Keywords
Duodenal Neoplasms; Duodenum; Gastrointestinal Stromal Tumors; Neoplasms; Neuroendocrine Tumors; Somatostatin- Secreting Cells; Somatostatinoma
Conflict of interest
The authors have no potential conflicts of interest
INTRODUCTION
Duodenal endocrine tumors comprise 2-3% of all gastrointestinal endocrine tumors and are increasing in frequency. These include tumors producing a variety of peptides (gastrin, somatostatin, VIP, PP, etc.), non-functioning endocrine tumors, gangliocytic paragangliomas and poorly differentiated endocrine carcinomas. Although most of these tumors are non-functioning, duodenal/pancreatic endocrine tumors are a frequent cause of Zollinger-Ellison syndrome and can cause other clinical hormonal syndromes (carcinoid, Cushing's, etc.) [1]. Nowadays, the term “somatostatin-producing endocrine tumors” has replaced earlier terms, such as somatostatinomas, according to the recent World Health Organization Classification of Tumors [2]. These tumors are very rare neoplasms. Until recently, only about 170 cases have been reported in the literature [3]. These unusual neoplasms are often found in extra-pancreatic locations (most commonly in the duodenum, about 70%). The first case of a duodenal tumor exclusively producing somatostatin was reported by Kaneko et al. in 1979 [4]. Since that time, we have only been able to find only 109 cases of duodenal somatostatin-producing endocrine tumors published in the international literature.
In this paper, we present the case of a patient with von Recklinghausen’s disease, an ampullary somatostatin-producing endocrine carcinoma and a gastrointestinal stromal tumor in the gastric antrum (found incidentally during surgery and treated with a classic Whipple procedure). The relevant literature is briefly reviewed.
CASE REPORT
A 49-year-old female patient, with known von Recklinghausen’s disease, underwent abdominal ultrasonography during the followup for a known uterine leiomyoma. Ultrasound examination incidentally showed dilation of the biliary tree. The patient was asymptomatic and in good general condition. No weight loss, anorexia, nausea or vomiting had been reported. Clinical evaluation was unremarkable, without abnormal findings, except for the clinical manifestations of von- Recklinghausen’s disease (multiple skin pigmentation and subcutaneous tumors). Past medical history was unremarkable (except for the von Recklinghausen’s disease and the known uterine leiomyoma).
A diagnostic work-up revealed biochemical evidence of biliary obstruction. Abdominal computed tomography (CT), upper gastrointestinal endoscopy, and ERCP showed a duodenal mass at the ampulla of Vater, causing biliary tree dilatation. Preoperative endoscopic biopsy was negative for malignancy. The patient underwent a classic pancreaticoduodenectomy (Whipple procedure), with the presumed diagnosis of an ampullary neoplasm.
Macroscopic evaluation of the resected specimen showed a large (5 cm in diameter) polypoid mass at the ampulla of Vater. The distal part of the common bile duct was markedly dilated (2 cm in diameter). Of note, another mass was noted in the resected part of the stomach (5 cm in diameter, at the greater curvature) which was adherent to the omentum (Figure 1). Microscopic evaluation of the resected specimen showed that the ampullary mass was a well-differentiated endocrine carcinoma, causing an ulceration of the duodenal mucosa and infiltration of the ampulla of Vater (Figure 2a). Perineural infiltration and vascular emboli were also observed (Figure 2b). Early infiltration of the pancreatic head by the tumor was also evident. Three of the eleven resected lymph nodes were infiltrated by tumor cells. Immunohistochemistry revealed that the tumor was neuron-specific enolase (NSE)- positive, synaptophysin-positive, chromogranin A (CGA)-positive, and somatostatin-positive (Figure 3). Based on these findings and according to the recent WHO classification of gastroenteropancreatic endocrine tumors, the neoplasm was characterized as a large ampullary well-differentiated endocrine carcinoma composed exclusively of somatostatin immunoreactive cells (somatostatin-producing ampullary endocrine carcinoma), with lymph node metastases. Histology showed that the incidentally found mass in the greater curvature of the stomach was a gastrointestinal stromal tumor (5 cm in diameter), with low mitotic activity (1-4/10 HPF) (Figure 4).
Figure 1. The surgical specimen is opened. The mass
in the second part of the duodenum is evident,
protruding into the lumen (white arrow). The gastric
mass is also evident (red arrow).
