and third priority to behavioural avoidance.
Materials
Revised UCLA loneliness scale
The revised UCLA loneliness scale [44] a precedent loneliness measure in the literature, comprises 20 statements (e.g., “I feel in tune with the people around me”) along with a four-point Likert scale ranging from 1 (never) to 4 (often). Half of the statements reflect satisfaction and the other half reflect dissatisfaction, with one’s social relationships. Total scores range between 20 to 80, higher scores denote greater levels of loneliness. The scale has a high internal consistency (α=0.94) and good test-retest reliability over a 12-month period (r=0.73) [44]. The R-UCLA total score was used to operationalise participants’ level of loneliness in the present study.
State-trait anxiety inventory
The Trait scale of the State-Trait Anxiety Inventory (STAI-T), [46] is a 20-item self-report measure that determines how anxious individuals “generally” feel on 4-point Likert scale ranging from 1 (almost never) to 4 (almost always). Trait anxiety scores span from 20 to 80 (higher scores indicate a higher level of trait anxiety). A good test-retest reliability for male (r=0.73) and female (r=0.77) college students over a 104-day interval and a high median Cronbach’s alpha coefficient (α=0.90) indicates excellent internal consistency [46].
Fear questionnaire
The Fear Questionnaire (FQ) [47] is a measure of phobic avoidance consisting of 15 situations, for example, traveling alone, large open spaces, talking to people in authority, an audience, and hospitals that can be rated from 0 (would not avoid it) to 8 (always avoid it). A total avoidance score ranges between 0 to 120; higher scores indicate greater avoidance. Test-retest reliability with phobic participants over a 7-day interval (r=0.82) is good [47]. Tests of internal consistency for the FQ subscales yielded coefficient alphas ranging from 0.57 to 0.70 [48].
Anxiety sensitivity index
The Anxiety Sensitivity Index (ASI) [49] comprises of 16 statements pertaining to beliefs that anxiety symptoms are signs of harmful or aversive consequences (e.g., “When I notice that my heart is beating rapidly, I worry that I might have a heart attack). Participants rate the extent to which they agree or disagree with each item on a five-point Likert scale ranging from 0 (very little) to 4 (very much). Total scores range between 0 to 64 (higher ASI scores indicate higher levels of AS). Pearson product-moment correlations for the ASI were found to (0.71; 0.75), reveal adequate test/retest reliability [49].
Procedure
This study was granted full ethics approval by the University Human Research Ethics Panel. Participants were recruited via an online invitation to participate in a study to determine the relationship between loneliness, AS and avoidance by completing an online survey comprising of five sections. Section-1 contained items regarding demographic information (e.g., age, gender, cultural background), as well as a screening item for participants currently seeking help for anxiety or depression related disorders. Sections 2, 3, 4, and 5, each consisted of one of the four inventories (R-UCLA, STAI-T, FQ, and ASI) which were ordered randomly for each participant by the online system to minimise the order effect. Electronic submission of the completed survey implied informed consent. All participants received course credit.
After screening for possible clinical disorders, R-UCLA scores for 501 were explored. The data were normally distributed; both males (M=39.02, SD=10.74) and females (M=37.56, SD=10.73) had scores similar to [44] for a normative university sample. No significant difference between male and female scores was found, t (499)=1.24, p>0.05. Following the precedent of previous studies [3,4], three groups were formed of participants scoring in the 1st (socially embedded), 3rd (normal) and 5th (lonely) quintiles of R-UCLA. As such, participants scoring in the 2nd and 4th quintiles of R-UCLA scores were excluded from the analysis.
Results
One-way between-subjects Multivariate Analysis of Variance (MANOVA) was conducted on three dependent variables: trait anxiety, anxiety sensitivity, and avoidance. The independent variable comprised three levels of loneliness: socially embedded, normal, and lonely. The analysis was conducted using SPSS MANOVA with the sequential adjustment for non-orthogonality.
