Welcome to volume 12 of Diversity and Equality in Health
and Care. There really will be more Diversity – we have had our
time on the brink, and have survived. As our regular readers will
know, our journal was sold by Radcliffe Medical in 2014, and
we are now published by iMedPub, an India-owned publisher.
If we do truly love diversity and endorse it, then we should
welcome change. There will be teething problems – ‘Change is
never achieved without difficulty, even from worse to better’,
as Richard Hooker (theologian, 1554-1600, or was it the diarist
Dr Johnson?) once remarked. We hope that our readers old and
new will find that our standards have remained as high as ever,
and that our value in presenting new evidence, challenging
orthodoxy and speaking ‘truth to power’, has not diminished.
Our new website is at https://diversityhealthcare.imedpub.
com/ where you will find our guidance for authors, our current
call for papers and recent papers. The transfer to new ownership
has brought a lot of changes, the most notable of which is that
Diversity and Equality in Health and Care is now an Open
Access journal, which does mean that authors will have pay
a fee once their papers have been accepted for publication.
Open Access provides free and unrestricted on-line access to
research papers for researchers, students, teachers, practitioners
and others across the world and thus contributes to the timely
sharing of knowledge, the development of best practice and
to communities of discourse. The problem, as with the British
NHS, is that we are now ‘free at the point of use’ – but (as in
1948 in UK, and under “ObamaCare” in the USA) someone has
to pay somehow for the costs. Moving those to the sponsors
of research seems one logical way forward, since if they are
prepared to pay researchers to conduct studies, they must have
a vested interest in those results reaching the widest possible
audience. Open access does also mean, of course, that the
papers get a much wider readership and have, potentially,
greater impact! Papers are published under Creative Commons
Attribution License and may be copied and used by anyone
providing the original work and source is appropriately cited’
(https://diversityhealthcare.imedpub.com/).
Open Access has the potential to improve health and care
practice for the benefit of patients and clients. Professional
preparation and continuing professional development can be
enriched by the latest research findings. Researchers themselves
may also benefit through increases in both the impact of
their work and the number of citations it attracts. Individuals
no longer have to depend on their libraries to subscribe to a
particular journal nor do they have to buy it themselves unless
they particularly need to. Open Access is also of benefit to tax payers. A great deal of research is paid for out of public funds
but, aside from those who are prepared to pursue the matter,
tax payers have had little formal access to published results. In
this context science becomes disconnected from society, insular
and preoccupied with its own arcane concerns. Society too may
become uninterested in a topic it sees as having nothing to do
with everyday life or regard science with suspicion and distrust.
Equally, health charities have an interest in ensuring that work
they have sponsored researchers to conduct gets the widest
possible readership, and is shown to achieve the highest levels
of peer approval. This conclusion has been embraced by many
large ‘Third sector’ organisations, who are prepared to pay the
fees to ensure that their work is widely reported and used.
Open Access enables the public to see the outcomes of
research and contributes to the democratisation of knowledge,
particularly knowledge about science, which is consistent with
broader policies to engage a wider range of people. An example
of such policies is the European Commission’s (2001) Science
and Society Action Plan which provided a common strategy
to improve scientific understanding among the populations
of member states by, for example, improving the teaching of
science in schools, facilitating public debate and encouraging
a wider range of perspectives in science, especially those of
women. The aim was to facilitate the development of more
scientifically-literate populations in which the creative energies
of those previously disconnected from science could be used
to breathe new life into innovation and foster research in new
or under-addressed fields. The Framework Programme has
facilitated the implementation of this policy and led gradually
from a perspective of science and society to science with and
for society (European Commission 2014 https://ec.europa.eu/
research/swafs/index.cfm?pg=home). Public engagement is
essential in bringing scientists and non-scientists together, as
equals who respect each other’s knowledge and expertise and
who have access to the same resources.
