Keywords
bevacizumab; erlotinib; Fluorouracil; gemcitabine; oxaliplatin; Pancreatic Neoplasms; Radiotherapy
Abbreviations
FOLFIRINOX: 5-fluorouracil, leucovorin, irinotecan, and oxaliplatin
What We Knew Before the 2011 ASCO GI Cancer Symposium
Locally advanced pancreatic cancer, in which the tumor has not metastasized but encases the celiac axis or superior mesenteric artery, is by definition unresectable and represents about 25% of pancreatic cancer cases at presentation. Patients with limited vascular involvement by tumor are considered to have borderline resectable disease and are often treated as locally advanced pancreatic cancer. Treatments range from chemoradiation to chemotherapy alone to induction chemotherapy followed by chemoradiation for patients who do not metastasize [1, 2, 3]. The median survival is limited to 10-12 months, leaving significant room for improvement.
What We Learned at the 2011 ASCO GI Cancer Symposium
Novel Agents for Locally Advanced Pancreatic Cancer Phase I trial of gene-mediated cytotoxic immunotherapyin combination with chemoradiation for locally advanced pancreatic cancer
Bloomston et al. injected escalating doses of an adenoviral vector containing HSV-thymidine kinase gene into tumors of a dozen patients with locally advanced pancreatic cancer, followed by treatment with an anti-viral prodrug and standard 5-fluorouracil (5-FU) and radiation. (Abstract #195). No doselimiting toxicities were seen and there were two partial responses [4].
A phase I study of erlotinib, bevacizumab, and external beam radiation therapy (RT) for patients with localized pancreatic carcinoma (PC)
Dr. Czito and the Duke University group completed a phase I dose-escalation trial of erlotinib, a smallmolecule inhibitor of the epidermal growth factor receptor (EGFR), with bevacizumab, a monoclonal antibody inhibitor of vascular endothelial growth factor (VEGF) (Abstract #281). Borderline resectable and locally advanced pancreatic cancer patients were enrolled. Three of the 9 patients enrolled went to surgery, but only one underwent successful resection [5].
Discussion
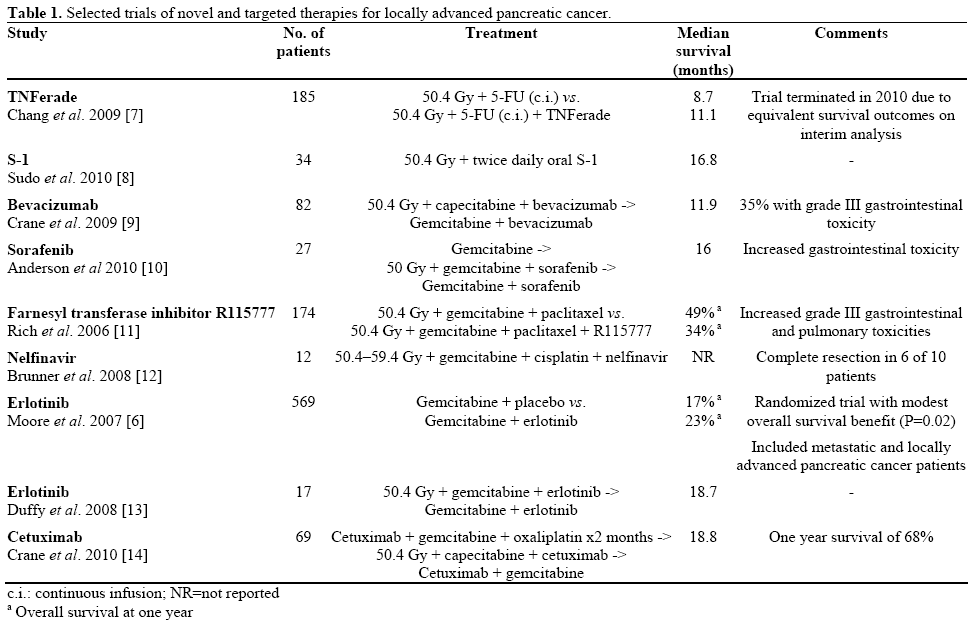
The combination of gemcitabine with erlotinib has been shown to modestly extend survival in patients with metastatic pancreatic cancer in comparison to gemcitabine monotherapy [6]. Numerous other biological and targeted therapies have been studied in metastatic and locally advanced disease, without benefit (Table 1). Gene-mediated cytotoxic immunotherapy is a fascinating and elegant concept and appears safe in phase I, but further studies are required to evaluate its true benefit in terms of efficacy. A recent phase III trial of an injectable adenoviral vector bearing tumor necrosis factor-alpha failed to show a survival benefit when added to conventional chemoradiation [7].
