Kimberly L. Johung1, Muhammad Wasif Saif2, Bryan W. Chang1
1Yale University School of Medicine, New Haven, CT, USA
2Tufts University School of Medicine, Boston, MA, USA
- *Corresponding Author:
- Bryan W. Chang
Yale University School of Medicine
Department of Therapeutic Radiology
P.O. Box 208040, New Haven
CT 06520-8040
USA
Phone: +1.203-200-2100
Fax: +1.203-785-4622
E-mail bryan.chang@yale.edu
Keywords
Chemoradiotherapy; Induction Chemotherapy; Pancreatic Neoplasms
What Did We Know Before ASCO 2014?
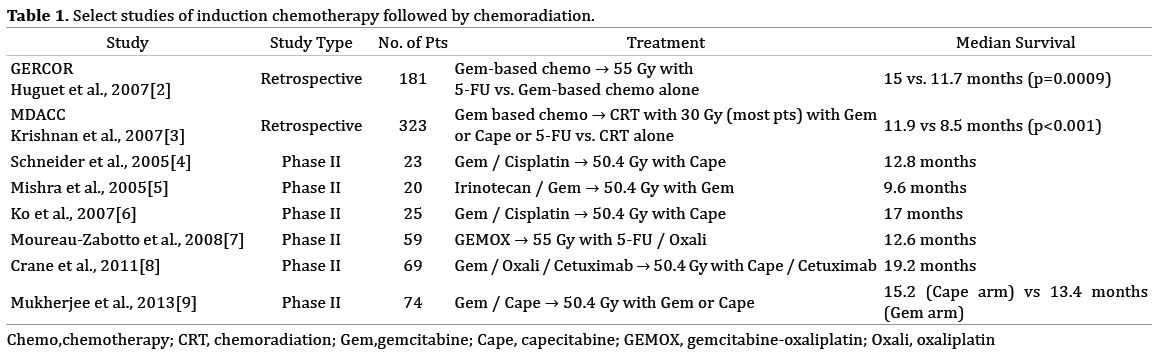
Recent advances in the treatment of locally advanced pancreatic cancer have demonstrated modest improvements in outcomes. A role for concurrent chemoradiation was established in the Eastern Cooperative Oncology Group (ECOG) 4201 study [1]. Despite low accrual, there was a small yet significant median survival benefit with gemcitabine chemoradiation compared to gemcitabine alone (11 versus 9.2 months, respectively). Retrospective and phase II studies summarized in Table 1 have shown a further survival benefit with chemoradiation after induction chemotherapy is used to exclude those patients with early distant failure.
What Did We Learn at ASCO 2014?
Impact of Chemoradiotherapy (CRT) on Local Control and Time Without Treatment in Patients With Locally Advanced Pancreatic Cancer (LAPC) Included in the International Phase III LAP 07 Study.
The GERCOR LAP 07 phase III study employed a 2x2 randomization to evaluate the benefit of chemoradiation after 4 months of induction gemcitabine, and also the benefit of adding erlotinib to the treatment regimen (Figure 1). Overall survival results were presented at 2013 ASCO Annual Meeting. At 3 years median follow up, median survival was equivalent in the chemotherapy arms compared to the chemoradiation arms (16.5 versus 15.3 months, respectively; p=0.8). Further analysis presented at this year’s ASCO meeting demonstrated a trend towards improved progression free survival with CRT vs. chemotherapy (p=0.055), and a significant local control benefit with CRT. Local progression was reduced by nearly 50% with CRT compared to chemotherapy alone, from 65% to 34% (p<0.0001). Tumor progression occurred in 87% of patients, and one third of these patients (34%) had local progression only. Isolated local disease as the first site of progression was significantly reduced with CRT vs. chemo (32 vs. 46%, p = 0.035). Improved local control correlated with a significantly prolonged treatment-free interval of 5.3 months after CRT compared to 3.2 months (p=0.05).
Figure 1. Design of the GERCOR LAP 07 Study.
Impact Of Gemcitabine (Gem)- or Capecitabine (Cape)- Based Chemoradiation (CRT) on Health-Related Quality of Life (HRQL) in Patients With Locally Advanced Pancreatic Cancer (LAPC): Outcomes from the Randomized Phase II SCALOP Trial.
The SCALOP trial randomized patients to 50.4 Gy of conformal radiation to a margin around the primary tumor and involved nodes with concurrent gemcitabine or capecitabine. Median overall survival was superior by 2 months in the capecitabine arm (15.2 vs. 13.4 months, p=0.01), and grade 3-4 hematologic toxicity was significantly lower. Quality of life was assessed at baseline, after induction therapy, after CRT, and at 3 weeks and 4 months post-CRT. Patient reported quality of life was significantly better immediately post-CRT compared to pre-CRT in terms of fatigue, cognitive function, xerostomia, and bloating. By 3 weeks and 4 months post-treatment, only cognitive function and xerostomia differed in quality of life assessments.
Prognosis Model for Overall Survival in Locally Advanced Pancreatic Cancer (LAPC): An Ancillary Study of the LAP 07 Trial
Vernerey et al. evaluated 35 clinicopathologic factors in the LAPC patients enrolled in the LAP 07 trial, and used statistical modeling to define a prognostic score which classifies patients into three risk groups with median OS ranging from 18.8 months in the low risk group to 11.8 months in the high risk group. Age, pain, albumin level, and tumor size were identified as independent predictors of overall survival.
