Keywords
Fluoroscopy time; Trainee competency; Transradial; Transfemoral
Introduction
The transradial (TR) approach is increasingly being used as the default access for coronary angiography. National cardiac governing bodies, such as the Cardiac Society of Australia and New Zealand, assess competency by requiring trainees to perform minimum angiography case numbers throughout their training [1]. There are no guidelines, however, to the minimum number of TR cases a trainee should complete, neither are there standardized tools for the assessment of proficiency in coronary angiography by the end of three years of cardiology training.
Fluoroscopy time (FT) has been suggested as an objective measure of proficiency where a decrement in FT time indicates increasing competency [2]. As expected, trainees have been shown to have, in general, longer FT as compared with their supervisors [3,4]. However, it is unknown if cardiology trainees improve their efficiency in performing coronary angiography particularly in the first few years of training. In addition, although there is a learning curve of operators new to TR angiography, there is limited data on the difference in FT of trainees performing TR and TF angiography
The aims of this study are to: (i) establish if a difference in FT exists between supervisors and trainees, (ii) investigate if trainees have shorter FT with increasing seniority, (iii) compare FT of cardiology trainees between TR and TF approaches, and (iv) determine a minimum number of TR cases to overcome any potential “learning curve”.
Methods
The FT in patients undergoing coronary angiography (with left ventriculography) was assessed at the University Hospital Geelong, a single tertiary referral center, from February 2010 to January 2014. Assessment was restricted to cases performed in the outpatient/ambulatory or elective cardiac catheterization laboratory. TF or TR approaches were performed as per cardiologists’ preference.
Study design and protocol
The dates of this study were chosen to capture the entire 24-month tenure of eight individual cardiology advanced trainees. Trainees were supervised by 7 cardiologists, of which two were general cardiologists highly experienced in TF coronary angiography and five interventional cardiologists deemed experienced in both TF and TR angiography as per the ESC consensus document [5]. TF and TR cases were dichotomized to with trainee (trainee) or without trainee (consultant) present in the catheterization laboratory. A cardiologist was all present and supervised all cases performed. FT was collected in all cases and expressed in minutes. Each trainee performed a median of 49 (IQR: 21 – 97) TR and 55 (IQR 27 – 96) TF cases in each year of training thus arbitrarily fifty cases were chosen as a cut-off to assess for improvement in FT.
Complex cases (coronary artery bypass graft studies, ad hoc percutaneous coronary intervention, fractional flow reserve and right heart studies) were excluded. Trainee attendances at cases performed in the in-patient or acute catheterization laboratory were not included in this study, as a proportion of cases proceeded to coronary intervention.
Statistical analysis
Non-normally distributed continuous variables are reported as a median with the interquartile range (IQR) in square parenthesis and compared using non-parametric tests. Categorical variables are reported as n (%) and analysed using Chi-square, Fisher test, Kruskal-Wallis test or Wilcoxon rank sum test where appropriate. Variables with an alpha significance level of 0.05 were considered significant. Statistical analysis was performed using the R statistical package, version 3.2.5, Vienna, Austria.
Results
1,699 patients underwent outpatient coronary angiography during the study period. Of these, 425 complex cases were excluded leaving a study total of 1274 patient who had coronary angiography with left ventriculography. A trainee was present (trainee) in 707 (55.5%) and absent (consultant) in 567 (44.5%) cases.
Baseline characteristics of the patients undergoing outpatient coronary angiography are shown. Although patients in the trainee cohort were older (70.0 vs 65.0 years, p-value=0.01), there was no statistically significant difference in gender, height, weight or body mass index (BMI). In addition, trainees did less radial and more femoral cases than consultants (47.4 vs 57.5% and 52.6 vs 42.5%, p-value <0.0004). TF had a 100% procedural success rate, whilst there was a TR to TF conversion rate of 5.5%. Over the 4 years of the study, there were an increasing number of TR cases performed (41.2 vs 47.2 vs 52.0 vs 68.4, p-value<0.001), with a corresponding decline in the number of TF cases.
Fluoroscopy times
The median overall fluoroscopy times across both groups during the study period was 5.0 minutes [IQR 3.4 – 7.4]. The FT in both trainee and consultant cases improved over the duration of the study, with a median FT of 6.3 minutes in 2010 versus a FT of 4.7 in 2013. TR cases took longer to complete than TF cases (5.7 vs 4.6 minutes, p-value <0.001). Comparing consultant and trainee cases, the presence of a trainee during the case affected the FT. The total, TR and TF FT in trainee cases was longer than that in consultant cases (Figures 1-3).
