Keywords
gemcitabine; Neoadjuvant Therapy; Pancreatic Neoplasms
Abbreviations
GERCOR: Groupe d'Etude et de Recherche en Cancreologie Onco-Radiotherapic; NCCN: National Comprehensive Cancer Network; S-1: tegafur, gimeracil, and oteracil potassium
INTRODUCTION
Pancreatic cancer remains a major unsolved health problem, representing approximately 3% of new cancer diagnoses last year (42,470 new cases) and 6% of the total cancer deaths (35,240) in the United States [1]. Unfortunately most patients present with locally advanced or metastatic disease at the time of diagnosis leaving relatively few patients as candidates for upfront resection. Locally advanced disease is observed in 15- 20% of all patients with pancreatic cancer, and is associated with a median survival of 6-10 months. Locally advanced pancreatic cancer is defined as surgically unresectable because of the encasement or occlusion of the superior mesenteric vein or portal vein confluence, or direct involvement of the superior mesenteric artery, celiac axis, inferior vena cava, or aorta. Four randomized control trials have compared the effectiveness of chemoradiation incorporating 5- fluorouracil with radiation alone or systemic chemotherapy [2, 3, 4, 5]. Three of these trials showed an improved median survival of 10.1-10.6 months for radiotherapy plus 5-fluorouracil alone or triple therapy (streptozocin, mitomycin C and 5-fluorouracil) compared with 5.7-6.3 months for radiotherapy alone or systemic chemotherapy with streptozocin, mitomycin C and 5-fluorouracil. Based on these data, chemoradiotherapy has been considered a standard therapy for locally advanced pancreatic cancer.
Locally advanced pancreatic adenocarcinoma represents a particularly troublesome area with several unanswered questions: What is the optimal regimen for locally advanced pancreatic adenocarcinoma? What is the role of the neoadjuvant approach? Is there a role for radiotherapy? Do we know how to incorporate targeted agents in this setting? The Groupe d'Etude et de Recherche en Cancreologie Onco-Radiotherapic (GERCOR) has provided continued work in this area to help provide some much needed answers. In 2007 Huguet et al. explored the role of chemoradiotherapy in patients achieving either disease stability or improvement following upfront chemotherapy. They found an improvement in progression free survival and overall survival between the chemoradiotherapy and the chemotherapy arms of 10.8 and 7.4 months (P=0.005) and 15.0 and 11.7 (P=0.0009) months, respectively [6]. A phase III study conducted with the addition of oxaliplatin to gemcitabine (versus gemcitabine alone) in the locally advanced setting has shown improvement in response rates and progression free survival but not in overall survival [7]. Although this trial failed to show a survival advantage; the improvement in response rates were marked (14.9% versus 27.4%), providing an approach for patients with “borderline-resectable” disease who may have the potential to become surgical candidates.
The following abstracts, presented at the 2010 ASCO Gastrointestinal Cancers Symposium, seek to add to our breadth of knowledge of the treatment of locally advanced pancreatic cancer (Table 1).

Update on Treatment in Locally Advanced Pancreatic Cancer
Abstract #132: Multi-institutional phase II trial of induction cetuximab, gemcitabine, and oxaliplatin, followed by radiotherapy with concurrent capecitabine, and cetuximab, for locally advanced pancreatic adenocarcinoma (LAPC) [8]
This phase II study evaluates the role of induction therapy with chemotherapy alone followed by chemoradiotherapy. Sixty-nine, treatment naïve patients were accrued between October 2005 and June 2009 and given induction therapy with gemcitabine and oxaliplatin. Figure 1 shows the treatment schema. After 4 doses patients were re-imaged with CT scans and those without progression of disease went on to receive radiation therapy with concurrent capecitabine. Cetuximab was administered on a biweekly basis starting on day 1 and continued throughout the treatment regimens with chemotherapy and chemoradiotherapy. The primary and secondary endpoints were 1-year overall survival and response and safety, respectively. The 1-year overall survival was 66.7% (95% confidence interval (CI): 60.2-73.2%) with a median survival of 19 months. Four patients who initially presented with disease that was deemed unresectable were “converted” into surgical candidates and underwent R0 resections. Major adverse events were constitutional, gastrointestinal, neuropathic, and hematologic. Sixty percent of patients experienced at least a grade-2 acneiform rash. Overall this regimen was tolerated reasonably well and was associated with encouraging responses.
