Keywords
Hemorrhage; Pancreatectomy; Risk Factors
Abbreviations
ISGPS: International Study Group on Pancreatic Surgery; MRSA: methicillin-resistant Staphylococcus aureus; PPH: post-pancreatectomy haemorrhage
INTRODUCTION
The mortality rate after major pancreaticoduodenectomy has decreased considerably over the last few decades and current mortality rates from high volume centres are less than 3% [1, 2]. However, the morbidity from this surgery still remains high, ranging from 20% to 40% [3, 4]. Haemorrhage following pancreaticoduodenectomy (PPH) is infrequent, but is a dramatic complication occurring in the early and late post operative period. Clinically significant haemorrhage is noted in 2% to 8% of cases; it is associated with a significant mortality rate ranging from 18% to 47% and accounts for up to 25% of post operative deaths [5]. Debate still continues around its causes and as to whether its best treatment is by surgery or angiographic embolisation [6, 7]. Several factors have been shown to predispose to PPH including intra-abdominal abscess, pancreatic fistula and bile leaks [8]. Recently, methicillin-resistant Staphylococcus aureus (MRSA) has been implicated in adverse clinical outcomes in patients undergoing upper GI [9] and vascular surgery [10]; however no data is available regarding its impact in patients undergoing pancreaticoduodenectomy. The primary aim of this study was to identify risk factors and prognostic factors for PPH and to report on our results following their management by radiological intervention.
METHODS
All patients who underwent pancreaticoduodenectomy from January 2004 to May 2007 in Ninewells Hospital (Dundee, Scotland) were reviewed. Data were obtained from a prospectively maintained departmental hepatobiliary- pancreatic data base, and included incidence of haemorrhagic complication, interval between pancreaticoduodenectomy and bleeding, site of bleeding, details of its management and outcome, presence of MRSA infection. Neo-adjuvant treatment is not routinely employed in the UK; therefore, no patients received the treatment. Patients’ electronic records were also reviewed retrospectively to identify possible discrepancies.
Definitions
Haemorrhage was defined as postoperative bleeding from the surgical site with a drop in haemoglobin concentration greater than 3 g/dL with peripheral circulatory impairment requiring medical intervention. The definition of PPH used was that proposed by the International Study Group on Pancreatic Surgery (ISGPS), based on the three parameters: onset, location, and severity. The onset is either early (less than 24 hours after the end of the index operation) or late (more than 24 hours). The location is either intraluminal or extraluminal. The severity of bleeding may be either mild or severe. Three different grades of PPH (grades A, B, and C) are defined according to the time of onset, site of bleeding, severity, and clinical impact [11].
Pancreatic fistula was defined by presence of an amylase concentration in the abdominal drains fluid exceeding 3-time serum concentration at any time during the postoperative period. Drain fluid was routinely tested for amylase and sent for culture on postoperative day 5, 10, 15 and every 5 days thereafter if appropriate. Clinical grading of the fistula was according to the ISGPF definition.
Radiological Intervention
Patients suspected to suffer from late PPH routinely underwent an urgent CT angiogram scan of the abdomen. If any evidence of active bleeding was noted, the patient was then immediately subjected to conventional catheter angiography for diagnostic confirmation and treatment. Stent grafts were favoured to treat pseudoaneurysms in situations where preservation of flow to the target organ is advisable (i.e., pseudoaneurysms of common hepatic artery). Haemorrhage from branches of superior mesenteric artery, splenic artery and gastroduodenal artery was controlled by occlusive metal coil embolisation.
MRSA Colonization and Infection
All patients admitted for pancreaticoduodenectomy were screened for MRSA status at admission as per hospital policy. This involved swabs of each of the nostrils, groin and open wounds. Further screening swabs were taken routinely during the patient’s postoperative stay in the hospital. Isolation of MRSA from any of these swabs was considered as “MRSA colonization”. In patients, with symptoms or signs of infection, body fluids including sputum, abdominal drains fluid and blood were cultured as well as wound swabs and central line catheter tips, as appropriate. Isolation of MRSA from any of these sites was deemed as systemic MRSA infe0ction. Fluid from the abdominal drains was routinely sampled and sent for culture on postoperative day 5-10-15 and every 5 days thereafter if appropriate.
ETHICS
The informed consent was obtained from each patient and the study protocol conforms to the ethical guidelines of the "World Medical Association Declaration of Helsinki", as reflected in a priori approval by the Ninewells Hospital ethics committee.