Erlotinib and bevacizumab are both felt to have enhance the antitumor effect of radiotherapy [15, 16], but efficacy in the Duke series does not seem overwhelming. A note of caution is in order as bevacizumab is known to cause wound healing complications after surgery [17], and two patients in this series had serious post-operative complications.
Which Chemotherapy to Combine with Radiotherapy Long-term results of full-dose gemcitabine with radiation therapy compared to 5-fluorouracil with radiation therapy for locally advanced pancreatic cancer.
Huang et al. retrospectively reviewed records of 93 patients with locally advanced pancreatic cancer (Abstract #287). Patients treated with concurrent fulldose gemcitabine and radiation had improved overall survival compared with those who received chemoradiation with 5-FU, and 11% survived for 5 years. There was no difference in acute gastrointestinal toxicity [18].
A phase II study of neoadjuvant gemcitabine/5- fluorouracil followed by 5-fluorouracil/oxaliplatin concurrent with radiation in patients with locally advanced pancreatic cancer.
Dr. Lin and other researchers from University of Nebraska treated 29 borderline resectable patients with 6 weeks of induction chemotherapy followed by chemoradiation to 50-50.4 Gy with 5-FU and weekly oxaliplatin (Abstract #259). Almost half of the patients experienced grade 3-4 acute toxicity, but 7 underwent margin-negative resections. The median survival was 26 months for patients undergoing resection but 10 months for the entire population [19].
Concurrent chemoradiotherapy with gemcitabine and S-1 for unresectable locally advanced pancreatic adenocarcinoma: A phase I study
Ioka et al. treated 15 patients on a phase I protocol with escalating doses of S-1 and gemcitabine combined with 50.4 Gy (Abstract #305). Dose-limiting toxicities were found to be anorexia and neutropenia. The 2-year survival rate was 44.4% [20].
Phase II trial of neoadjuvant full-dose gemcitabine, oxaliplatin, and radiation (RT) in patients with resectable (R) or borderline resectable (BR) pancreatic cancer.
Dr. Kim et al. reported the results of a multiinstitutional trial of neoadjuvant chemoradiation in resectable and borderline resectable patients (Abstract #239). The radiation dose was 30 Gy in 15 fractions. In the borderline resectable population, 19 of 30 patients had a margin-negative resection, and the median survival was 18 months [21].
Discussion
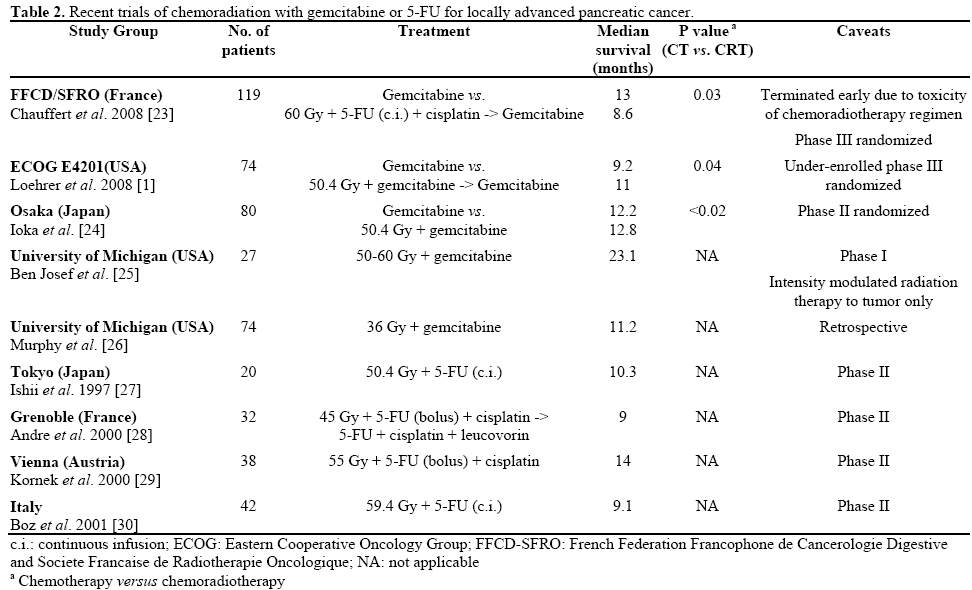
One flawed randomized trial compared gemcitabinebased chemoradiation to 5-FU-based chemoradiation, showing a survival benefit for gemcitabine [22]. Selected series of patients treated with 5-FU and gemcitabine-based regimens are presented in Table 2. Recent studies such as the results presented by Huang et al. [18] have shown promising results for gemcitabine-based chemoradiation. Of note, severe acute toxicity with concurrent full-dose gemcitabine [31] has generally necessitated dose reductions of radiotherapy, as in the Kim et al. study [21], or use of limited-field radiotherapy [32], an approach used successfully by Ioka et al. [20]. Further study in homogeneous patient populations will be needed to better define the efficacy of these promising regimens.