Figure 1. Induction chemotherapy followed by chemoradiotherapy
for LAPC: treatment schema for abstract #132 [8].
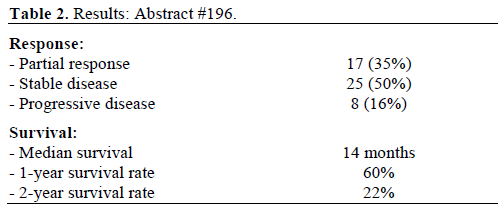
Abstract #196: Phase II study of oral fluoropyrimidine anticancer agent (S-1) with concurrent external-beam radiotherapy for locally advanced pancreatic cancer [9]
Fluoropyrimidines have been a mainstay in the treatment of gastrointestinal malignancies for many years. Infusional formulations such as 5-fluorouracil can often time be cumbersome to administer. Several oral formulations have emerged and offer a multitude of potential benefits. S-1 is a new oral formulation consisting of 1 M tegafur, 0.4 M gimeracil and 1 M oteracil potassium. S-1 was developed by the scientific theory of both potentiating antitumor activity of 5- fluorouracil and reducing gastrointestinal toxicity induced by 5-fluorouracil [10, 11]. S-1 is widely used in Japan in both the adjuvant and metastatic setting as both monotherapy and in combination with gemcitabine. The key clinical sites and functional pathways of activity are noted in Figure 2.
Figure 2. S-1: an oral fluoropyrimidine [24].
Ikeda et al. evaluated the combination of S-1 and concomitant radiotherapy in a phase I study; yielding a recommended treatment dose of 80 mg/m2 [12]. The median survival for patients in this study (at varied S-1 doses) was 11.0 months. Although two patients reached dose-limiting toxicity in the 70 mg/m2 dosing, no patients reached dose-limiting toxicity at the 50, 60, or 80 mg/m2 dose [12].
Patients were deemed eligible if they had locally advanced pancreatic cancer, without evidence of distant metastatic disease, Eastern Cooperative Oncology Group (ECOG) 0-1, and adequate organ function. S-1 was administered at 80 mg/m2 po twicedaily on days 1-21 along with radiation therapy. External beam radiotherapy (EBRT) was administered at 1.25 Gy/fraction twice daily over a period of 4 weeks for a total of 40 fractions (50 Gy). Following the initial chemoradiotherapy induction, a maintenance period of S-1 monotherapy was administered on a “14 day on, 14 day off” schedule at the previous dosage. This was continued until disease progression or cessation due to toxicity.
Of the 50 patients entered into the trial all but two completed the planned regimen of chemoradiotherapy. Forty-two patients (85%) had stable disease or better by Response Evaluation Criteria in Solid Tumors (RECIST) criteria [13] (Table 2). The regimen was tolerated quite well overall and was associated with only two instances of grade 3 toxicities and no grade 4 toxicities. This approach appears quite favorable and further phase III studies are warranted.
Abstract #218: Factors predicting outcomes in patients with locally advanced pancreatic cancer (LAPC) [14]
Surgical resection remains the cornerstone of curability in patients in pancreatic cancer. Although a minority of patients will be candidates for upfront surgical resection; a number of patients with unresectable, locally advanced disease at presentation can be converted to an operable status. Moskovic et al. have sought to tease out the factors associated with this phenomenon in hopes of formulating a prediction schema which may help to guide initial management of locally advanced pancreatic cancer.