STATISTICS
Data are reported as mean±SD and frequencies. Median and range were used to describe the time of haemorrhage. Statistical analysis was performed using SPSS software (SPSS, Chicago, IL, USA). Continues variables were compared using Mann-Whitney U-test and categorical variables were compared with the Pearson chi square, the liner-by-linear chi square and Fisher’s exact tests as appropriate. Multivariate logistic regression was performed to identify independent risk factors and a two-tailed P value less than 0.05 was considered statistically significant.
RESULTS
Sixty-seven patients underwent pancreaticoduodenectomy during the study period. The mean operative blood loss was 1,324±678 mL and the mean duration of procedure was 420±70 minutes.
Seven patients developed PPH (10.4%). The haemorrhage was observed into the abdominal drain in all patients between postoperative day 3 and 35 (median 23 days). One patient developed massive bleeding after discharge and had to be readmitted. The mean haemoglobin levels before and after bleeding were 13±1.6 g/dL and 6.7±2.1, respectively. The mean number of units of blood transfusion required was 8.4±10.0 and all patients presented with haemodynamic instability requiring aggressive resuscitation. All these were classed as late haemorrhages (more than 24 hours) based on ISGPS classification.
The sites of haemorrhage, management and outcome are summarised in Table 1. All PPH were classified by us as ISGPS type C. The initial CT angiogram revealed the source of the bleeding in all patients and 6 patients went on immediately to have mesenteric angiography. Stent grafting (n=2) was used to control bleeding sites in the common hepatic artery (Figure 1) and coil embolisation (n=5) was employed for bleeding sites arising from branches of superior mesenteric artery, gastroduodenal artery and splenic artery (Figure 2). One patient who underwent metal coil embolisation of proximal hepatic artery for a large psuedoaneurysm from the stump of gastroduodenal artery required further coil packing of the vessel and a follow-up CT scan two weeks after the initial embolisation demonstrated persistent flow in the common hepatic artery. No laparotomy was ever needed after embolization.
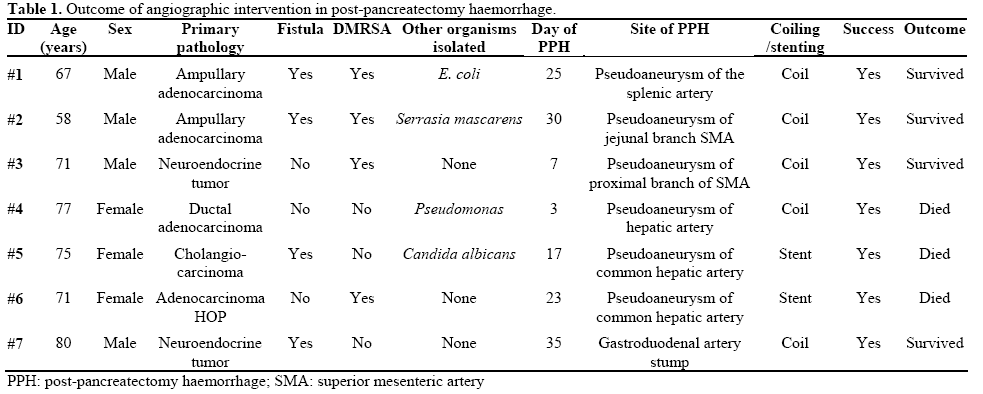
Figure 1: Digitally subtracted angiographic images. a. A
pseudoaneurysm arising from the stump of the gastroduodenal artery
(arrowed). The tip of the catheter is in the common hepatic artery. b. Image from the same patient after deployment of a 6x20 mm stentgraft
(arrowed) in the common hepatic artery across the origin of the
gastroduodenal artery. The stent-graft has excluded flow from the
gastroduodenal stump. The tip of the catheter is in the common
hepatic artery.
Figure 2: a. Axial CT image through the upper abdomen
demonstrating a pseudoaneurysm arising from the proximal splenic
artery. The splenic artery is compressed by pressure from
extravasated blood at the site of the pseudoaneurysm neck (arrowed). b. Digitally subtracted angiographic image from the same patient
showing occlusive embolisation coils placed in the splenic artery
both distal to (“back door”, straight arrow) and proximal to (“front
door”, curved arrow) the neck of the pseudoaneurysm. The tip of the
catheter is in the coeliac trunk.
