Keywords
Collective trauma; Mass trauma; Recovery process; Vulnerability; Resiliency
Introduction
Disasters bring devastating impacts to communities across the globe is more than evidenced in recent years. Just over the past 24 months, there were phenomenal increase in the number and geographic spread of terrorist attacks that shocked the international headlines. At the same time, the seemingly unending natural disasters are becoming constant news. Such remarkable frequency and scale of natural and man-made disasters often induce a chain of psychological phenomena that have direct impact on a person’s physiological condition, psychological state, functional capacity, interpersonal relationships, communal involvement and spiritual beliefs. The interconnectedness and the extend of the trauma impact can easily be sidelined by the urgency in first-aids and relief work, which in many ways is then missing a crucial piece in setting the stage for long-term mental health recovery in terms of collective trauma [1].
Disaster Mental Health
The interconnected concept of psychological impact of trauma
From a psychological perspective, the interconnected impact can be understood conceptually as below. Extreme external stimuli of a disaster trigger the sensory input system which activates the neuropsychological information processing [2]. The processed neuropsychological messages elicit a variety of corresponding physiological and emotional reactions that inform both the conscious and unconscious self to adopt different coping skills or defense mechanisms for survival [3]. These patterns of the response style applied by the individuals are likely to affect their ability to access resources from their relational support systems among family and friends, or to recount the sense of identity from communal involvement, or to reconstruct the meaning of their existence and the traumatic disaster itself (Figure 1) [4].
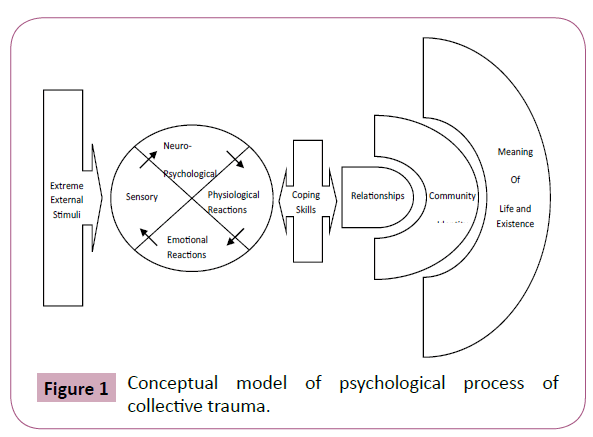
Figure 1: Conceptual model of psychological process of collective trauma.
When an individual is traumatized by a life-threatening experience such as an earthquake, the process of psychological traumatization can be expected. In the event of a trauma, the sensory input system can be overloaded, causing an interruption of the neuropsychological information processing. When neuropsychological information failed to process properly, a variety of corresponding physiological and emotional reactions will be put in a displacement mode [5]. This will directly deplete and affect the victim’s coping ability or defense mechanisms. Thus, the response and motivation to get involved in social and communal activities is diminished, creating a stand of isolation and disconnection [6]. Such patterns of response style inevitably can lead to hopelessness in life and the trauma itself; therefore the victim continues to re-experience the spiral of pain and confusion induced by the traumatic experience.
Responses to trauma exposure
How does the process of psychological traumatization manifest as observable responses? According to the American Academy of Experts in Traumatic Stress Inc. (2004), there are four major areas of symptom list to consider: Physiological, Behavioral, Cognitive and Emotional [7].
Physiological Responses may include rapid heart beats, elevated blood pressure, difficulty breathing, shock symptoms, chest pains, cardiac palpitations, muscle tension and pains, fatigue, fainting, flushed face, pale appearance, chills, cold clammy skin, increased sweating, thirst, dizziness, vertigo, hyperventilation, headaches, grinding of teeth, twitches and gastrointestinal upset.
Behavioral Responses in the face of a traumatic event may include withdrawal, “spacing-out,” non-communication, changes in speech patterns, regressive behaviors, erratic movements, impulsivity, a reluctance to abandon property, seemingly aimless walking, pacing, an inability to sit still, an exaggerated startle response and antisocial behaviors.
Cognitive Responses to traumatic exposure are often reflected in impaired concentration, confusion, disorientation, difficulty in making a decision, a short attention span, suggestibility, vulnerability, forgetfulness, self-blame, blaming others, lowered self-efficacy, thoughts of losing control, hypervigilance, and perseverative [recurring] thoughts of the traumatic event.