Multiple factors were evaluated for a patient cohort of 150 patients with locally advanced pancreatic adenocarcinoma. These included demographics such as age, race, gender; laboratory data such as CA 19-9 levels; as well as anatomic data looking at primary tumor location and presence of vascular invasion. The primary endpoint was rate of conversion to resectability and its correlative factors. Secondary endpoints were overall and progression free survivals and utilization of second-line chemotherapy. Eight patients were not evaluated in the final analysis as complete records were unavailable for those subjects. In total 26 out of 142 (18.3%) patients were converted to resectability following chemotherapy with or without chemoradiotherapy. Although multiple variables affected the likelihood of survival; only anatomic variables had a significant effect on rates of resectability. All tumors which were eventually deemed “resectable” were located either in the head of the pancreas or in the uncinate process (P=0.0002). Tumors which remained unresectable were more likely to have either celiac artery invasion (P=0.001) or superior mesenteric artery invasion (P<0.001).
Younger age, lower CA 19-9, and maintenance chemotherapy all correlated with a statistically significant improvement in progression free survival. Older age, higher CA 19-9, and lack of maintenance therapy trended towards lower overall survival and progression free survival but did not reach significance. The findings of this abstract can help to guide a plan of care for patients with locally advanced pancreatic cancer and offer some prognostic methodology as well.
Abstract #220: A phase I study of weekly oxaliplatin (Ox) and gemcitabine (Gem) during radiotherapy (RT) for unresectable pancreatic or biliary carcinoma [15]
Gemcitabine has been shown to be a potent radiosensitizer in pancreatic cancer cells [16]. Although the standard weekly dosing of gemcitabine is 1,000 mg/m2; phase I studies have demonstrated a significant increase in hematologic and hepatic doselimiting toxicities at this dosing level [17]. In turn, when gemcitabine is given concomitantly with radiation, the dosing ranges are typically on the order of 100-400 mg/m2. The combination of gemcitabine and oxaliplatin has been studies in the locally advanced and metastatic setting in the GERCOR and the Italian Group for the Study of Gastrointestinal Tract Carcinomas (GISCAD) trials [7]. While this study did not demonstrate a significant improvement in overall survival; significant improvements were seen in response rates and progression free survival. The abstract discussed here offers phase I data examining the role of the combination of gemcitabine and oxaliplatin in the locally advanced setting when combined with radiotherapy.
Patients were allocated into 4 treatment arms based on a 3x3 design. Four dosing levels were tested with gemcitabine doses ranging 100-200 mg/m2 and oxaliplatin doses ranging 30-60 mg/m2. The chemotherapy was administered on a weekly basis (for a maximum of 6 doses) along with daily radiation of 180 cGy/fraction for a cumulative dose of 50.4 Gy.
The highest dosing cohort (gemcitabine 200 mg/m2 plus oxaliplatin 60 mg/m2) had no dose-limiting toxicities. Major side effects included leukopenia, nausea and hyperglycemia. Overall survival was 10.8 months with a 95% CI of 7.1-16.7 months and progression free survival was 9.6 months with a 95% CI of 4.6-11.1 months. This dosing level cohort has been expanded for further testing. Phase II/III studies are warranted to explore this approach further.
Discussion
Optimal therapy for patients with locally advanced pancreatic cancer remains elusive. Early clinical data presented at the 2010 ASCO Gastrointestinal Cancers Symposium offer a multitude of venues for further research. The National Comprehensive Cancer Network (NCCN) guidelines recommend gemcitabine monotherapy versus gemcitabine based chemoradiotherapy [18]. The position of the NCCN remains that the best approach for all patients with cancer is clinical trial.
As surgical resection remains a key component of the curative strategy; a neoadjuvant approach in the locally advanced setting represents a viable pathway to long term survival. A recent meta-analysis by Morganti et al. showed evidence that patients who do not progress after induction therapy may benefit from radical surgical approaches in skilled surgical settings [19]. In Japan the availability of S-1 allows for its use in concert with gemcitabine based chemoradiotherapy in efforts to convert patients to resectability [20, 21].