No statistically significant difference was noted between the “PPH” and “no-haemorrhage” groups in sex (males: 4, 57.1% vs. 37, 61.7%; females: 3, 42.9% vs. 23, 38.3%; P=1.000), age (67±7 vs. 66±10 years; P=1.000), the number of patients with obstructive jaundice (5, 71.4% vs. 50, 83.37%, P=0.600), the site of pancreatic cancer (pancreatic: 2, 28.6% vs. 28, 46.7%; periampullary: 2, 28.6% vs. 19, 31.7%; distal cholangiocarcinoma: 1, 14.3% vs. 6, 10.0%; other: 2, 28.6% vs. 7, 11.7% P=0.589), the consistency of pancreas (firm: 3, 42.9% vs. 27, 45.0%; soft: 4, 57.1% vs. 33, 55.0%; P=1.000) and the T stage of the disease (T1: 0 vs. 2, 3.3%; T2: 3, 42.9% vs. 13, 21.7%; T3: 3, 42.9% vs. 41, 68.3%; T4: 1, 14.3% vs. 4, 6.7%; P=0.782).
One patient in the late PPH group (14.3%) compared to 6 patients in the no haemorrhage group (10.0%) had superior mesenteric vein resection and no significant association was noted between vein resection and development of PPH (P=0.556).
Overall thirty-eight patients tested positive to MRSA (56.7%). Thirty-one (46.3%) were found to be colonized by MRSA (routine postoperative screening swabs) of which 17 (54.8%) later on developed systemic MRSA infection at various sites (Table 2). Seven patients developed systemic MRSA infection without evidence of previous colonization. Patients who developed systemic MRSA infection had longer postoperative stay compared to the non MRSA group (31±11 vs. 22±2 days; P=0.005).

Twenty-eight patients (41.8%) were found to have high amylase levels in the drain fluid. Fourteen of them were ISGPF grade A and these leaks remained a laboratory finding only (subclinical fistula). Fourteen patients had clinically relevant fistulas (20.9%), of which ten patients had a grade B fistula (14.9%) and 4 a grade C (6.0%).
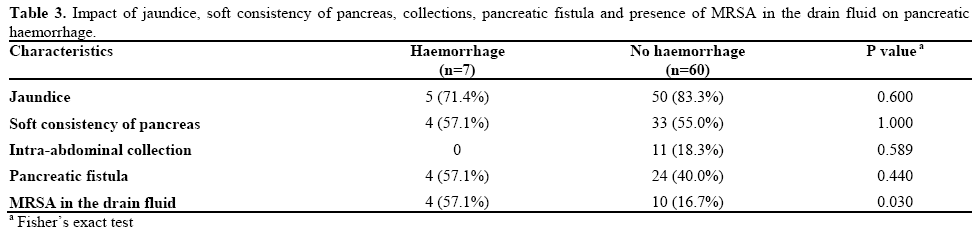
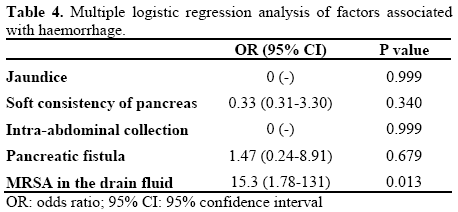
Amongst the 7 patients who developed PPH, 4 patients had a pancreaticojejunostomy fistula which we therefore graded as C (although this is not an inclusion criterion in the original ISGPF classification). No statistically significant correlation was noted between the development of PPH and both intra-abdominal collection and pancreatic fistula (Table 3). However, 4 out of the 7 patients who developed haemorrhage had MRSA isolated from the drain fluid, compared to 10 out of 60 patients who did not, develop PPH (P=0.030) (Table 3). The results were significant on univariate and multivariate analysis (Table 4). Various other organisms were cultured in drain fluid in patents with PPH, however MRSA was constantly isolated in four patients who developed PPH (Table 1).
Three out of the 7 patients (42.9%) who developed PPH eventually died. The cause of death was renal failure in two patients and a myocardial infarction in one patient. The site of haemorrhage in all three patients was the common hepatic artery. One patient died for pneumonia in the no-haemorrhage group giving an overall mortality in the present series of 6.0% (4/67)
DISCUSSION
Late post-pancreatectomy haemorrhage (after 24 hours) is a life threatening complication and remains a significant cause for morbidity following pancreaticoduodenectomy. In our experience, control of the haemorrhage was successfully achieved by angiographic treatment in all cases.