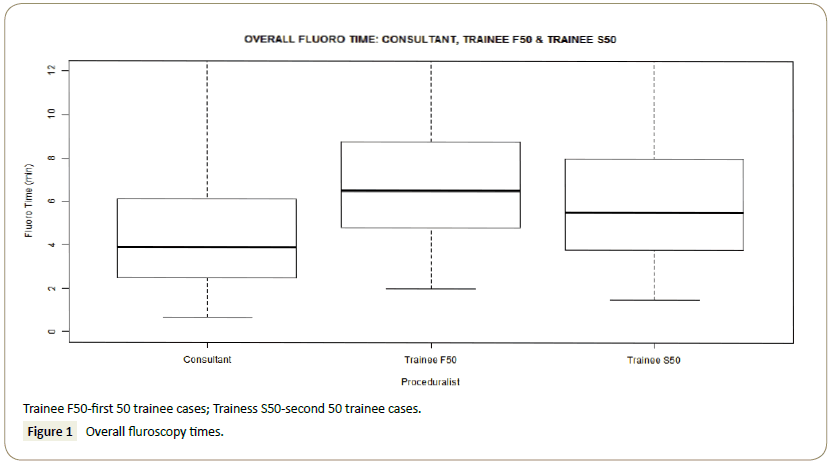
Figure 1: Overall fluroscopy times.
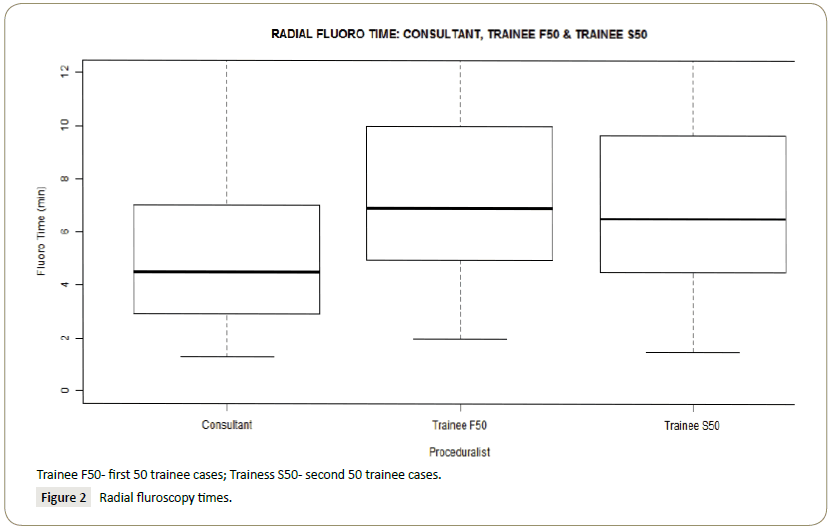
Figure 2: Radial fluroscopy times.
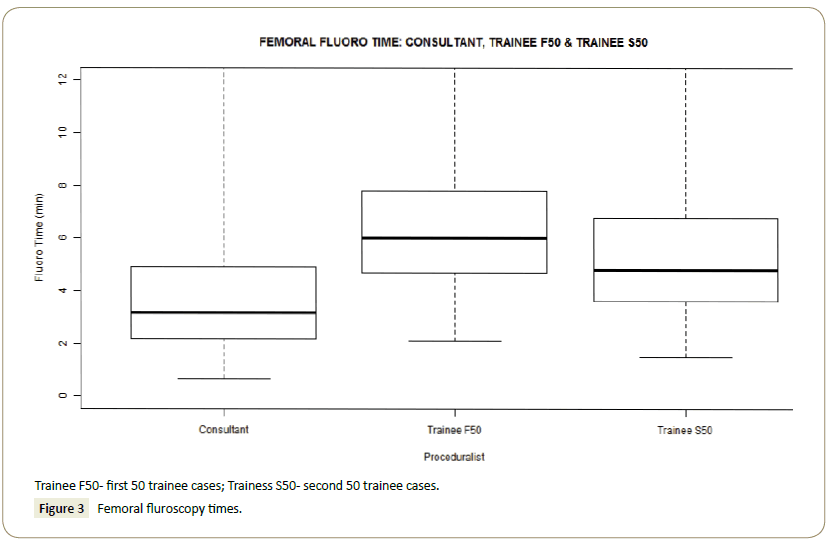
Figure 3: Femoral fluroscopy times.