Chemotherapy Alone for Locally Advanced Pancreatic Cancer
Pilot study of neoadjuvant FOLFIRINOX in unresectable locally advanced (LA) pancreatic carcinoma (PC)
Hosein et al. treated 12 patients with locally advanced pancreatic cancer using 5-FU, leucovorin, irinotecan and oxaliplatin (FOLFIRINOX) off protocol (Abstract #324). Four patients were able to undergo marginnegative resections. The overall median survival was estimated at 20.7 months [33].
Phase I/II study of arterial infusion with 5-fluorouracil combined with systemic gemcitabine for unresectable pancreatic cancer
Dr. Tanaka together with a Japanese group studied the toxicity and efficacy of a chemotherapy-alone regimen including hepatic and pancreatic arterial-infusion 5-FU (Abstract #307). A number of metastatic patients were included. The partial-response rate was 68% [34].
Discussion
Trials of chemotherapy for metastatic disease have sometimes included locally advanced pancreatic cancer as well [6], which has led some investigators to treated locally advanced pancreatic cancer without radiation. While the regimen of the Tanaka et al. study appears safe, it requires further study for efficacy in a locally advanced pancreatic cancer population. FOLFIRINOX has been shown to dramatically improve survival in metastatic disease compared with gemcitabine alone [35]. The researchers from Miami and Sao Paulo [33] have reported some of the first results from use of this promising but rigorous regimen in patients with locally advanced pancreatic cancer. Both the median survival and the fact that a third of patients were rendered resectable are impressive, and further study is certainly warranted.
Conclusions
The 2011 ASCO GI Cancer Symposium showcased a number of promising, early-phase results with a variety of therapeutic approaches. The search continues for a targeted therapy with clinically significant activity in locally advanced pancreatic cancer. Meanwhile, researchers are growing increasingly adept at safely and effectively combining gemcitabine-based chemotherapy regimens with radiation. It is clear that some very good results can be obtained with gemcitabine-based chemoradiation, although the optimal approach is not yet clear. Finally, FOLFIRINOX has demonstrated intriguing activity in locally advanced pancreatic cancer, which will need to be confirmed. This regimen may also be useful as induction prior to chemoradiation for patients who do not metastasize early, as large retrospective series have shown that this is a beneficial way to deliver chemoradiation [3, 36]. There is also a need to investigate tailored or adaptive strategies to guide therapy for locally advanced pancreatic cancer. Such strategies could be guided by molecular tumor characteristics or by imaging, such as positronemission tomography. Future trials should include provisions to aid in the development of flexible strategies that maximize therapeutic index and patient benefit.
Conflict of interest
The authors have no potential conflict of interest
References
- Loehrer PJ, Powell ME, Cardenes HR, et al. A randomized phase III study of gemcitabine in combination with radiation therapy versus gemcitabine alone in patients with localized, unresectable pancreatic cancer: e4201 [abstract]. J Clin Oncol 26, a4506 (2008).
- Heinemann V, Labianca R, Hinke A, et al. Increased survival using platinum analog combined with gemcitabine as compared to single-agent gemcitabine in advanced pancreatic cancer: pooled analysis of two randomized trials, the GERCOR/GISCAD intergroup study and a German multicenter study. Ann Oncol. 2007 Oct;18(10):1652-9. Epub 2007 Jul 28.
- Huguet F, André T, Hammel P, et al. Impact of chemoradiotherapy after disease control with chemotherapy in locally advanced pancreatic adenocarcinoma in GERCOR phase II and III studies. J Clin Oncol 2007 Jan 20;25(3):326-31.
- Bloomston M, Marsh C, Walker J, et al. Phase I trial of genemediated cytotoxic immunotherapy in combination with chemoradiation for locally advanced pancreatic cancer. J Clin Oncol 2011; 29(Suppl. 4):Abstract 195.
- Czito BG, Willett C, Kennedy-Newton P, et al. A phase I study of erlotinib, bevacizumab, and external beam radiation therapy (RT) for patients with localized pancreatic carcinoma (PC). J Clin Oncol 2011; 29(Suppl. 4):Abstract 281.