The exact mechanism of haemorrhage after pancreatic surgery is unclear but the presence of local sepsis and the association with a pancreatic fistula appear to be common predisposing factors [8, 12, 13]. Other reported risk factors include soft consistency of the pancreatic remnant and surgical trauma from vascular skeletonization during lymphadenectomy [13]. The differentiation of PPH into early (within 24 hours) and late (after 24 hours) has assumed significance as it has an impact on the therapeutical management and outcome. Haemorrhage in the early postoperative period in majority of the patients is usually attributed to technical failure and seems to have better prognosis [6, 13]. A delayed haemorrhage following pancreatectomy is often associated with local sepsis resulting from pancreatic abscess, fistula and bile leak [8, 12, 13, 14] and carries a significantly higher mortality [14].
The best treatment of a haemorrhage following pancreaticoduodenectomy is still subject to debate. Blanc et al. [6] similarly noted that majority of early bleeds were due to technical failure requiring laparotomy. On the contrary late PPH were better dealt with interventional angiography in stable patients, reserving surgery for unstable patients. Yekebas et al. [14] reviewed a large series of patients with PPH, where surgery was the primary treatment in unstable patients and interventional angiography was reserved for stable patients. They noted that 69% of patients required laparotomy to control haemorrhage with at least half of those dealt with initial interventional radiology or endoscopy requiring further laparotomy to control haemorrhage. This has never happened in our experience, where all angiographic interventions were successful in controlling the bleeding and no laparotomy was ever required. They also observed that interventional coiling was not possible in the vicinity of hepatic artery, a problem which is being increasingly addressed with stenting to preserve blood supply to the liver, like in two cases in our study [7, 15]. In addition, they observed a re-bleeding rate of 30% requiring repeat angiography (14% in our experience). Nevertheless, they report that over all success rate of radiological coiling was 80%.
With increasing expertise in dealing with primary bleeds more and more specialist centres are employing interventional radiology to deal with re-bleeding after initial embolisation, like in one case in our experience, and, as reported by Choi et al. who observed a rebleeding rate of 10% after embolisation, which was successfully controlled by repeat embolisation [8]. In our department we adopt a policy of routine imaging by CT angiogram in cases of late extraluminal PPH, almost irrespectively of haemodynamic status, with interventional catheter angiogram being reserved as a second line diagnostic technique or for therapeutic embolisation. In our experience all PPH were ‘late’ and noted after 48 hours and were successfully managed with angiographic intervention. We routinely prefer stent grafting to coil embolisation when possible for bleeding in the territory of common hepatic artery to preserve the blood supply to the liver, and prevent the occurrence of liver abscess and delayed bile leakage caused by ischaemia of the biliary system after embolisation [12, 16]. As noted in previous studies, bleeding from hepatic artery territory carried a high mortality rate despite successful stenting [8, 12] and this seems to be confirmed in our series where both patients who bled from the common hepatic artery died.
PPH is often reported in association with pancreatic fistula, although this did not reach statistical significance in our study. The ISGPF classification defined pancreatic fistula into different grades of severity based on the impact of fistula on clinical outcome. Although we have wholeheartedly adopted such an improved classification, we notice that the occurrence of a PPH is not included amongst the ISGPF criteria that define fistulas and we feel that this is a limitation of the classification. In our study 4 out of 7 patients who developed pancreatic haemorrhage had a pancreatic fistula and we graded these fistulas as C, because we felt that a major change in clinical management had occurred in these patients as a result of the haemorrhage. Although ISGPF classification does not associate type C fistulas with pancreatic haemorrhage, pancreatic fistula is a recognised risk factor for PPH and therefore we felt that these fistulas should be graded as type C. We propose that PPH is included in the ISGPF classification although we recognize that large scale studies and consensus amongst the HPB community would be required to finalise such a change and validate our findings.
The presence of MRSA infection in the drain fluid was a common finding in the PPH group (4 out of seven patients, 57%). We also noted a high prevalence of MRSA colonisation among patients undergoing pancreaticoduodenectomy but reassuringly only half of these patients proceeded on to develop a systemic MRSA infection. Although this may reflect the increasing incidence of MRSA in the UK, with infection rates doubling over the last seven years [17], only one previous study reported on the association between MRSA infection and PPH in one case. In our experience this association was strong and statistically significant (Table 2) and we conclude that, in all likelihood, MRSA may have infection contributed to these haemorrhages. We recognize however that our results should be interpreted cautiously due to small number of patients and larger studies are required to further validate this association. Nevertheless, in our opinion, a high index of suspicion of PPH is justified in patients with drain fluid positive for MRSA. In patients with signs of sepsis, we routinely send drain fluid for culture followed by antibiotic treatment based on the results of the culture. If MRSA is identified in the drain fluid we currently employ a policy of aggressive intravenous antibiotic treatment following advice from the microbiologist.