Among trainee cases, the median total FT improved with increasing seniority and between their first fifty versus the second fifty cases (6.5 mins vs 5.2 mins, p-value<0.0001). A similar improvement was seen when cases were separated into radial and femoral cases (7.1 mins to 6.1 mins, p-value 0.00015 for TR and 5.9 mins to 4.7 mins, p-value<0.0001 for TF) (Figure 4). When compared to consultants, the median FT of trainees fell within the 75% quartile of their supervisors in their second year. The total, radial and femoral median FT of consultants, first year trainees and second year trainees are depicted.
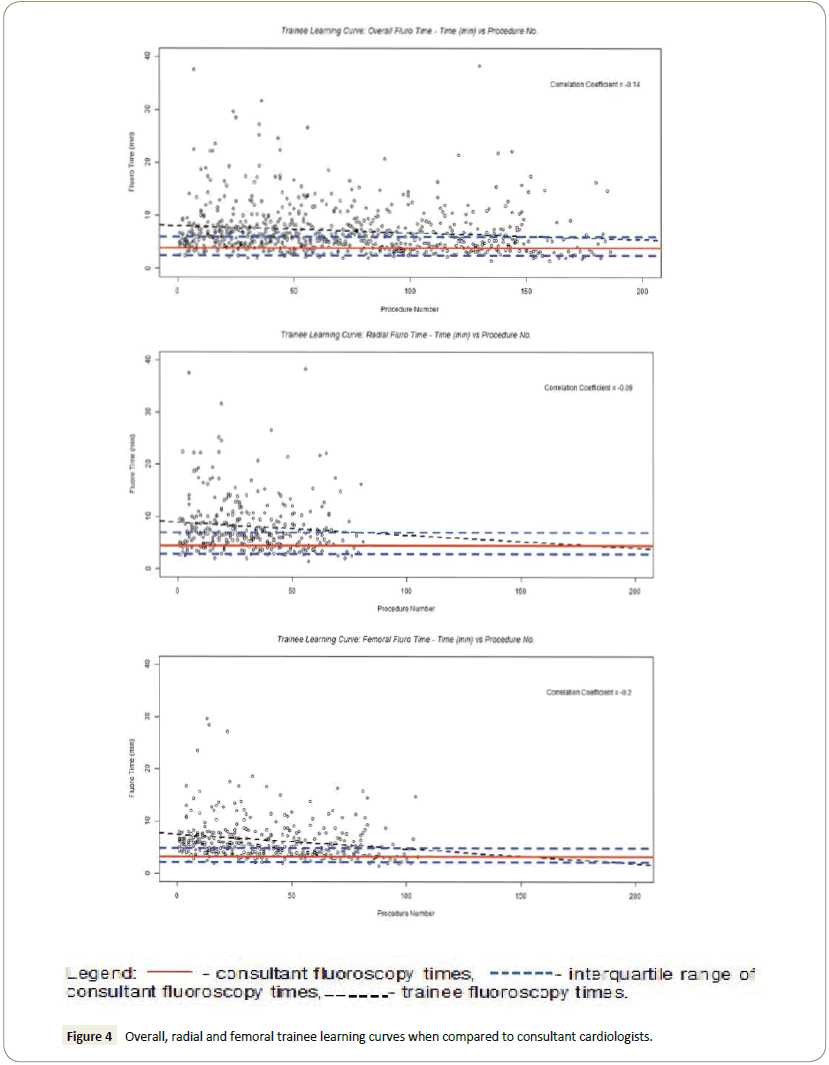
Figure 4: Overall, radial and femoral trainee learning curves when compared to consultant cardiologists.
Using these results, we derived scatter plots to evaluate trainee FT against procedure number, to try to identify trainee “learning curves” for overall, transradial and transfemoral angiography. Trainee FTs appear to decrease with increasing procedure numbers, and this applies for all means of coronary angiography. However, the coefficient correlations for all three scatter plots were not statistically significant, limited by the small sample size.
Discussion
In this study, we have demonstrated that cardiology trainees took longer to perform diagnostic coronary angiography than their supervisors. The transradial approach was associated with longer FT, however with increasing experience, trainees were able to decrease this in both transfemoral and transradial approaches. After fifty supervised cases, there was a discernible improvement in total, TF and TR efficiency.