- Moore MJ, Goldstein D, Hamm J, et al. Erlotinib plus gemcitabine compared to gemcitabine alone in patients with advanced pancreatic cancer. A phase III trial of the National Cancer Institute of Canada Clinical Trials Group (NCIC-CTG). J Clin Oncol 2005; 23(16S part I). Abstract No: 1.
- Chang, K. J. Fisher W, Kenady D, et al. Multicenter randomized controlled phase III clinical trial using TN Ferade (TNF) with chemoradiation (CRT) in patients with locally advanced pancreatic cancer (LAPC): Interim analysis (IA) of overall survival (OS) [abstract]. J Clin Oncol 2009; 27, Abstract 4605.
- Sudo K, Yamaguchi T, Ishihara T, Nakamura K, Hara T, Denda T, Tawada K, Imagumbai T, Araki H, Sakai M, Hatano K, Kawakami H, Uno T, Ito H, Yokosuka O. Phase II Study of Oral S-1 and Concurrent Radiotherapy in Patients with Unresectable Locally Advanced Pancreatic Cancer. Int J Radiat Oncol Biol Phys. 2010 Jun 2.
- Crane CH, Winter K, Regine WF, et al. Phase II study of bevacizumab with concurrent capecitabine and radiation followed by maintenance gemcitabine and bevacizumab for locally advanced pancreatic cancer: Radiation Therapy Oncology Group RTOG 0411. J Clin Oncol 2009 Sep 1;27(25):4096-102.
- Anderson S, Cardenes HR, Akisik F, et al. Phase I study of sorafenib (S) with gemcitabine (G)-based radiotherapy (G-RT) in patients (pts) with locally advanced unresectable pancreatic adenocarcinoma (LAUPC). J Clin Oncol 2010: 28:15s, (suppl; abstr 4139).
- Rich T, Harris J, Abrams R, et al. Phase II study of external irradiation and weekly paclitaxel for nonmetastatic, unresectable pancreatic cancer: RTOG-98-12. Am J Clin Oncol 2004 Feb;27(1):51-6.
- Brunner TB, Geiger M, Grabenbauer GG, et al. Phase I trial of the human immunodeficiency virus protease inhibitor nelfinavir and chemoradiation for locally advanced pancreatic cancer. J Clin Oncol 2008 Jun 1;26(16):2699-706.
- Duffy A, Kortmansky J, Schwartz GK, et al. A phase I study of erlotinib in combination with gemcitabine and radiation in locally advanced, non-operable pancreatic adenocarcinoma. Ann Oncol 2008 Jan;19(1):86-91.
- Crane CH, Varadhachary GR, Javle MM, et al. Multiinstitutional phase II trial of induction cetuximab, gemcitabine, and oxaliplatin, followed by radiotherapy with concurrent capecitabine, and cetuximab, for locally advanced pancreatic adenocarcinoma (LAPC). J Clin Oncol 2010; ASCO Gastrointestinal Cancers Symposium. Abstract No. 132.
- Prakash C, Huang S, Vallabhaneni G, et al. Mechanisms of Enhanced Radiation Response following Epidermal Growth Factor Receptor Signaling Inhibition by Erlotinib (Tarceva). Cancer Res 65: 3328-35, 2005.
- Gorski DH, Beckett MA, Jaskowiak NT, et al. Blockage of the vascular endothelial growth factor stress response increases the antitumor effects of ionizing radiation. Cancer Res 59:3374-3378, 1999.
- Scappaticci FA, Fehrenbacher L, Cartwright T, et al. Surgical Wound Healing Complications in Metastatic Colorectal Cancer Patients Treated with Bevacizumab. J Surg Oncol 2005; 91:173-180.
- Huang J, Robertson JM, Margolis JH, et al. Long-term results of full-dose gemcitabine with radiation therapy compared to 5- fluorouracil with radiation therapy for locally advanced pancreatic cancer. J Clin Oncol 2011; 29(Suppl. 4):Abstract 287.
- Lin C, Kos BM, Sasson AR, et al. A phase II study of neoadjuvant gemcitabine/5-fluorouracil followed by 5- fluorouracil/oxaliplatin concurrent with radiation in patients with locally advanced pancreatic cancer. J Clin Oncol 2011; 29(Suppl. 4):Abstract 259.
- Ioka T, Fukutake N, Ikezawa K, et al. Concurrent chemoradiotherapy with gemcitabine and S-1 for unresectable locally advanced pancreatic adenocarcinoma: A phase I study. J Clin Oncol 2011; 29(Suppl. 4):Abstract 305.
- Kim EJ, Ben-Josef E, Griffith A, et al. Phase II trial of neoadjuvant full-dose gemcitabine, oxaliplatin, and radiation (RT) in patients with resectable (R) or borderline resectable (BR) pancreatic cancer. J Clin Oncol 2011; 29(Suppl. 4):Abstract 239.