The total number of participants (N=319) was reduced by 3 due to missing data. Following the recommendation of [50], a further 8 univariate outliers were deleted after various attempts at data transformation failed to achieve univariate normality; assumptions of normality were satisfactory. The final sample retained for analysis was N=308. No multivariate within-cell outliers were identified at p=0.001. Table 1 shows the pooled within-cell correlations for the ASI, STAI-T, and FQ; the logdeterminant was sufficiently different from zero indicating the absence of multicollinearity [50]. Bartlett’s test of sphericity was significant at p=0.01 indicating that all of the dependent variables were suitable for MANOVA. Level of significance was set at p=0.05 for all analyses (Table 1).
| |
ASI |
STAI-T |
FQ |
| ASI |
8.795a |
|
|
| STAI-T |
0.384 |
9.451a |
|
| FQ |
0.400 |
0.240 |
16.953a |
Note: N=308. ASI=Anxiety Sensitivity Index [49]; STAI-T=Spielberger Trait Anxiety Scale [46]; FQ=Fear Questionnaire [47]; a=Standard deviation.
Table 1: Pooled Within-cell Correlations for ASI, STAI-T, and FQ.
Pillai’s criterion indicated a significant effect for group, F(6,608)=33.88, p=0.000, on the linear combination of dependent variables. There was modest association between group scores and the combined dependent variables, partial η²=0.25. Univariate tests of between-subject effects yielded significant main effects for trait anxiety, F(2, 305)=141.13, p=0.000, partial η²=0.48, anxiety sensitivity, F(2, 305)=45.31, p=0.000, partial η²=0.23, and avoidance, F (2, 305)=28.31, p=0.000, partial η²=0.16.
Roy-Bargmann step-down analysis was conducted to investigate the nature of the multivariate main effect in terms of the individual dependent variables and was deemed sufficiently reliable to justify step-down analysis, and homogeneity of regression was achieved. In the step-down analysis, trait anxiety was given the highest priority, anxiety sensitivity was given second priority, and avoidance was given third priority. As such, trait anxiety was tested in a univariate ANOVA and then treated as the covariate in the analysis of anxiety sensitivity; following this, both trait anxiety and anxiety sensitivity were treated as covariates in the analysis of avoidance.
As already indicated by the univariate tests of between-subject effects following the MANOVA, a unique contribution to predicting group differences in level of loneliness was made by trait anxiety, stepdown F(2,305)=141.13, p=0.000, partial η²=0.48. Participants in the lonely group recorded higher STAI-T scores (M=52.00, SD=9.06) than did participants in the normal group (M=38.88, SD=9.43) who in turn recorded higher STAI-T scores than socially embedded participants (M=30.06, SD=7.56). After controlling for trait anxiety (i.e., entering it as a covariate) a unique contribution to predicting group differences in level of loneliness was made by anxiety sensitivity, stepdown F (2, 304)=3.47, p=0.032, partial η²=0.022 (Figure 1).
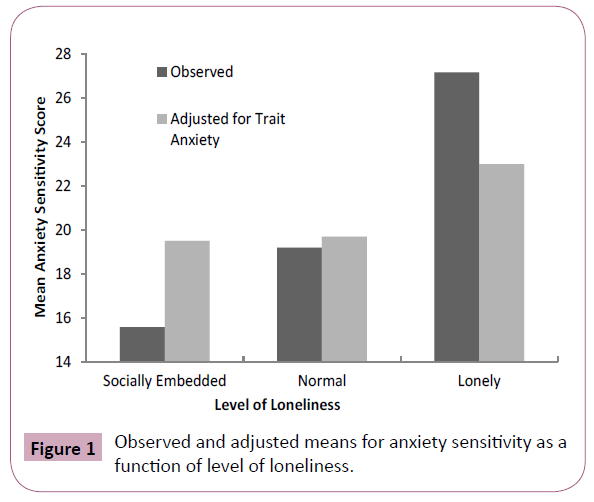
Figure 1: Observed and adjusted means for anxiety sensitivity as a function of level of loneliness.