Trainee inexperience has been found to be associated with longer procedure times as assessed by fluoroscopy time [3,4]. Jensen et al determined a caseload of 150 coronary angiographies to obtain competency - defined as a median fluoroscopy time within the IQR of an expert [2]. All trainees in our study had no prior experience with coronary angiography prior to entering into cardiology training. In their first year of training, the trainees’ overall-FT, TR-FT and TF-FT were consistently outside the thirdquartile of the supervisors FT. In their second year, median FT was all within the 50% to 75% interquartile range thus attaining competency as per Jensen’s definition. Although this competency was not consistently met just after 50 cases, at this “cut-off”, a statistically significant improvement in FT was achieved. This is in keeping with the thirty to 150 cases that has been described as the “learning curve” in the transradial approach: 30 to 50 for TF interventional cardiologist to attain TR proficiency [6,7], over 50 cases as per the ESC consensus [5] and as high as 100-150 in certain operators [7].
A caseload-based system of training to attain TR proficiency is likely more fruitful than a time-based system. Castles et al. [8] found a 6-month introductory phase to introduce TR to the catheterization laboratory to have no improvement in FT; likely due to low case numbers (109 cases in 6 months across five experienced cardiologists). Conversely, Looi et al. [9] found that a six-month learning curve to be sufficient in decreasing FT in nonexperienced radial operators with a relatively similar caseload (36 procedures per operator in the first 9 months). A potential for the difference in the findings may be related to each centre’s different experience in TR procedures. Vlachadis Castle study was undertaken at a center in the early phase of establishing a TR program with only one TR expert and 4 non-experts, versus in Looi’s center of 3 experts to 5 non-experts. The role of a transradial proctor to help establish TR in a traditional TF center has its appeals, however has never been studied. In our center, the presence of five transradial “experts” may have helped our trainees improve their TR proficiency more quickly.
Study Limitations
There are several limitations to this study. It is a retrospective, single centre study where the accuracy is dependent on the proper documentation of each procedure. Trainees may have gained some experience in the in-patient catheterization laboratory and so the minimum number of cases required demonstrating equivalence to consultant times may be underestimated. We used fluoroscopy time as a surrogate marker for competence, however no data was collected comparing clinical outcomes or complications. Complication rates for coronary angiography are generally low thus the numbers required to identify a difference are beyond the scope of this study. It is possible that supervisors may intervene at an earlier stage in the beginning of training. This, however, would likely decrease FT in the first 50 cohort and not invalidate our findings that a significant improvement in FT exists.
Conclusion
This study demonstrates that cardiology advance trainees do have longer fluoroscopy times when compared to consultant cardiologists, in overall, radial and femoral cases. However, these times improve over the course of their training. In addition, we have shown an improvement in transradial coronary angiography is feasible in trainees after at least fifty cases at a transradial cardiac center, with appropriate supervision.
References
- The Cardiac Society of Australia and Zealand (2014) Position Statement: Competency in adult diagnostic cardiac catheterisation and coronary angiography.
- Jensen UJ, Lagerquist B, Jensen J, Tornvall P (2012) The use of fluoroscopy to construct learning curves for coronary angiography. Catheter Cardiovasc Interv 80: 564-569.
- Xu BJ, Duszak R, McGinnis RS, Stanfill JG, O'Rear J, et al. (2013) Increased fluoroscopy time for central venous catheter placement by radiology residents versus staff radiologists. J Am Coll Radiol 10: 518-522.
- Soleimani RA, Hsu JC, Han FT, Nguyen N, Kwon M, et al. (2013) Trainee inexperience is associated with longer procedure times but no increase in complications for cardiac device implantation. Heart Rhythm 10: 1755-1758.
- Hamon M, Pristipino C, Mario CD, Nolan J, Ludwig J, et al. (2013) Consensus document on the radial approach in percutaneous cardiovascular interventions: Position paper by the European Association of Percutaneous Cardiovascular Interventions and Working Groups on Acute Cardiac Care** and Thrombosis of the European Society of Cardiology. Euro Intervention 8: 1242-1251.
- Hess CN, Peterson ED, Neely ML, David D, William B, et al. (2014) The learning curve for transradial percutaneous coronary intervention among operators in the United States: A study from the National Cardiovascular Data Registry. Circulation 129: 2277-2286.
- Rao SV, Tremmel JA, Gilchrist IC, Shah PB, Gulati R, et al. (2014) Best practices for transradial angiography and intervention: A consensus statement from the society for cardiovascular angiography and intervention's transradial working group. Catheter Cardiovasc Interv 83: 228-326.
- Castles AV, Asrar UHM, Barlis P, Ponnuthurai FA, Lim CC, et al. (2014) Radiation exposure with the radial approach for diagnostic coronary angiography in a centre previously performing purely the femoral approach. Heart Lung Circ 23: 751-757.
- Looi JL, Cave L, El-Jack S (2011) Learning curve in transradial coronary angiography. Am J Cardiol 108: 1092-1095.