Figure 2. Microscopic evaluation of the resected
specimen. a. Well differentiated endocrine tumor
infiltrating the ampulla of Vater (H&E, x40). b. Tumor
emboli within small veins of the subserosa. (H&E,
x100).
Figure 3. Immunohistochemistry. a. Tumor cells
strongly positive for synaptophysin (x100). b. Diffuse
immunoreactivity for somatostatin (x100).
Figure 4. Histology. a. Gastric mesenchymal tumor
with morphological features of a stromal tumor with
mild atypia and low mitotic activity (H&E, x100). b.
Gastric GIST: diffuse immunopositivity of neoplastic
cells for c-kit protein (x200).
The postoperative course was uneventful. The patient was discharged on postoperative day 8. During regular follow-up (which has included periodic abdominal CT and OctreoScan), no evidence of tumor recurrence has been observed for the six years following surgery.
DISCUSSION
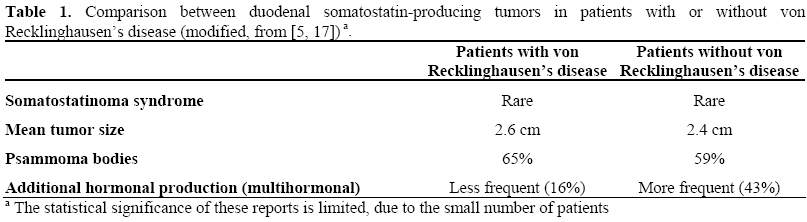
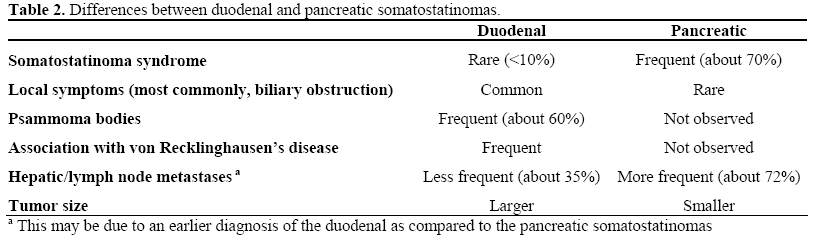
Duodenal somatostatin-producing endocrine tumors are a rare type of neoplasm, belonging to the group of gastrointestinal endocrine tumors. Gastrointestinal endocrine tumors are increasingly being recognized in clinical practice. These tumors may be either functioning or non-functioning, depending on their hormonal activity. Functioning and nonfunctioning gastrointestinal endocrine tumors are identical as regards development and histology but differ in their clinical course and outcome [5]. Non-functioning gastrointestinal endocrine tumors occur with the same frequency as hormonally active ones and they too therefore deserve consideration [5, 6]. Although somatostatin-producing gastrointestinal endocrine tumors may be of pancreatic origin, extrapancreatic (most commonly duodenal) somatostatin-producing gastrointestinal endocrine tumors are very common. The classic somatostatinoma syndrome (steatorrhea, cholelithiasis, and diabetes mellitus-like symptoms) is often observed in somatostatin-producing pancreatic endocrine tumors; in contrast, the somatostatinoma syndrome is a rare clinical manifestation in duodenal somatostatinproducing endocrine tumors (less than 10%) [3, 7]. Duodenal somatostatin-producing endocrine tumors tend to produce only local symptoms or are completely asymptomatic [5, 6, 8]. In symptomatic patients, jaundice induced by a periampullary tumor is the most common symptom reported [8, 9, 10]. The severity of these symptoms is directly related to the size and the location of the tumor and to the presence of metastases. Most symptomatic duodenal somatostatinproducing endocrine tumors are located at the ampulla of Vater and are usually more than 1 cm in diameter. The association of duodenal somatostatin-producing endocrine tumors with somatostatinoma syndrome is more probable in large tumors with metastatic disease; however, the presence of a large tumor or massive metastases does not guarantee symptoms of excessive somatostatin production [10, 11, 12, 13, 14]. Multiple neurofibromatosis or von Recklinghausen’s disease was first described in 1882 by von Recklinghausen [15]. It is a relatively common autosomal hereditary dominant disorder with a variable expression having a frequency of 1 out of 3,000-4,000 live births and a high rate of new mutations. Von Recklinghausen’s disease is characterized by multiple skin pigmentation (‘café au lait’ spots) and the formation of multiple nerve-sheath tumors. Neurofibromata originate from Schwann cells and may occur in any location, although they are found predominantly in the skin and subcutaneous tissue. The association between von Recklinghausen’s disease and tumors of neurogenic and neuroendocrine origin, such as meningiomas, gliomas, and pheochromocytomas is well known. Its association with duodenal neuroendocrine tumors, particularly somatostatin-producing endocrine tumors, though uncommon, has become more widely recognized as a distinct neuroendocrine syndrome during the two last decades [5, 16]. Up to the time of writing (November 2006), by reviewing the international