- Li CP, Chao Y, Chi KH, et al. Concurrent chemoradiotherapy treatment of locally advanced pancreatic cancer: gemcitabine versus 5-fluorouracil, a randomized controlled study. Int J Radiat Oncol Biol Phys. 2003 Sep 1;57(1):98-104.
- Chauffert B, Mornex F, Bonnetain F, et al. Phase III trial comparing intensive induction chemoradiotherapy (60 Gy, infusional 5-FU and intermittent cisplatin) followed by maintenance gemcitabine with gemcitabine alone for locally advanced unresectable pancreatic cancer. Definitive results of the 2000-01 FFCD/SFRO study. Ann Oncol 19(9): 1592-99, 2008.
- Ioka, T., Nakamura, S., Nishiyama, K. A randomized phase II study of gemcitabine 1000 mg/m2 and concurrent radiotherapy comparing gemcitabine alone for unresectable locally advanced pancreatic adenocarcinoma. Int J Radiat Oncol Biol Phys 2010;78(3, Supplement):S102.
- E. Ben-Josef, K. Griffith, I. R. Francis et al. Phase I radiation dose-escalation trial of intensity-modulated radiotherapy (IMRT) with concurrent fixed dose-rate gemcitabine (FDR-G) for unresectable pancreatic cancer. J Clin Oncol 2009; 27:15s (suppl; abstr 4602).
- Murphy JD, Adusumilli S, Griffith KA, et al. Full-dose gemcitabine and concurrent radiotherapy for unresectable pancreatic cancer. Int. J. Rad Oncol Biol Phys, Vol. 68, No. 3, pp. 801-808, 2008.
- Ishii H, Okada S, Tokuuye K, et al. Protracted 5-fluorouracil infusion with concurrent radiotherapy as a treatment for locally advanced pancreatic carcinoma. Cancer. 1997 Apr 15;79(8):1516-20.
- André T, Balosso J, Louvet C, et al. Combined radiotherapy and chemotherapy (cisplatin and 5-fluorouracil) as palliative treatment for localized unresectable or adjuvant treatment for resected pancreatic adenocarcinoma: results of a feasibility study. Int J Radiat Oncol Biol Phys. 2000 Mar 1;46(4):903-1.1.
- Kornek GV, Schratter-Sehn A, Marczell A, et al. Treatment of unresectable, locally advanced pancreatic adenocarcinoma with combined radiochemotherapy with 5-fluorouracil, leucovorin and cisplatin. Br J Cancer. 2000 Jan;82(1):98-103.
- Boz G, De Paoli A, Innocente R, et al. Radiotherapy and continuous infusion 5-fluorouracil in patients with nonresectable pancreatic carcinoma. Int J Radiat Oncol Biol Phys. 2001 Nov 1;51(3):736-40.
- Crane CH, Antolak JA, Rosen II et al. Phase I study of concomitant gemcitabine and IMRT for patients with unresectable adenocarcinoma of the pancreatic head. Int J Gastrointest Cancer 30(3):123-32, 2001.
- Small W, Jr, Berlin J, Freedman GM, et al. Full-Dose Gemcitabine With Concurrent Radiation Therapy in Patients With Nonmetastatic Pancreatic Cancer: A Multicenter Phase II Trial. J Clin Oncol 26(6): 9427-7, 2008.
- Hosein PJ, Kawamura C, Macintyre J, et al. Pilot study of neoadjuvant FOLFIRINOX in unresectable locally advanced (LA) pancreatic carcinoma (PC). J Clin Oncol 2011; 29(Suppl. 4):Abstract 324.
- Tanaka T, Nishiofuku H, Sho M, et al. Phase I/II study of arterial infusion with 5-fluorouracil combined with systemic gemcitabine for unresectable pancreatic cancer. J Clin Oncol 2011; 29(Suppl. 4):Abstract 307.
- Conroy T, Desseigne F, Ychou M et al. Randomized phase III trial comparing FOLFIRINOX (F: 5FU/leucovorin [LV], irinotecan [I], and oxaliplatin [O]) versus gemcitabine (G) as first-line treatment for metastatic pancreatic adenocarcinoma (MPA): Preplanned interim analysis results of the PRODIGE 4/ACCORD 11 trial. J Clin Oncol 2010; 28:15s,(suppl; abstr 4010).
- Krishnan S, Rana V, Janjan NA, et al. Induction chemotherapy selects patients with locally advanced,unresectable pancreatic cancer for optimal benefit from consolidative chemoradiation therapy. Cancer. 2007 Jul 1;110(1):47-55.