We hope that our move to Open Access will continue to
contribute to discourses about diversity and equality but we
also acknowledge that the change has not been easy and there
are still some transitional issues that need to be addressed and
we plan some changes and to develop new resources and ways
of enabling you, our readers, to engage with the community of
scholars over the coming year. Nevertheless, we will continue
to maintain high standards in reviewing and presenting papers
which challenge prevailing orthodoxies and injustices. We
continue to welcome papers relating to all aspects of diversity
and equality in health and care. We particularly encourage multi-professional perspectives and attention to the views of service users and carers, and papers exploring the international dimensions of diversity and equality across and within cultures. We continue to adhere to the code of practice of COPE, The Committee for Publication Ethics in Medical Journals, and encourage authors to follow the guidelines of CLAS (in the USA) and others regarding the use of appropriate language. Detailed advice about presentation can be found at https://imedpub.com/. Papers may
• report on qualitative or quantitative research
• describe and evaluate good practice or service provision
• put forward arguments for debate
• discuss educational issues.
We recognise the potential disadvantages of Open Access although at present we can offer no solutions. On-line publication may be problematic for some people. Older adults and those with sensory impairments who are not yet trained and supported in the new technologies may miss out of key advice and opportunities (International Longevity Centre UK (ILC-UK, 2015, https://www.ilcuk.org.uk/). Across Europe, those who are disadvantaged in terms of ‘race’, ethnicity, religion or faith, age, sex or gender, sexual orientation, migrant status or disability, are further hindered in their quest for equality and justice by inequalities and injustices in the availability of information and their access to new technology. Equality and Diversity as a discipline addresses all areas of exclusion and inequality, and reveals that this approach has benefits for all in the health and care field. A recent report suggests, for example, that the question of gender-inequality still needs to be addressed, and that the lessons learned during the Thalidomide scandal were poorly learned. It is, for example, being recognised that the signs of a heart attack – notably, elevated levels of a hormone (Troponin), differ between men and women, with much lower levels indicating a significant risk among women (Shah et al 2015). In other words, sauce for the goose is definitely not sauce for the gander, and one should apply different rules or even different tests to establish risk for different groups, whether defined by gender (as here) or ethnicity, as is the case in respect of body mass index and diabetes (Chiu 2011). As we may have said before, cultural competence is not just about being ‘nice’ to people who we might define as ‘other’, but remains a real safety issue that is, or should be, central to fitness to practice.
Equality and diversity are expanding concepts as society becomes more aware of the increasing number of ways in which individuals are excluded. Moreover, it is increasingly recognised that multiple diversity and exclusions are possible through the intersectionality of protected characteristics (Bowleg 2012, Vertovec 2007), although we might argue that this journal in its former guise as Diversity in Health & Social Care, and its ‘mission statement’ first published as early as 2004 was slightly in advance of this recognition, and hopefully has helped to spearhead it!.
We know that some authors may be discouraged by Open Access: those at the start of their careers and those who pursue a lonely research path investigating the margins of their societies or unfashionable, neglected subjects. We have published many papers of this kind in our previous volumes and we hope to continue doing so. We encourage researchers to factor the cost of Open Access into applications for research funding. Others may have to approach their universities or employers to cover costs. However, if all other avenues fail we will do our best to help and advise where we can: in exceptional circumstances, our publishers may agree to a discount or waiver! Please contact us to discuss your ideas at Paula McGee (paula.mcgee@bcu.ac.uk) or Mark Johnson (mrdj@dmu.ac.uk).
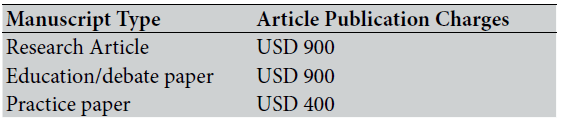
Open Access fees
In this issue
We begin our first Open Access issue with two guest editorials on controversial topics. Jo Samanta, an expert on medical law and ethics, presents a carefully argued discussion of the new rules regarding assisted dying for children in Belgium. This is a hugely emotive issue, and it is likely that there cannot be a single right answer for all cases, even if strong moral arguments rage on both sides. We hope that our readers will read, consider, and react and in so doing, please cite the source of your provocation. Equally controversial but in a different field, is Harshad Keval’s stance on a recent report about psychosis and schizophrenia issued by the British Psychological Society. Whilst highly commendable in explaining voice hearing and the importance of de-stigmatising severe mental health problems, the report neglects to say anything about black and other minority ethnic people who, in Western health care systems such as the UK, are more likely than their white counterparts to be diagnosed with psychosis or schizophrenia. Black people in particular have repeatedly reported negative experiences of health care, institutional racism, lack of cultural understanding among practitioners and many other problems. The report has ignored all of them.