Pairwise comparisons with a Bonferroni correction illuminated a significant difference in adjusted means for anxiety sensitivity between the normal (M=19.70, SE=0.81) and lonely (M=23.00, SE=0.99) groups (p=0.037). Figure 1 illustrates the observed and adjusted means for anxiety sensitivity. While a marginally greater difference in adjusted means for anxiety sensitivity can be seen between the socially embedded group (M=19.50, SE=0.94) and the lonely group, this difference was not significant at p=0.05 after a Bonferroni correction.
After the patterns of differences for trait anxiety as the first priority covariate, and anxiety sensitivity as the second priority covariate were entered, no unique contribution to predicting group differences in level of loneliness was made by avoidance, stepdown F(2,303)=1.87, p=0.156, partial η²=0.012. That is, although a univariate comparison with avoidance as the dependent variable and trait anxiety as a covariate revealed a significant difference between the socially embedded and lonely groups after a Bonferroni adjustment, univariate F (2,304)=3.36, this difference was already represented in the stepdown analysis by anxiety sensitivity. Figure 2 demonstrates that after controlling for both trait anxiety and anxiety sensitivity, the adjusted mean avoidance increased for the socially embedded and normal groups while simultaneously decreased for the lonely group. The pattern of mean avoidance with an adjustment for trait anxiety only (which was not part of the stepdown analysis) serves to demonstrate that anxiety sensitivity was most influential as a covariate of avoidance within the lonely group. Table 1 shows that anxiety sensitivity and avoidance were the most highly correlated (r=0.40) of the possible pairs of dependent variables in this study.
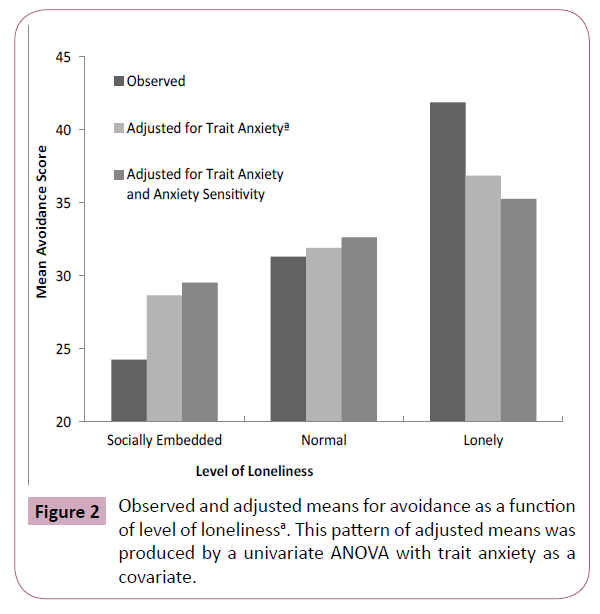
Figure 2: Observed and adjusted means for avoidance as a function of level of lonelinessa. This pattern of adjusted means was produced by a univariate ANOVA with trait anxiety as a covariate.
Discussion
The findings of the present study provide clear evidence of the relationship between AS and loneliness. As predicted, the lonely group endorsed significantly higher levels of AS than did either the normal or socially embedded groups. Moreover, the normal group endorsed significantly higher levels of AS than did the socially embedded group indicating that raw ASI scores varied monotonically between the three levels of loneliness. Even after controlling for trait anxiety, AS uniquely predicted differential levels of loneliness between the normal and lonely groups. Contrary to predictions, however, no significant difference was found between the socially embedded and lonely groups as a function of AS. While avoidance did reveal differences between the socially embedded and lonely groups after controlling for trait anxiety only, however contrary to predictions, avoidance did not account for a significant portion of group variance after controlling for both trait anxiety and AS. Nevertheless, these findings constitute an important contribution to both loneliness and AS literatures.