Emotional Responses during a traumatic event may include shock, in which the individual may present a highly anxious, active response or perhaps a seemingly stunned, emotionally-numb response. He [or she] may describe feeling as though being “in a fog.” He [or she] may exhibit denial, in which there is an inability to acknowledge the impact of the situation or perhaps, that the situation has occurred. He [or she] may evidence dissociation, in which he [or she] may seem dazed and apathetic, and he [or she] may express feelings of unreality. Other frequently observed acute emotional responses may include panic, fear, intense feelings of aloneness, hopelessness, helplessness, emptiness, uncertainty, horror, terror, anger, hostility, irritability, depression, grief and feelings of guilt. Individual’s experience and expression of traumatization varies. Most will have a few symptoms from the list while others may have recurrent or multitude of symptoms at different times. Another helpful concept to differentiate is shortterm versus long-term psychological impact of trauma. The two corresponding phases are the Intrusive Phase and Denial Phase [8]. Intrusive Phase is an arousal stage. It usually lasts from a few hours to eight weeks and it encompasses most of the immediate responses similar to the above four areas of responses.
Intrusive Phase–hypervigilance, increased startle reaction; intrusive and repetitive thoughts, feelings, and behaviors, difficulties concentrating, emotional liability, sleep and dream disturbances, physical symptoms related to chronic arousal (e.g. nausea, diarrhea, sweating), compulsive repetitions, various forms of self-medication (e.g. alcohol/drugs) along with other activities designed to avoid internal and external triggers.
Although overlapping between the two phases is possible, the long-term impact of trauma can predictably turn into the Denial Phase. This is a phase of avoidance mode. Duration of responses varies and, if left untreated, some symptoms could last a lifetime.
Denial Phase–a host of defensive and distorted mechanisms, including but not limited to, emotional numbing, inability to appreciate significance or internal/external stimuli, avoidance of certain topics/situations, amnesia (partial or complete), constrictive/inflexible thinking, use of fantasy to counteract reality, sleep disturbances, physical complaints (e.g. bowel problems, fatigue, headaches, hyperarousal), impulsivity, over activity, social isolation, self-blame, phobic responses, depression, anxiety, diminished self-care, foreshortened sense of future, re-enactment (of original trauma in play, at work or at home), along with continued substance abuse.
Primary versus secondary trauma
The short-term response mentioned earlier is commonly referred to as Primary Trauma, which is not only observable among victims of traumatic experience. Similar responses are reported among individuals who are indirectly exposed to a traumatic event. These individuals also internalize the victims’ devastating experience, leading to a phenomenon called Secondary Trauma or Vicarious Trauma [9]. Family members of disaster victims are often identified as possible candidates of Secondary Trauma. Obviously, their emotional connection and involvement with the changed life of the victims can deeply affect their mental and emotional states. On the other hand, rescue workers, relief aids, medical staff, debriefing personnel, caretakers, cleanup teams, and witnesses are also at substantial risks. One cannot be close to trauma work without being affected. Unaware, they may be traumatized during the process of witnessing and helping victims. The immense pressure of rescue and providing urgent relief by itself is psychologically demanding. Adding to it the breaking factor of time, in the form of prolonged state of crisis response mode or increased time exposure to the event, the likelihood of experiencing Secondary Trauma is increased [10].
Retraumatization
Retraumatization for natural disaster victims often happens unavoidably. Conditions that echo the same immediate threat to one’s basic survival or conditions that evoke similar physiological or psychological states one just experienced in a traumatic event are likely to trigger Retraumatization [11]. In the case of largescale earthquakes, that can come in the form of earthquake aftershocks, less than satisfactory temporary living arrangement, casualties due to hygiene and weather conditions, or prolonged stay at crumbled and disastrous environment. Moreover, it is noted that merely repeated images of the traumatic event via the media can elicit retraumatization responses among victims, witnesses and related individuals.
Multitude of losses
Within seconds, lives are changed forever - the demise of loved ones, the destruction of homes and communities, the disappearing of possessions and means of income, the loss of irreplaceable memories and one’s sense of control in life, and the crumbling of hope and sense of security. Trying to survive the multitude of losses in a natural disaster is a seemly insurmountable task by itself [12]. To deal with the process of grieving, it is helpful to understand the natural psychological responses that an average person will experience when faced with an immense loss. The five interchangeable stages of dealing with losses after the initial shock are Denial, Anger, Bargaining or Guilt, Depression, and Acceptance. These stages were identified and named by the well recognized Dr. Elizabeth [13]. The stages are briefly summarized below:
1. Denial is generally the first stage of grieving. It can be experienced as numbness, avoidance, isolation or direct denial. It is a stage in which the individual simply cannot believe that the loss took place. The reality does not seem to comprehend mentally. For many people, denial may manifest by simply doing what they would in their normal routines or they may act in such a way that minimizes the event’s impact as if nothing has happened. For some, denial is in the form of going into seclusion or refusing any contacts that can confirm the reality of the loss. Yet some others may seek substances such as alcohol and drugs to numb their pain.