literature, we found that duodenal somatostatin-producing endocrine tumors were associated with von Recklinghausen’s disease in 30 of 109 patients (27.5%). Duodenal somatostatinproducing endocrine tumors associated with von Recklinghausen’s disease tend to be located in the periampullary area, thereby causing biliary obstruction which is clinically manifested as painless obstructive jaundice (as occurred in our patient). Patients with von Recklinghausen’s disease have a tendency to develop periampullary tumors, most commonly somatostatin-producing endocrine neoplasms [17]. The prevalence of pheochromocytomas is also high (about 1%) in patients with von Recklinghausen’s disease as compared to the general population [18]. The incidence of pheochromocytomas is even higher (about 15%) in patients with duodenal somatostatin-producing endocrine tumors associated with von Recklinghausen’s disease [5]. This association (von Recklinghausen’s disease, duodenal somatostatin-producing endocrine tumors, pheochromocytoma) suggests an inherited endocrinopathy and represents a particular form of multiple endocrine neoplasia syndrome [3, 18]. Our patient also had a gastric GIST, incidentally found in the gastric antrum during surgery using a classic Whipple procedure which was confirmed after histological examination of the resected specimen. The association of duodenal somatostatin-producing endocrine tumor with von Recklinghausen’s disease and GIST is extremely rare. We found four papers in the international literature describing this association [19, 20, 21, 22]. We also found only a reported case of duodenal somatostatin-producing endocrine tumor associated with an appendiceal carcinoid tumor. Table 1 summarizes the differences between duodenal somatostatin-producing endocrine tumors associated with von Recklinghausen’s disease and duodenal somatostatin-producing endocrine tumors not associated with von Recklinghausen’s disease. In Table 2, the differences between pancreatic and duodenal somatostatinproducing endocrine tumors are presented.
In patients with clinical manifestations of somatostatinoma syndrome, diagnosis is established by demonstrating elevated somatostatin levels and the presence of a duodenal tumor [3]. As noted above, however, duodenal somatostatin-producing endocrine tumors are most often manifested by local symptoms. Diagnostic evaluation usually includes abdominal ultrasonography and abdominal computed tomography; as expected, a periampullary mass is commonly associated with dilatation of the biliary tree. However, radiological techniques often fail to detect small duodenal somatostatin-producing endocrine tumors [23]. Hypervascular lesions in the arterial phase, imaged on CT, are often characteristic of neuroendocrine tumors [23]; however, the different types of neuronendocrine tumors have similar radiological features. Somatostatin-receptor scintigraphy can be used to locate the primary tumor (if occult) and to stage the disease [24]. The sensitivity of this method is impaired when the tumor is small and when there are not many surface receptors, as in lessdifferentiated tumors.
The presence of the duodenal tumor is confirmed by upper gastrointestinal endoscopy. However, preoperative histological documentation of the diagnosis is not always possible. As a consequence, these patients are operated on with the presumed diagnosis of a periampullary tumor. Surgical resection is the treatment of choice for duodenal somatostatin-producing endocrine tumors. Local resection may be appropriate for small duodenal somatostatin-producing endocrine tumors. To achieve radical resection, larger tumors should be treated by pancreaticoduodenectomy. During pancreaticoduodenectomy, excision of localized metastatic disease could be achieved at the same time. Complete tumor resection or even debulking - when there is extensive metastatic disease (for example, massive liver metastases) - is of benefit for the patient [25] and can achieve long-term palliation or even cure [10].