Consistent with previous research, trait anxiety was found to increase as a function of loneliness [3-5]. Findings suggest that lonely individuals may have an increased predisposition to react fearfully to the physiological symptoms of anxiety (as indicated by increased AS). Perhaps the most poignant implication of these findings is toward a clearer understanding of the psychophysiology of loneliness. It is reasoned that [3] behavioral and emotional disengagement from the social environment is more powerful than trait anxiety in lonely individuals. The present findings of increased AS among lonely individuals supports previous [3] conclusions, and also suggest a more parsimonious explanation: that lonely individuals may employ social and emotional disengagement as a strategy to suppress the physiological symptoms of anxiety triggered by social events. Further, while it is seemingly incongruent that lonely individuals can simultaneously experience greater levels of stress (as indicated by increased HPA activation) and lower physiological symptoms of stress [3,31] however, AS can account for increased stress [16,17] as well as the suppression of physiological symptoms [25].
The present findings of increased AS among lonely individuals also have cognitive implications beyond those of trait anxiety alone. it is suggested [3] that, “It is conceivable that, relative to nonlonely individuals, lonely individuals have, as a default, a threat appraisal regarding not active coping stressors but the very contexts of their lives”. However, the nature of such a threat appraisal is unclear. Some evidence suggests that AS is predictive specifically of threat-related cognitive biases [27]. Moreover, expectancy theory [16,17] of which AS is a component, posits that expected feared outcomes are avoided as a function of an individual’s level of sensitivity to such outcomes. Lonely individuals’ increased threat perception [3] may be a function of AS. The present findings suggest the possibility that lonely individuals simultaneously long to satisfy relationship deficits [5,8,10,12] and seek to avoid social and emotional engagement [3-5] as a result of higher than normative levels of AS.
The exploratory nature of the present study precludes the inference of a causal relationship between loneliness and AS. However, the influence of AS in the lonely group must not be underestimated. Mean ASI score for the lonely group is comparable to most clinical groups of social phobia patients [51]. It is probable that AS may function to motivate social avoidance in lonely individuals who are sensitive to physiological arousal associated specifically with social events, a proposed role of AS in social phobia patients [52]. The similarities in AS levels between the lonely group in the present study and those experiencing social phobia lends credence to the notion that lonely individuals may socially disengage as a strategy to avoid the physiological symptoms of anxiety triggered during social events. This finding is particularly important as the present sample was specifically non-clinical. Thus, this study demonstrates the need for further clinical attention in loneliness research [5], and greater social application of AS research [6].
Behavioural avoidance as measured by the FQ [47] could not predict group differences beyond those predicted respectively by trait anxiety and AS. The significant main effect for avoidance as part of the MANOVA analysis, coupled with the significant univariate ANOVA result for avoidance after controlling for trait anxiety, indicates a positive relationship between FQ and R-UCLA scores. This finding supports and extends literature, characterizing lonely individuals as socially [3]; emotionally [3,4], and interpersonally [37,38] avoidant, by adding a measure of behavioural avoidance (the FQ) relatively unexamined in the context of loneliness. Moreover, it is behavioural avoidance (as measured by the FQ) that appears to be most closely related to AS [25,34,35].
Second, Roy-Bargmann stepdown analysis is a much more conservative follow-up procedure to MANOVA than are separate univariate ANOVAs [53]. Separate ANOVAs would have yielded significant results for both AS and avoidance even after controlling for trait anxiety in the present study. However, as behavioural avoidance and AS are theoretically and empirically related [35], separate univariate ANOVAs may have yielded duplicate significance [50]. Hence, the more conservative procedure was used herein.
Finally, the inclusion of FQ data permitted to investigate whether avoidance accounted for some unique group difference not represented by AS. The contribution of AS can be seen as comprehensive insofar as, FQ scores could not illuminate further between-group differences. Interestingly, as a covariate, AS was most influential on the lonely group’s adjusted mean for avoidance. It may be that even though avoidance played some role in the multivariate effect of group differences for loneliness, AS had the preeminent effect within the lonely group. This is a question for further empirical study.
The finding of no significant differences in AS after controlling for trait anxiety between the socially embedded and lonely groups is somewhat unexpected. The markedly higher adjusted mean for AS in the socially embedded group reflects the concurrently low levels of trait anxiety. There are two possible explanations for this result. The practice of controlling for trait anxiety may in some cases obscure the true effects of AS [16]. Alternatively, this finding may reflect that AS seems to be most influential at pathological levels [19,26]. Further detailed investigation is needed to determine the role of AS in socially embedded individuals.