Discussion
The role of CRT in the treatment of LAPC remains controversial. Despite promising results in retrospective and phase II studies, the phase III LAP 07 trial did not show a survival benefit with CRT following induction chemotherapy, compared to continued systemic therapy. This lack of survival benefit may be a result of inferior induction chemotherapy, as both FOLFIRINOX and nabpaclitaxel have been shown to significantly improve overall survival in metastatic disease compared to gemcitabine alone in the phase III trial published by Conroy et al. [10], and the MPACT trial [11]. Data from the LAP 07 trial presented at ASCO 2014 indicates that CRT improves local control. Quality of life data from this trial has not been presented, but it will be interesting to see if improved local control and time off of treatment are associated with a quality of life benefit for the radiation arm. Moreover, the local control benefit with CRT, coupled with the previously published data suggesting a survival benefit with CRT, suggests that induction chemotherapy followed by CRT may still be of benefit in LAPC if distant disease control can be improved with superior systemic regimens.
Controversy remains regarding the optimal concurrent systemic agent with radiation. The SCALOP trial demonstrates improved survival outcomes with capecitabine, but the dose of gemcitabine was half of what was prescribed in the ECOG 4201 study [1]. The inferior quality of life reported with concurrent gemcitabine as opposed to capecitabine is surprising, as rates of grade 3-4 toxicity, and quality of life measurements were equivalent with concurrent gemcitabine and radiation compared to gemcitabine alone in the ECOG study. There was a non-significant trend towards improved progressionfree survival on the Cape-CRT arm, and the quality of life benefit may be a reflection of delayed tumor progression and prolonged time to salvage therapy.
The prognostic model proposed from the LAP 07 trial highlights the importance of using such models to select patients likely to benefit from escalation of therapy. Currently, induction chemotherapy is employed to select a subset of patients without distant progression that would benefit from local therapy with CRT. In the future, biomarkers and models such as this one may give up-front information about the likely future behavior of the tumor, allowing for the selection of patients likely to derive an overall survival benefit from intensification of local therapy.
Conflict of Interest
The authors have no potential conflicts of interest.
References
- Loehrer PJ, Feng Y, Cardenes H, Wagner L, Brell JM, Cella D, Flynn P, et al. Gemcitabine alone versus gemcitabine plus radiotherapy in patients with locally advanced pancreatic cancer: an Eastern Cooperative Oncology Group trial. J ClinOncol. 2011; 29:4105-12. [PMID:21969502]
- Huguet F, André T, Hammel P, Artru P, Balosso J, Selle F, Deniaud- Alexandre E, et al. Impact of chemoradiotherapy after disease control with chemotherapy in locally advanced pancreatic adenocarcinoma in GERCOR phase II and III studies. J ClinOncol. 2007; 25:326-31. [PMID:17235048]
- Krishnan S, Rana V, Janjan NA, Varadhachary GR, Abbruzzese JL, Das P, Delclos ME, et al. Induction chemotherapy selects patients with locally advanced,unresectable pancreatic cancer for optimal benefit from consolidative chemoradiation therapy. Cancer. 2007; 110:47-55. [PMID:17538975]
- Schneider BJ, Ben-Josef E, McGinn CJ, Chang AE, Colletti LM, Normolle DP, Hejna GF, et al. Capecitabine and radiation therapy preceded and followed by combination chemotherapy in advanced pancreatic cancer. Int J RadiatOncolBiol Phys. 2005; 63:1325-30. [PMID:15993549]
- Mishra G, Butler J, Ho C, Melin S, Case LD, Ennever PR, Magrinat GC, et al. Phase II trial of induction gemcitabine/CPT-11 followed by a twice-weekly infusion of gemcitabine and concurrent external beam radiation for the treatment of locally advanced pancreatic cancer. Am J ClinOncol. 2005; 28:345-50. [PMID:16062075]
- Ko AH, Quivey JM, Venook AP, Bergsland EK, Dito E, Schillinger B, Tempero MA. A phase II study of fixed-dose rate gemcitabine plus low-dose cisplatin followed by consolidative chemoradiation for locally advanced pancreatic cancer. Int J RadiatOncolBiol Phys. 2007; 68:809- 16. [PMID:17363191]
- Moureau-Zabotto L, Phélip JM, Afchain P, Mineur L, André T, Vendrely V, Lledo G, et al. Concomitant administration of weekly oxaliplatin, fluorouracil continuous infusion, and radiotherapy after 2 months of gemcitabine and oxaliplatin induction in patients with locally advanced pancreatic cancer: a GroupeCoordinateurMultidisciplinaire en Oncologie phase II study. J ClinOncol. 2008; 26:1080-5. [PMID:18309942]
- Crane CH, Varadhachary GR, Yordy JS, Staerkel GA, Javle MM, Safran H, Haque W, et al. Phase II trial of cetuximab, gemcitabine, and oxaliplatin followed by chemoradiation with cetuximab for locally advanced (T4) pancreatic adenocarcinoma: correlation of Smad4(Dpc4) immunostaining with pattern of disease progression. J ClinOncol. 2011; 29:3037-43. [PMID:21709185]
- Mukherjee S, Hurt CN, Bridgewater J, Falk S, Cummins S, Wasan H, Crosby T, et al. Gemcitabine-based or capecitabine-based chemoradiotherapy for locally advanced pancreatic cancer (SCALOP): a multicentre, randomised, phase 2 trial. Lancet Oncol. 2013; 14:317-26. [PMID:23474363]
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, Adenis A, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011; 364:1817-25. [PMID:21561347]
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, Seay T, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013; 369:1691-703. [PMID:24131140]