A definitive diagnosis is established by histology and confirmed by immunohistochemistry. Immunohistochemistry is of particular importance when the tumor is not associated with the somatostatinoma syndrome (which is very common in duodenal somatostatin-producing endocrine tumors). The presence of psammoma bodies is a distinguishing feature of duodenal somatostatin-producing endocrine tumors. For unclear reasons, psammoma bodies are not observed in pancreatic somatostatinproducing endocrine tumors [12]. The surgical pathologist should be aware of this characteristic of duodenal somatostatinproducing endocrine tumors to avoid a potentially serious misdiagnosis [26].
The overall postoperative 5-year survival rate is 75% (ranging 40-60% in patients with metastases and 100% in patients without metastases) [3, 27]. Predictors of an unfavorable prognosis include size greater than 3 cm, poor cytological differentiation, regional and/or portal metastases and incomplete surgical resection [28]. Currently, there are no clinical trials demonstrating significant improvement in survival with the use of adjuvant therapy. The administration of somatostatin analogues inhibit somatostatin receptor activation and may alleviate symptoms in symptomatic patients [3]. Somatostatin-receptor scintigraphy is very useful for the follow-up of patients following surgical resection in order to detect incomplete tumor removal or distant metastases [24].
In conclusion, duodenal somatostatinproducing endocrine tumors are rare neoplasms, often associated with von Recklinghausen’s disease. The clinician should be aware of this association and should include duodenal somatostatin-producing endocrine tumors in the differential diagnosis when he/she faces a patient with known von Recklinghausen’s disease presenting with painless obstructive jaundice or a mass in the duodenum.
References
- Hoffmann KM, Furukawa M, Jensen RT. Duodenal neuroendocrine tumors: Classification, functional syndromes, diagnosis, and medical treatment. Best Pract Res ClinGastroenterol 2005; 19:675-97. [PMID 16253893]
- HeitzPh.U, Komminoth P, Perren A, Klimstra DS, Dayal Y, Bordi C, Lechago J, Centeno BA, Kloppel G. Pancreatic endocrine tumors. In: WHO Classification of Tumors, Volume 8, Pathology and Genetics, Tumors of Endocrine Organs FeLellis Ram Lloyd RV, Hitz PU, EngCh (Eds). WHO Press, October 2004, 177-85.
- Simon P, Spilcke-Liss E, Wallaschofski H. Endocrine tumors of the pancreas. EndocrinolMetabClin North Am 2006; 35:431-47. [PMID 16632104]
- Kaneko H, Yanaihara N, Ito S, Kusumoto Y, Fujita T, Ishikawa S, et al. Somatostatinoma of the duodenum. Cancer 1979; 44: 2273-6. [PMID 509396]
- Cappelli C, Agosti B, Braga M, Cumetti D, Gandossi E, Rizzoni D, AgabitiRosei E. Von Recklinghausen's neurofibromatosis associated with duodenal somatostatinoma. Minerva Endocrinol 2004; 29: 19 - 24. [PMID 15258554]
- Guo M, Lemos LB, Bigler S, Baliga M. Duodenal somatostatinoma of the ampulla of Vater diagnosed by endoscopic fine needle aspiration biopsy: a case report. Acta Cytol 2001; 45:622-6. [PMID 11480730]
- Green BT, Rockey DC. Duodenal somatostatinoma presenting with complete somatostatinoma syndrome. J ClinGastroenterol 2001; 33:415-17. [PMID 11606861]
- Hamy A, Heymann MF, Bodic J, Visset J, Le Borgne J, Lenéel JC, Le Bodic MF. Duodenal somatostatinoma. Anatomic /clinical study of 12 operated cases. Ann Chir 2001; 126:221-6. [PMID 11340706]
- Jordan PH. A personal experience with pancreatic and neuroendocrine tumors. J Am CollSurg 1999; 189:470-82. [PMID 10549736]
- O'Brien TD, Chejfec G, Pritz RA. Clinical features of duodenal somatostatinomas. Surgery 1993; 114:1144-7. [PMID 8256221]
- Wakeman C, Bagshaw PF, Gearry J, Jarvis J, Evans J, Ding S. Duodenal somatostatinoma: a rare cause of gastrointestinal bleeding. NZ Med J 2003; 116:U519. [PMID 12897887]
- Dayal Y, Doos WG, O'Brien MJ, Nunnemacher G, DeLellis RA, Wolfe HJ. Psammomatoussomatostatinomas of the duodenum. Am J Surg Pathol 1983; 7:653-65. [PMID 6139028]
- Sawady J, Katzin WE, Mendelsohn G, Aron DC. Somatostatin-producing neuroendocrine tumor of the ampulla (ampullarysomatostatinoma). Evidence of prosomatostatin production. Am J ClinPathol 1992; 97:411-5. [PMID 1371903]
- Borobia FG, Fabregat J, Jorba R, Poves I, Biondo S, Serrano T, et al. Exocrine pancreatic insufficiency caused by a somatostatinoma of the minor and major duodenal papilla in a patient with neurofibromatosis. Eur J Surg 2001; 167:154-6. [PMID 11266260]
- Von Recklingausen FD. Uber die multiplenfibrome der Haut und ihrebeziehungzu den multiplenneuromen. Berlin: A. Hirschwald; 1882.