The recruitment of undergraduate students (Mean age=21.4 years) can be seen as a limitation of this study. While the prevalence of AS appears to be similar for younger and older adults [54], it has been reported to decrease from early development to old age [55]. Likewise, in the present study, variance in cell sizes prohibited the investigation of possible multivariate effects associated with gender. Male participants represented only 24.8% of the sample. While multivariate analyses of variance are robust to differences in cell size up to a ratio of 1:1.5 [50], to achieve this in the present study would have entailed the random deletion of 122 female participants from the study. Such a sacrifice was deemed unjustifiable.
The finding that lonely individuals may avoid social and emotional engagement partially due to an increased sensitivity to the Symptoms of Anxiety (AS) elicited specifically in a social context has several important implications. For example, that lonely individuals are driven to find others [12] integrate socially [30], and satisfy belongingness needs [8], but are simultaneously socially and emotionally avoidant [3,4,16], is rendered less paradoxical by the possibility that higher levels of AS may inhibit approach behaviours, precisely because of the physiological arousal of new social experiences. Put simply, while most people perceive the common feelings of nervousness in new social situations as essentially harmless, higher AS levels in lonely people may motivate avoidance of the very social and emotional engagement they long for. Further, the present study provides a more parsimonious explanation of findings that lonely individuals experience greater levels of stress [3,4] but lower physiological reactivity to stressors [3]. Indeed, AS predicts the avoidance of feared physiological sensations regardless of the level of concurrent trait anxiety [25,34,35].
This study has made an important contribution towards better understanding the relationship between loneliness and AS, as well as how this relationship might affect lonely individuals’ avoidance behaviours. Further a better understanding of individual and social factors in the emergence of loneliness is important [56]. Likewise, considering multidimensional models of loneliness in the context of AS and utilising an attachment framework may further illuminate the relationship between loneliness and AS. While the present study was exploratory in nature, it stresses a need for greater clinical focus in loneliness research [5] and broader social focus in AS research [6]; the posited relationship between loneliness and AS is promising.
References
- Mijuskovic B (1986) Loneliness, anxiety, hostility, and communication. Child Stud J 16: 227-240.
- Weeks DG, Michela JL, Peplau LA, Bragg ME (1980) Relation between loneliness and depression: a structural equation analysis. J Pers Soc Psychol 39: 1238-1244.
- Cacioppo JT, Ernst JM, Burleson MH, McClintock MK, Malarkey WB, et al. (2000) Lonely traits and concomitant physiological processes: the MacArthur social neuroscience studies. Int J Psychophysiol 35: 143-154.
- Hawkley LC, Burleson MH, Berntson GG, Cacioppo JT (2003) Loneliness in everyday life: cardiovascular activity, psychosocial context, and health behaviors. J Pers Soc Psychol 85: 105-120.
- Heinrich LM, Gullone E (2006) The clinical significance of loneliness: a literature review. Clin Psychol Rev 26: 695-718.
- Zvolensky MJ, Schmidt NB (2007) Introduction to anxiety sensitivity: recent findings and new directions. Behav Modif 31: 139-144.
- Bowlby J (1969) Attachment and loss. Attachment London (2nd Edn): The Hoggart Press, p: 425.
- Baumeister RF, Leary MR (1995) The need to belong: desire for interpersonal attachments as a fundamental human motivation. Psychol Bull 117: 497-529.
- Rotenberg KJ, Hymel S (1999) Loneliness in childhood and adolescence. Cambridge: Cambridge University Press.
- Peplau LA, Perlman D (1982) Loneliness: a sourcebook of current theory, research, and therapy. New York: John Wiley & Sons, p: 447.
- Cacioppo JT, Fowler JH, Christakis NA (2009) Alone in a crowd: the structure and spread of loneliness in a large social network. J Pers Soc Psychol 97: 977-991.