Minority ethnic health features throughout this issue. In our research section we present two papers from well-established contributors to our pages. First, Geeta Patel and colleagues provide a useful extension to the small literature on the patient experiences of minority ethnic groups in the cancer pathways. For the first time, we can read the stories of low English proficiency (LEP, or Non-English Speaking Background) South Asian women living with breast cancer. Their evidence powerfully underscores the importance of language in the provision of culturally competent care and support.
Iraj Poureslami and colleagues report from Canada where multiculturalism has been a relatively new phenomenon beyond the interfaces between First Nation and Settler descendants and between English and French speaking populations. About 20% of migrants in Canada are Chinese and, like many first generation migrant populations the world over, they tend to live in specific areas, creating a home from home in which Mandarin and Cantonese, are most commonly spoken languages. Many aspects of their health and care needs are under-researched and they are disadvantaged further by lack of access to health information tailored to their needs. Poureslami at al.’s papers
paper provides a welcome insight into beliefs about smoking
and respiratory disease in the wake of deliberate targeting by
tobacco companies in China.
We carry, as usual, our selection of features that we hope
will prove attractive and informative. The Practitioners Blog
concerns a matter that has great potential to affect the lives of
black and other minority ethnic people. Inequalities in organ
and other cell donation, including blood and gametes, are well
established, and have traditionally been blamed on cultural
factors. Mary Dawood and David Crichton show that real
problem is lack of cultural competence among the professional
workforce or fear of giving offence. Organ donation for black
and other minority ethnic people is so important that we have
devoted our CPD feature to this issue in order to facilitate
debate and a learning process. To this we add, as ever, our
Knowledgeshare feature, for the first time open to all readers in
the Open Access process.
References
- Bowleg L 2012 ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âThe problem with the phrase women and minorities: intersectionality ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â an important theoretical framework for public healthÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ American Jnl Public Health 102, 7:1267-1273
- Chiu M, Austin PC, Manuel DG, Shah BR, Tu JV ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¦Ã¢â¬ÅDeriving ethnic-specific BMI cutoff points for assessing diabetes riskÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡ÃâàDiabetes Care 34,8 :1741-1748
- European Commission (2001) Science and Society Action Plan, Luxemburg, Office of the Official Publications of the European Communities.
- Keval H, 2015 ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âSchizophrenia and psychosis: the magical and troubling disappearance of race from the debateÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ Guest editorial Diversity and Equality in Health and Care 12: 6-8
- International Longevity Centre-UK 2015 Next Generation Health Consumers: The changing face of health seeking behaviour across Europe London: International Centre for Longevity www.ilcuk.org.uk (accessed 5 March 2015).
- Patel-Kerai G, Harcourt D, Rumsey N, Naqvi H 2015 ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¦Ã¢â¬ÅExploring the lived experience of breast cancer diagnosis and treatment amongst Gujarati-speaking Indian womenÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡ÃâàDiversity and Equality in Health and Care 12 12: 9-17
- Poureslami I, Shum J, FitzGerald M 2015 ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¦Ã¢â¬ÅWhy do Chinese people with COPD continue smoking: the attitudes and beliefs of Chinese residents of Vancouver, CanadaÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡ÃâàDiversity and Equality in Health and Care 12: 18-27
- Samanta J 2015 ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âChildren and euthanasia: BelgiumÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s controversial new lawÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ Guest editorial Diversity and Equality in Health and Care 12: 4-5
- Shah ASV, Griffiths M, Lee KK, McAllister DA, Hunter AL et al 2015 ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¦Ã¢â¬ÅHigh sensitivity cardiac troponin and the underdiagnosis of myocardial infarction in women: Prospective cohort studyÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡ÃâàBMJ 350:g7873 https://dx.doi. org/10.1136/bmj.g7873
- Vertovec S 2007 ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âSuper-diversity and its implicationsÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ Ethnic and Racial Studies 30,6 :1024-1054