2. Anger is a typical response of grieving for losses. Overwhelming feelings of unfairness, abandonment and powerlessness related to the loss are expressed outwardly with the attempt to regain certainty and control. The angry emotion may be directed to self, loved ones or even the deceased at times. In other cases, anger is projected out onto outsiders, events or institutions, usually in a manner familiar to the individual.
3. Bargaining or Guilt is a stage in which people try to come up with ways to get back what was lost, sometimes in the form of blaming. Common thoughts include "If only I had just …." or "Maybe if I do this now, then …" Survivor’s guilt is often observed in working with family members of the victim. Some survivors feel guilty for surviving and may have recurring thoughts about how they too should have perished with the victims or if they could somehow take their places instead. For many, guilt can further power yet other self-defeating behaviors while some can turn guilt into constructive forces or movements.
4. Depression stage occurs when one feels overwhelmingly helpless and hopeless about the loss. The realty of having to go on with life without a loved one begins to sink in. Withdrawal, isolation or crying spells are typical ways one expresses sadness. Disruption of routine cycle of sleeping and eating is common. Depression is quite a consuming stage to undergo and, in some cases, professional help is needed.
5. Acceptance is considered the last stage. It is a stage of reflection and reorganization. Life is taking on a new routine by incorporating the loss. The individual can still be sad about the loss at times, but the sadness does not keep the individual from normal functioning. Given time, the intensity of the sadness may generally decrease but may never entirely go away.
Grief is a unique process. Although typical among most people, for some, the process may have a very different order. The intensity and duration of each listed stage may also vary greatly from one person to another. Matters become more complicated when the losses are multi-folded while the strained relief programs provide limited resources that one can access.
A Framework of Understanding the Process of Recovery from Collective Trauma
From a clinical perspective in psychology, trauma results from natural disasters can be understood as the deepest challenge to one’s core existence trapped in time. The sense of helplessness and vulnerability is core in the process of psychological healing. As a society, it is extremely important to acknowledge the fact that there are numerous ways people express and manage their sense of helplessness and vulnerability. It is particularly true when the reality of struggling for basic survival in the aftermath can dissociate one’s trauma response and grieving process from the actual disastrous experience. For some, their automatic survival mode can give a false sense of resiliency in their recovery process. However, human’s natural ability to strive, adapt and rebound is undeniably powerful. With every toxic plant the nature presents, there is always an antidote nearby [Chinese proverbs]. The belief that individuals have within themselves the ability to heal is shared by many in the mental health profession who had a chance to witness the process of healing in the face of adversity. Rightly so, resiliency is an increasingly validate concept in trauma studies and in positive psychology [14]. Individuals who are able to rebound from traumatic experience are expected to respond to the process of traumatization differently, referred here as the resiliency process.
Resiliency Process
Pulling from accumulated field experiences and observations of over 20 years of clinical work, an effort to articulate a phase-wise resiliency process is offered by the author here. When extreme external stimuli trigger the collection of sensory inputs and activate neuropsychological information processing and organization, vital mental processes can kick start the protective physiological and emotional reactions, identified in this preliminary framework as the: 1) Organizing, 2) Acknowledging, and 3) Expressing. Correspondingly, when a person reaches the Coping Skills phase, the recurring healing activities are: 1) Adapting, and 2) Learning to live with the multitude of losses. In turn, when coping skills are gaining grounds for individual, relational support systems can play a significant role at this stage. Organized resources will be better utilized if they offered under the principles of: 1) Accessing, 2) Affirming, and 3) Reconnecting. When the sense of one’s post-trauma identity can be affirmed and reconnected, for some survivors the quest of explanation of life events or disrupted values about world orders may eventually surface, sometimes even years afterwards. The natural quest of making existential meaning out of the seemingly impossible situation of rebuilding one’s life is a continuous effort of regaining and/or redefining the sense of psychological safety and predictability. This intrapersonal or arguably existential quest proposed in this framework includes: 1) Reviewing, 2) Exploring, and 3) Transforming about the meaning of one’s core existence can be expected (Figure 2).
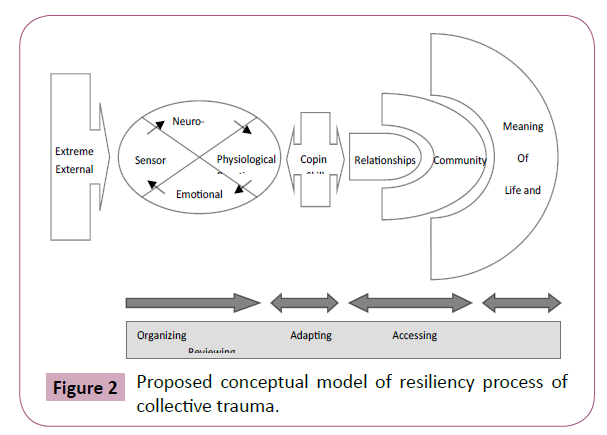
Figure 2: Proposed conceptual model of resiliency process of collective trauma.