- https://mitpress.mit.edu/books/loneliness
- Vanhalst J, Gibb BE, Prinstein MJ (2015) Lonely adolescents exhibit heightened sensitivity for facial cues of emotion. Cogn Emot 31: 377-383.
- Lykes VA, Kemmelmeier M (2014) What predicts loneliness? Cultural difference between individualistic and collectivistic societies in Europe. J Cross Cult Psychol 45: 468-490.
- Qualter P, Vanhalst J, Harris R, Van Roekel E, Lodder G, et al. (2015) Loneliness across the life span. Perspect Psychol Sci 10: 250-264.
- Reiss S (1991) Expectancy model of fear, anxiety, and panic. Clin Psychol Rev 11: 141-153.
- Reiss S, McNally RJ (1985) Expectancy model of fear. In Reiss S & Bootzin RR (Edn), Theoretical issues in behavior therapy. New York: Academic Press.
- Taylor S, Koch WJ, McNally RJ, Crockett DJ (1992) Conceptualizations of anxiety sensitivity. Psychol Assess 4: 245-250.
- Schmidt NB, Capron DW, Raines AM, Allan NP (2014) Randomized clinical trial evaluating the efficacy of a brief intervention targeting anxiety sensitivity cognitive concerns. J Cross Cult Psychol 82: 1023-1033.
- Reiss S (1997) Trait anxiety: It's not what you think it is. J Anxiety Disord 11: 201-214.
- McNally RJ (1989) Is anxiety sensitivity distinguishable from trait anxiety? Reply to Lilienfeld, Jacob, and Turner (1989). J Abnorm Psychol 98: 193-194.
- Francis SE, Noël VA (2010) Parental contributions to child anxiety sensitivity: a review and recommendations for future directions. Child Psychiatry Hum Dev 41: 595–613.
- Noël VA, Francis SE (2011) A meta-analytic review of the role of child anxiety sensitivity in child anxiety. J Abnorm Child Psychol 39: 721-33.
- Schmidt NB, Zvolensky MJ, Maner JK (2006) Anxiety sensitivity: Prospective prediction of panic attacks and Axis I pathology. J Psychiatr Res 40: 691-699.
- Wilson KA, Hayward C (2006) Unique contributions of anxiety sensitivity to avoidance: a prospective study in adolescents. Behav Res Ther 44: 601-609.
- Taylor S (1999) Anxiety sensitivity: theory, research, and treatment of the fear of anxiety. Lawrence Erlbaum Associates Publishers, p: 384.
- McNally RJ, Hornig CD, Hoffman EC, Han EM (1999) Anxiety sensitivity and cognitive biases for threat. Behav Ther 30: 51-61.
- Lilienfeld SO, Turner SM, Jacob RG (1993) Anxiety sensitivity: an examination of theoretical and methodological issues. Adv Behav Res Ther 15:147-183.
- Lilienfeld SO, Turner SM, Jacob RG (1998) Deja vu all over again: critical misunderstandings concerning anxiety sensitivity and constructive suggestions for future research. J Anxiety Disord 12: 71-82.
- Sullivan HS (1953) The interpersonal theory of psychiatry. New York: Norton & Company, p: 393.
- Cacioppo JT, Hawkley LC, Ernst JM, Burleson M, Berntson GG, et al. (2006) Loneliness within a nomological net: an evolutionary perspective. J Res Pers 40: 1054-1085.
- Gerson AC, Perlman D (1979) Loneliness and expressive communication. J Abnorm Psychol 88: 258-261.
- Hayward C, Killen JD, Taylor CB (2003) The relationship between agoraphobia symptoms and panic disorder in a non-clinical sample of adolescents. Psychol Med 33: 733-738.
- Zvolensky MJ, Forsyth JP (2002) Anxiety sensitivity dimensions in the prediction of body vigilance and emotional avoidance. Cognit Ther Res 26: 449-460.
- Hayward C, Wilson KA (2007) Anxiety sensitivity: a missing piece to the agoraphobia-without-panic puzzle. Behav Modif 31: 162-173.
