Aman Makhija*, Arun Mohanty and Raja Ram Mantri
Department of Cardiology, Sir Ganga Ram Hospital, Rajinder Nagar, New Delhi, India
*Corresponding Author:
Aman Makhija
Department of Cardiology
Sir Ganga Ram Hospital, Rajinder Nagar
New Delhi
India
Tel: 9310928258
E-mail:Amanmakhija@gmail.com
Received date: August 26, 2017; Accepted date: October 28, 2017; Published date: November 02, 2017
Citation: Makhija A, Mohanty A, Mantri RR (2017) Late Fragmentation of Coronary Sinus Lead and Perforation with Retained Guide Wire after Cardiac Resynchronization Therapy. Interv Cardiol J. Vol.3 No. 3:66
Keywords
Lead fracture; Retained guide wire; Lead dislocation
Introduction
Passive fixation of coronary sinus leads is an imperfect technique with a high incidence of intra-operative and post-operative dislocations as high as 10% [1], leading to loss of left ventricular capture or undesirable phrenic nerve stimulation. The retained guide wire technique [2] has been proposed as an alternative method for stabilizing the left ventricular lead in patients who experience repetitive intra-operative dislocations. However longterm effects of retained guide wire on lead parameters are not known.
Case Presentation
We describe two cases of cardiac resynchronization therapy in which guide wire was retained in the coronary sinus lead because of recurrent intra-operative lead dislocations.
A 28-year-old male patient with dilated cardiomyopathy, Left bundle branch block (LBBB), severe Left ventricular dysfunction was implanted with a Cardiac resynchronization therapydefibrillator (CRT-D) device (Promote RF 3207-36, St Jude Medical, St. Paul, MN, USA). It was impossible to stabilize the bipolar lead (1258-1286 cm, St Jude Medical, St. Paul, MN, USA) in the desired posterolateral vein with repeated intra-operative dislocations. A retained guide wire technique was used as described by Cock et al. [2], maneuver consisting of exteriorizing of a hydrophilic guide wire (Whisper®, Guidant Corp., MN, USA) 10-15 mm beyond the electrode tip, its proximal portion was cut and left inside the electrode.
Our second patient was a 60-year-old male patient with Indwelling Dual chamber AICD with severe Left ventricular dysfunction with underlying Complete heart block, pacing dependent. He was taken up for up gradation to biventricular pacing (CRT-D) device. Intra-operative there was presence of phrenic nerve stimulation at all apical and mid locations thus requiring a basal placement of bipolar LV lead (1258-1286 cm, St Jude Medical, St. Paul, MN). Quadripolar pacing lead was not available in the Cath lab at the time of the procedure. Hydrophilic guide wire (Whisper®, Guidant Corp., MN, USA) was retained in a similar fashion as described previously to stabilize the lead in a basal position without phrenic stimulation with acceptable pacing thresholds.
At implant, the threshold of the LV electrode @ 0.5 ms was 1.5 V and 1.0 V respectively in both patients with impedances of 1008 Ω and 960 v respectively.
Results and Discussion
Both the patients showed initial improvement with satisfactory biventricular pacing at 3 and 6 months of follow up. However, they presented with deterioration in functional grade; first patient at 9 months and the other at 12 months post implantation. Device interrogation showed marked rise in LV lead impedance with loss of capture. Fluoroscopy revealed multiple sites of fragmentation in both the coronary sinus lead as well as the indwelling guide wire (Figure 1). In one patient, the proximal hard end of the guide wire perforated through the lead, subcutaneous tissue, and the overlying skin. Both these leads were subsequently extracted (Figure 2).
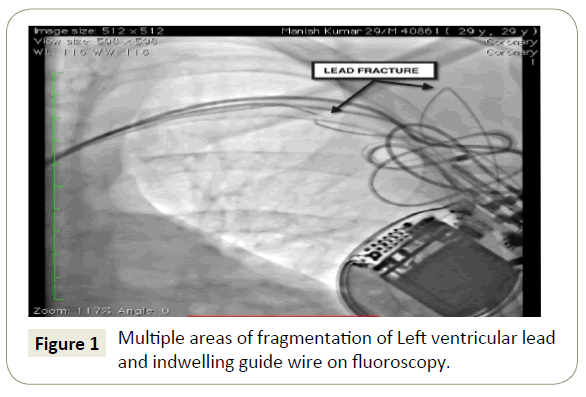
Figure 1: Multiple areas of fragmentation of Left ventricular lead and indwelling guide wire on fluoroscopy.
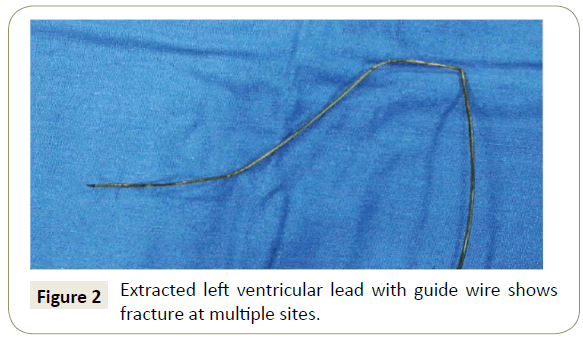
Figure 2: Extracted left ventricular lead with guide wire shows fracture at multiple sites.
The retained guide wire technique allows the guide wire to manipulate and stiffen the lead into one of the venous branches overlying the left ventricular wall. This allows the lead to remain in place and add rigidity to that lead and, presumably, reduce the likelihood of its eventual displacement. Cock et al. [2] had a follow up of 6 months in six patients without having seen any deterioration in the electrode. However as is evident from our experience in two patients, the presence of the guide wire inside the lead may be associated with prolonged friction inducing damage to the inner coil that may ultimately induce lead fracture. Lead fracture not only results in failure to capture as in our case but potentially can cause serious injury to the patient by penetration of guide wire fragments through vessel walls and subcutaneous tissue. Similar cases of coronary sinus lead fragmentation with retained guide wires have been reported in the literature from 6 months [3] to as late as two years after implantation [4].
Coronary angioplasty guide wires are not manufactured to resist the permanent mechanical stress, especially in the sub clavicular region. Taking into consideration that the guide wire is less flexible than the electrode, it is possible that this may break due to the repeated movements of the patients, which may damage the insulating layers and the spirals of the electrode. Given our experience, one should consider prophylactic replacement of leads already implanted by this technique.
Conclusion
The retained guide wire not only causes lead degradation but also can cause perforation as was seen in one of our patients. Guide wire inside a lead is neither durable nor safe and should not be retained.
References
- Azizi M, Castel A, Behrens S, Rodiger W, Nagele H (2006) Experience with coronary sinus lead implantations for cardiac resynchronization therapy in 244 patients. Herzschr Elektrophys 17: 13-18.
- De Cock CC, Jessurun ER, Allaart CA, Visser CA (2004) Repetitive intra-operative dislocation during transvenous lead implantation: Usefulness of the retained guide wire technique. Pacing Clin Electrophysiol 27: 1589-1593.
- Elena A, Antonio GQ, Eduardo C, Antonio D, Celestina A, et al. (2008) Late failure of left ventricular leads stabilized using the retained guide wire technique in patients undergoing cardiac resynchronization therapy. Rev Esp Cardiol 61: 91-94.
- Nagele H, Hashagen S, Ergin M, Azizi M, Behrens S (2007) Coronary sinus lead fragmentation 2 years after implantation with a retained guide wire. Pacing Clin Electrophysiol 30: 438-439.