Conclusion
The key concept of trauma recovery lies in the recognition of a parallel process between vulnerability and resiliency. Grieving takes time. Grieving for a collective trauma takes time, organization, and vision. Understanding how to respect the grieving process and foster the sense of hope is the first step for organizing and rebuilding a community. There is both a need to respectfully acknowledge the on-going burden of living without loved ones or the familiar ways of life and to thoughtfully foster new ways of building on the communal strengths of the survivors. There is a need to cry and a need to fly. One can neither keep on mourning about the past indefinitely nor can one create a future without looking back at the past from time to time. Most survivors of trauma will come to make senses out of the recovery process–the pain never completely goes away, it gets to be part of life. There are days when life can be too much to handle, even the smallest steps seem impossible. Other times, the pain puts perspectives in life and makes it more meaningful to keep on trying.
Community’s acceptance, education and expectation about the recovery process are crucial in setting the stage for collective healing [15]. While the focus of rebuilding one’s life from the aftermath taps on people’s resiliency, it cannot be the only focus. It is equally fruitful to focus on the shared expression and acknowledgment that lives were changed and it is painful still. Above all, the conclusive lesson that the author is humbly sharing here: Being weak is strong, being strong is weak, and being both is needed. In other words, recovery from the majority of large-scale devastating psychological trauma requires the society’s collective sense of being able to integrate the simultaneous process of expressing vulnerability while fostering resiliency. When planning and developing aftercare supportive services, the parallel healing psychological process–living respectfully with vulnerability and hopefully with resiliency–is the guiding principle for clinicians, researchers and policy makers alike.
References
- Paganini M, Borrelli F, Cattani J, Ragazzoni L, Djalali A, et al. (2016) Assessment of disaster preparedness among emergency departments in Italian hospitals: a cautious warning for disaster risk reduction and management capacity. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 24: 101.
- Bromet EJ, Atwoli L, Kawakami N, Navarro-Mateu F, Piotrowski P, et al. (2017) Post-traumatic stress disorder associated with natural and human-made disasters in the World mental health surveys. Psychol Med 47: 227-241.
- Ochi S, Murray V, Hodgson S (2013) The great east Japan earthquake disaster: a compilation of published literature on health needs and relief activities, march 2011-september 2012. PLoS Curr 13: 5.
- Updegraff JA, Silver RC, Holman EA (2008) Searching for and finding meaning in collective trauma: results from a national longitudinal study of the 9/11 terrorist attacks. J Pers Soc Psychol 95: 709-722.
- Van der Kolk B (2000) Posttraumatic stress disorder and the nature of trauma. Dialogues Clin Neurosci 2: 7-22.
- Goodkind JR, Hess JM, Gorman B, Parker DP (2012) “We’re still in a struggle”: dine resilience, survival, historical trauma, and healing. Qual Health Res 22: 1019-1036.
- https://www.universitycrisisresponse.com/
- Grant R (1996) The way of the wound: a spiritual trauma and transformation. The Way of the Wound: A Spirituality of Trauma and Transformation Paperback.
- Kessler RC, McLaughlin KA, Koenen KC, Petukhova M, Hill ED, et al. (2012) The importance of secondary trauma exposure for post-disaster mental disorder. Epidemiol Psychiatr Sci 21: 35-45.
- Atkins CD, Burnett HJ (2016) Specialized disaster behavioral health training: Its connection with response, practice, trauma health, and resilience. DisHealth 3: 57-65.
- Fetter JC (2005) Psychosocial response to mass casualty terrorism: guidelines for physicians. Prim Care Companion J Clin Psychiatry 7: 49-52.
- Ushizawa H, Foxwell AR, Bice S, Matsui T, Ueki Y, et al. (2013) Needs for disaster medicine: lessons from the field of the Great East Japan Earthquake. WPSAR 4: 51-55.
- Kübler-Ross E, Kessler D (2007) On grief and grieving: finding the meaning of grief through the five stages of loss. 98: 980-981.
- Bleich A, Gelkopf M, Melamed Y, Solomon Z (2006) Mental health and resiliency following 44 months of terrorism: a survey of an Israeli national representative sample. BMC Med 4: 21.
- Reifels L, Pietrantoni L, Prati G, Kim Y, Kilpatrick DG, et al. (2013) Lessons learned about psychosocial responses to disaster and mass trauma: an international perspective. Eur J Psychotraumatol 4: 10.