- Bartholomew K, Horowitz LM (1991) Attachment styles among young adults: a test of a four-category model. J Pers Soc Psychol 61: 226-244.
- DiTommaso E, Brannen-McNulty C, Ross L, Burgess M (2003) Attachment styles, social skills and loneliness in young adults. Pers Individ Dif 35: 303 -312.
- Wiseman H, Mayseless O, Sharabany R (2006) Why are they lonely? Perceived quality of early relationships with parents, attachment, personality predispositions and loneliness in first-year university students. Pers Individ Dif 40: 237-248.
- Brennan KA, Clark CL, Shaver PR (1998) Self-report measurement of adult attachment: an integrative overview. In Simpson JA & Rholes WS, (Edn) Attachment theory and close relationships New York: Guilford Press 46-76.
- Mikulincer M, Shaver PR (2014) Mechanisms of social connection: from brain to group. Washington, DC: American Psychological Association, p: 426.
- Schinka KC, VanDlumen MHM, Bossart R, Swahn M (2012) Association between loneliness and suicidality during middle childhood and adolescence: longitudinal effects and role of demographic characteristics. J Psychol 146:105-118.
- Watt MC, McWilliams LA, Campbell AG (2005) Relations between anxiety sensitivity and attachment style dimensions. J Psychopathol Behav Assess 27: 191-200.
- Lilienfeld SO, Jacob RG, Turner SM (1989) Comment on Holloway and McNally's (1987) ‘Effects of anxiety sensitivity on the response to hyperventilation'. J Abnorm Psychol 98: 100-102.
- Russell D, Peplau LA, Cutrona CE (1980) The revised UCLA loneliness scale: concurrent and discriminant validity evidence. J Pers Soc Psychol 39: 472-480.
- Finch H (2007) Performance of the Roy-Bargmann Stepdown procedure as a follow up to a significant MANOVA. Multiple Linear Regression Viewpoints 33: 12-22.
- Spielberger CD (1983) Manual for the state-trait anxiety inventory (Form y). Palo Alto, CA: Consulting Psychologists Press.
- Marks IM, Mathews AM (1979) Brief standard self-rating for phobic patients. Behav Res Ther 17: 263-267.
- Trull TJ, Hillerbrand E (1990) Psychometric properties and factor structure of the fear questionnaire phobia subscale items in two normative samples. J Psychopathol Behav Assess 12: 285-297.
- Reiss S, Peterson RA, Gursky DM, McNally RJ (1986) Anxiety sensitivity, anxiety frequency and the prediction of fearfulness. Behav Res Ther 24: 1-8.
- Tabachnick BG, Fidell LS (2013) Using multivariate statistics (6th Edn) Pearson Education Limited.
- Cox BJ, Borger SC, Enns MW (1999) Anxiety sensitivity and emotional disorders: psychometric studies and their theoretical implications. In Taylor S (Edn) Anxiety sensitivity: Theory, research, and treatment of the fear of anxiety Mahwah, NJ, US: Lawrence Erlbaum Associates Publishers 115-148.
- Taylor S, Koch WJ, McNally RJ (1992) How does anxiety sensitivity vary across the anxiety disorders? J Anxiety Disord 6: 249-259.
- Huberty CJ, Morris JD (1989) Multivariate analysis versus multiple univariate analyses. Psychol Bull 105: 302-308.
- Bravo IM, Silverman WK (2001) Anxiety sensitivity, anxiety, and depression in older patients and their relation to hypochondriacal concerns and medical illnesses. Aging Ment Health 5: 349-357.
- Perlman D, Landolt MA (1999) Examination of loneliness in children, adolescents and in adults: two solitudes or a unified enterprise? In Rotenberg KJ & Hymel S (Edn) Loneliness in childhood and adolescence. Cambridge, England: Cambridge University Press 325-347.
- De Jong Gierveld J, Tesch-Römer C (2012) Loneliness in old age in Eastern and Western European societies: theoretical perspectives. Eur J Ageing 9: 285-295.