Other agents, such as irinotecan, which has shown activity in a variety of gastrointestinal tumors has been used as a radiosensitizer in patients with locally advanced pancreatic adenocarcinoma. Phase I data from de la Fouchardière C, et al. has shown activity with median survival times of 12.6 months [22].
Gene therapy also shows interesting promise as an adjunct in the neoadjuvant approach. Early data with the use of TNFerade® (GenVec Inc., Gaithersburg, MD, USA) has shown promise when used with radiotherapy with or without chemotherapy. TNFerade® delivers and modulates tumor necrosis factor alpha via a replication deficient adenovirus under the influence of a radiation-inducible gene promoter [23].
Targeted therapy has found a home in the age of personalized medicine. Moskovic et al. [14] offers an excellent framework for the “tailoring” of therapies based on individual patient/tumor nuances. As our knowledge advances in the fields of tumor biology and molecular analysis we begin to unravel the heterogeneity within pancreatic adenocarcinoma and can more accurately treat and potentially cure the disease.
Conflict of interest
The authors have no potential conflicts of interest
References
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, ThunMJ. Cancer Statistics, 2009. CA Cancer J Clin 2009; 59:225-49. [PMID 19474385]
- Moertel CG, Childs DS Jr, Reitemeier RJ, Colby MY Jr, Holbrook MA. Combined 5-fluorouracil and supervoltage radiation therapy of locally unresectable gastrointestinal cancer. Lancet 1969; 2:865-7. [PMID 4186452]
- Moertel CG, Frytak S, Hahn RG, O'Connell MJ, Reitemeier RJ, Rubin J, et al. Therapy of locally unresectable pancreatic carcinoma: a randomized comparison of high dose (6000 rads) radiation alone, moderate dose radiation (4000 rads + 5-fluorouracil), and high dose radiation + 5-fluorouracil: The Gastrointestinal Tumor Study Group. Cancer 1981; 48:1705-10. [PMID 7284971]
- Treatment of locally unresectable carcinoma of the pancreas: comparison of combined-modality therapy (chemotherapy plus radiotherapy) to chemotherapy alone. Gastrointestinal Tumor Study Group. J Natl Cancer Inst 1988; 80:751-5. [PMID 2898536]
- Klaassen DJ, MacIntyreJM, Catton GE, Engstrom PF, Moertel CG. Treatment of locally unresectable cancer of the stomach and pancreas: a randomized comparison of 5-fluorouracil alone with radiation plus concurrent and maintenance 5-fluorouracil--an Eastern Cooperative Oncology Group study. J ClinOncol 1985; 3:373-8. [PMID 3973648]
- Huguet F, André T, Hammel P, Artru P, Balosso J, Selle F, et al. Impact of chemoradiotherapy after disease control with chemotherapy in locally advanced pancreatic adenocarcinoma in GERCOR phase II and III studies. J ClinOncol 2007; 20:326-31. [PMID 17235048]
- Louvet C, Labianca R, Hammel P, Lledo G, Zampino MG, André T, et al. Gemcitabine in combination with oxaliplatin compared with gemcitabine alone in locally advanced or metastatic pancreatic cancer: results of a GERCOR and GISCAD phase III trial. J ClinOncol 2005; 23:3509-16. [PMID 15908661]
- Crane CH, Varadhachary GR, Javle MM, Safran H, Krishnan S, Fleming JB, et al. Multi-institutional phase II trial of induction cetuximab, gemcitabine, and oxaliplatin, followed by radiotherapy with concurrent capecitabine, and cetuximab, for locally advanced pancreatic adenocarcinoma (LAPC). 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 132.
- Shinchi H, Takao S. Phase II study of oral fluoropyrimidine anticancer agent (S-1) with concurrent external-beam radiotherapy for locally advanced pancreatic cancer. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 196.