In conclusion, post-pancreatectomy haemorrhage is a life threatening complication. A policy of urgent CT angiogram followed by conventional catheter angiography in patients suspected to have a lateextraluminal PPH is effective for diagnosis and treatment of ongoing haemorrhage. Radiologically guided endovascular treatment is effective in achieving haemostasis for haemorrhage in the majority of cases and should be considered routinely if local expertise is available.
Note Poster at the 8th European Hepato-Pancreato- Biliary Association Annual Congress; Athens, Greece; June, 2009. Published as abstract: Sanjay P, Fawzi A, Kulli C, Tait IS, Polignano FM. Postpancreatectomy haemorrhage (PPH): risk factors and management by interventional radiology. HPB 2009; 11(S1):79.
Conflict of interest The authors have no potential conflict of interest
References
- Izbicki JR, Bloechle C, Knoefel WT, Rogiers X, Kuechler T. Surgical treatment of chronic pancreatitis and quality of life after operation. Surg Clin North Am 1999; 79; 913-44. [PMID 10470335]
- Büchler MW, Wagner M, Schmied BM, Uhl W, Friess H, Z'graggen K. Changes in morbidity after pancreatic resection: toward the end of completion pancreatectomy. Arch Surg 2003; 138:1310-4. [PMID 14662530]
- Grobmyer SR, Pieracci FM, Allen PJ, Brennan MF, Jaques DP. Defining Morbidity after Pancreaticoduodenectomy: Use of a Prospective Complication Grading System. J Am Coll Surg 2007; 204:356-64. [PMID 17324768]
- Sperti C, Paquali C, Piccoli A, Pedrazzoli S. Survival after resection for ductal adenocarcinoma of the pancreas. Br J Surg 1996; 83:625-31. [PMID 8689203]
- Ellison EC. Evidence-based management of hemorrhage after pancreaticoduodenectomy. Am J Surg 2007; 194:10-2. [PMID 17560901]
- Blanc T, Cortes A, Goere D, Sibert A, Pessaux P, Belghiti J, Sauvanet A. Hemorrhage after pancreaticoduodenectomy: when is surgery still indicated? Am J Surg 2007; 194:3-9. [PMID 17560900] 7. de Castro SM, Kuhlmann KF, Busch OR, van Delden OM, Laméris JS, van Gulik TM, et al. Delayed massive hemorrhage after pancreatic and biliary surgery: embolization or surgery? Ann Surg 2005; 241:85-91. [PMID 15621995]
- Choi SH, Moon HJ, Heo JS, Joh JW, Kim YI. Delayed hemorrhage after pancreaticoduodenectomy. J Am Coll Surg 2004; 199:186-91. [PMID 15275871]
- Bowrey DJ, Evans MD, Clark GW. Impact of methicillinresistant Staphylococcus aureus infection on outcome after esophagectomy. World J Surg 2007; 31:326-31. [PMID 17171479]
- Cowie SE, Ma I, Lee SK, Smith RM, Hsiang YN. Nosocomial MRSA infection in vascular surgery patients: impact on patient outcome. Vasc Endovascular Surg 2005; 39:327-34. [PMID 16079941]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005; 138:8-13. [PMID 16003309]
- Yamashita Y, Taketomi A, Fukuzawa K, Tsujita E, Harimoto N, Kitagawa D, Kuroda Y, et al. Risk factors for and management of delayed intraperitoneal hemorrhage after pancreatic and biliary surgery. Am J Surg 2007; 193:454-9. [PMID 17368288]
- Rumstadt B, Schwab M, Korth P. Haemorrhage after pancreatoduodenectomy. Ann Surg 1998; 227:236-41. [PMID 9488522]
- Yekebas EF, Wolfram L, Cataldegirmen G, Habermann CR, Bogoevski D, Koenig AM, et al. Postpancreatectomy hemorrhage: diagnosis and treatment: an analysis in 1669 consecutive pancreatic resections. Ann Surg 2007; 246:269-80. [PMID 17667506]
- Harvey J, Dardik H, Impeduglia T, Woo D, DeBernardis F. Endovascular management of hepatic artery pseudoaneurysm hemorrhage complicating pancreaticoduodenectomy. J Vasc Surg 2006; 43:613-7. [PMID 16520182]
- Yoon YS, Kim SW, Her KH, Park YC, Ahn YJ, Jang JY, et al. Management of postoperative haemorrhage after pancreatoduodenectomy. Hepatogastroenterology 2003; 50:2208-12. [PMID 14696500]