- Griffiths DF, Williams GT, Williams ED. Multiple endocrine neoplasia associated with Von Recklinghausen's disease. Br Med J (Clin Res Ed) 1983; 287:1341-3. [PMID 6139138]
- Dayal Y, Tallberg KA, Nunnemacher G, DeLellis RA, Wolfe HJ. Duodenal carcinoids in patients with and without neurofibromatosis. Am J Surg Pathol 1986; 10:348-57. [PMID 2422964]
- Wheeler MH, Curley IR, Williams ED. The association of neurofibromatosis, pheochromocytoma, and somatostatin-rich duodenal carcinoid tumor. Surgery 1986; 100:1163-8. [PMID 2878497]
- Usui M, Matsuda S, Suzuki H, Hirata K, Ogura Y, Shiraishi T. Somatostatinoma of the papilla of Vater with multiple gastrointestinal stromal tumors in a patient with von Recklinghausen disease. J Gastroenterol 2002; 37:947-53. [PMID 12483251]
- Karatzas G, Kouraklis G, Karayiannakis A, Patapis P, Givalos N, Kaperonis E. Ampullary carcinoids and jejunal stromal tumour associated with von Recklinghausen's disease presenting as gastrointestinal bleeding and jaundice. Eur J SurgOncol 2000; 26:428-9. [PMID 10873367]
- Suzuki S, Sato K, Katada E, Kuno Y, Mizoguchi N, Tokuda H, et al. Periampullarysomatostatinoma and multiple gastrointestinal stromal tumors associated with von Recklinghausen's disease. J Gastroenterol 2004; 39:1011-2. [PMID 15549457]
- Bettini R, Falconi M, Crippa S, Capelli P, Boninsegna L, Pederzoli P. Ampullarysomatostatinomas and jejunal gastrointestinal stromal tumor in a patient with Von Recklinghausen's disease. World J Gastroenterol 2007; 13:2761-3. [PMID 17569151]
- Hamissa S, Rahmouni A, Coffin C, Wolkenstein P. CT detection of an ampullarysomatostatinoma in a patient with von Recklinghausen's disease. AJR Am J Roentgenol 1999; 173:503-4. [PMID 10430168]
- Krausz Y, Bar-Ziv J, de Jong RB, Ish-Shalom S, Chisin R, Shibley N, Glaser B. Somatostatin-receptor scintigraphy in the management of gastroenteropancreatic tumors. Am J Gastroenterol 1998; 93:66-70. [PMID 9448177]
- Modlin IM, Lewis JJ, Ahlman H, Bilchik AJ, Kumar RR. Management of unresectable malignant endocrine tumors of the pancreas. SurgGynecolObstet 1993; 176:507- 18. [PMID 8386860]
- Griffiths DF, Jasani B, Newman GR, Williams ED, Williams GT. Glandular duodenal carcinoid - a somatostatin rich tumor with neuroendocrine associations. J ClinPathol 1984; 37:163-9. [PMID 6141184]
- Soga J, Yakuwa Y. Somatostatinoma /inhibitory syndrome: a statistical evaluation of 173 reported cases as compared to other pancreatic endocarcinomas. J ExpClin Cancer Res 1999; 18:13-22. [PMID 10374671]
- House MG, Yeo CJ, Schulick RD. Periampullary pancreatic somatostatinoma. Ann SurgOncol 2002; 9:869-74. [PMID 12417508]