- Murakami Y, Uemura K, Sudo T, Hayashidani Y, Hashimoto Y, Nakagawa N, et al. Adjuvant gemcitabine plus S-1 chemotherapy after surgical resection for pancreatic adenocarcinoma. Am J Surg 2008; 195:757-62. [PMID 18367131]
- Nakamura K, Yamaguchi T, Ishihara T, Sudo K, Kato H, Saisho H. Phase II trial of oral S-1 combined with gemcitabine in metastatic pancreatic cancer. Br J Cancer 2006; 94:1575-9. [PMID 16721372]
- Ikeda M, Okusaka T, Ito Y, Ueno H, Morizane C, Furuse J, et al. A phase I trial of S-1 with concurrent radiotherapy for locally advanced pancreatic cancer. Br J Cancer 2007; 96:1650-5. [PMID 17533388]
- Therasse P, ArbuckSG, EisenhauerEA, Wanders J, Kaplan RS, Rubinstein L, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 2000; 92:205-16. [PMID 10655437]
- Moskovic DJ, Carlson PJ, Dakik HK, Qiao W, Javle MM, Fogelman DR. Factors predicting outcomes in patients with locally advanced pancreatic cancer (LAPC). 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 218.
- Raftery LL, Tepper JE, Goldberg RM, Blackstock AW, Aklilu M, Bernard SA, et al. A phase I study of weekly oxaliplatin (Ox) and gemcitabine (Gem) during radiotherapy (RT) for unresectable pancreatic or biliary carcinoma. 2010 ASCO Gastrointestinal Cancers Symposium. Abstract No. 220.
- Lawrence TS, Chang EY, Hahn TM, HertelLW, Shewach DS. Radiosensitization of pancreatic cancer cells by 2',2'-difluoro-2'- deoxycytidine. Int J RadiatOncolBiolPhys 1996; 34:867-72. [PMID 8598364]
- Ikeda M, Okada S, Tokuuye K, Ueno H, Okusaka T. A phase I trial of weekly gemcitabine and concurrent radiotherapy in patients with locally advanced pancreatic cancer. Br J Cancer 2002; 86:1551- 4. [PMID 12085203]
- National Comprehensive Cancer Network. Pancreatic Adenocarcinoma V.1.2009. NCCN Clinical Practice Guidelines in Oncology.
- Morganti AG, Massaccesi M, La Torre G, Caravatta L, Piscopo A, Tambaro R, et al. A systematic review of resectability and survival after concurrent chemoradiation in primarily unresectable pancreatic cancer. Ann SurgOncol 2010; 17:194-205. [PMID 19856029]
- Nakachi K, Furuse J, Kinoshita T, Kawashima M, Ishii H, Ikeda M, et al. A phase II study of induction chemotherapy with gemcitabine plus S-1 followed by chemoradiotherapy for locally advanced pancreatic cancer. Cancer ChemotherPharmacol 2009 Dec 5. [PMID 19967537]
- Watanabe F, Honda G, Kurata M, Tsuruta K, Tokashiki T, Funada N. A case report-neoadjuvantchemoradiotherapy with combination of S-1 and gemcitabine in a patient with locally advanced pancreatic cancer. GanTo Kagaku Ryoho 2009; 36:2430- 2. [PMID 20037446]
- de la Fouchardière C, Négrier S, Labrosse H, Martel Lafay I, Desseigne F, Méeus P, et al. Phase I study of daily irinotecan as a radiation sensitizer for locally advanced pancreatic cancer. Int J RadiatOncolBiolPhys 2010 Jan 28. [PMID 20116933]
- Chadha MK, Litwin A, Levea C, Iyer R, Yang G, Javle M, Gibbs JF. Surgical resection after TNFerade therapy for locally advanced pancreatic cancer. JOP. J Pancreas (Online) 2009; 10:535- 8. [PMID 19734632]
- Saif MW. Pancreatic cancer: are we moving forward yet? Highlights from the Gastrointestinal Cancers Symposium. Orlando, FL, USA. January 20th, 2007. JOP. J Pancreas (Online) 2007; 8:166- 76. [PMID 17356239]



