Keywords
Minimally Invasive Surgical Procedures; Pancreaticojejunostomy; Pancreatitis, Chronic
INTRODUCTION
In patients with chronic pancreatitis, severe recurrent abdominal pain and functional endocrine/exocrine insufficiency of the pancreas are common and frequently debilitating [1–7]. The elevated pressure in the pancreatic ducts due to the obstruction of the pancreatic ducts is one of the main causes of the severe abdominal pain [8–10]. The combination of the ductal decompression and continuous drainage using a surgical procedure or an endoscopic approach comprise the basis for the treatment of patients with chronic pancreatitis [11–14]. With the recent development of various endoscopic instruments and techniques, endoscopic treatment can now be used as a first-line medical option for chronic pancreatitis [15–19]. However, the authors of two studies that compared endoscopic and surgical treatments of chronic pancreatitis patients reported that surgical treatment was more effective than endoscopic treatment [20,21]. In a prospective randomized trial, Dite et al. [20] observed that surgical treatment was superior to endoscopic treatment for long-term pain reduction in patients with painful obstructive chronic pancreatitis. Cahen et al. [21] also reported that the benefits of a surgical drainage procedure were demonstrated by more rapid, effective, and sustained pain relief compared to endoscopic treatment. In addition, Laramée et al. [22] found that surgical drainage treatment was highly cost-effective compared to endoscopic drainage treatment for patients with obstructive chronic pancreatitis.
Laparoscopic surgery was proposed as a minimally invasive alternative surgical procedure in the field of the pancreatic surgery [23–27]. Longitudinal pancreaticojejunostomy is a common and suitable surgical procedure to treat chronic pancreatitis patients with an obstructed and dilated main pancreatic duct [28–32]. Many studies of limited series of laparoscopic longitudinal pancreaticojejunostomy for the management of chronic pancreatitis have been reported [33–43], but the evaluations of the laparoscopic longitudinal pancreaticojejunostomy procedure have been limited and controversial. In this review, we discuss the current status of laparoscopic longitudinal pancreaticojejunostomy for chronic pancreatitis.
OPERATIVE TECHNIQUE
Laparoscopic trocars position of laparoscopic longitudinal pancreaticojejunostomy is about the same with laparoscopic distal pancreatectomy. We used five trocars (Figure 1). Severe adhesion between the posterior wall of the stomach and the anterior surface of the pancreas is often observed in patients with chronic pancreatitis. Such adhesion has been released with the use of several laparoscopic devices including laparoscopic coagulating shears (SonoSurg; Olympus, Tokyo), a vessel-sealing instrument (LigaSure; Covidien, Norwalk, CT), and an ultrasonically activated scalpel (Harmonic ACE; Ethicon, Cincinnati, OH). In these procedures, it is important to obtain a sufficient working space and ensure an adequate laparoscopic view. To maintain the exposure of the pancreas, the stomach is taped using sutures in two places, and then the stomach is fixed to the abdominal wall. We called this method of retraction of the stomach the “stomach-hanging method” (Figure 2) [44]. It is often difficult to secure an adequate laparoscopic surgical field at the pancreatic tail. In this case, we used an endoscopic surgical spacer (Securea; Hogy Medical Co., Tokyo) to make the surgical space with appropriate isolation of the stomach and mesocolon without grasping organs [45].
Figure 1. Placement of the five trocars.
Figure 2. To maintain the exposure of the pancreas, the stomach is
taped using sutures in two places, and then the stomach is fixed to the
abdominal wall.
In the longitudinal pancreaticoduodenectomy procedure for chronic pancreatitis, the main pancreatic duct is opened wide for complete drainage of the main pancreatic duct. To identify the main pancreatic duct, a thin needle such as a lumbar puncture needle is useful [36,37]. The main pancreatic duct is confirmed by aspirating pancreatic juice. Laparoscopic ultrasound also helps to identify the dilated main pancreatic duct [43]. In addition, ultrasound is a useful tool for detection of the pancreatic stones in the pancreatic duct. We used a flexible laparoscopic ultrasound probe (Hitachi Aloka, Ltd., Tokyo) (Figures 3a, b). Pancreatic stones cause the obstruction of the main pancreatic duct and then cause the elevation of the pressure in the main pancreatic duct. The removal of the pancreatic stones is necessary to release the elevated pressure in the main pancreatic duct.
Figure 3. (a.). Laparoscopic ultrasound is useful to identify the dilated
main pancreatic duct, ductal strictures, pancreatic calcification, and
pancreatic stones. (b.). Intraoperative laparoscopic ultrasound showing
a dilated main pancreatic duct and a pancreatic stone.
Usually, the pancreatic stones are removed under direct vision using laparoscopic grasping forceps. Sahoo et al. [43] reported that an endoscopic retrograde cholangiopancreatography basket viewed under a cystoscope was useful to remove leftover pancreatic stones in both the pancreatic head and tail end during a laparoscopic longitudinal pancreaticojejunostomy. However, the identification of the main pancreatic duct under laparoscopic guidance is unexpectedly difficult. In fact, Tantia et al. [36] reported that four patients required conversion to open surgery, and in three of these procedures the main pancreatic duct could not be isolated laparoscopically.
Khaled et al. [42] reported that the diameter of the main pancreatic duct in five patients who had undergone a complete laparoscopic longitudinal pancreaticoduodenectomy was 6–11 mm. They also noted that the use of laparoscopic ultrasound facilitated the identification of the pancreatic duct. Palanivelu et al. [37] reported that a good candidate diameter of the main pancreatic duct for a laparoscopic longitudinal pancreaticoduodenectomy was approx. 10 mm or larger. Sahoo et al. [43] reported that all 12 of their patients showed a diameter of more than 14 mm.
In most cases, a Roux loop of jejunum is fashioned and is brought to the lesser sac via the retrocolic route. A side-toside longitudinal pancreaticojejunostomy is reconstructed laparoscopically using a single layer of continuous or interrupted sutures. The pancreaticojejunostomy should cover nearly the entire length of the dilated main pancreatic duct; otherwise, the insufficient length of the pancreaticojejunostomy presents the risk of obstructing the pancreaticojejunostomy, and this result causes the recurrence of the severe pancreatic pain post-surgery. We opened widely the main pancreatic duct using SonoSurg (Olympus) (Figure 4).
Figure 4. The main pancreatic duct is opened longitudinally.
In general, it is difficult to suture laparoscopically in a pancreaticojejunal anastomosis for chronic pancreatitis, because chronic pancreatitis is accompanied by hard pancreatic parenchyma due to severe inflammation and pancreatic fibrosis. Santoro et al. [34] reported a laparoscopy-assisted longitudinal pancreaticojejunostomy with the mini-laparotomic left subcostal procedure for chronic pancreatitis patients with severe fibrotic pancreatic parenchyma. The hand-assisted laparoscopic surgery (HALS) strategy is also useful for pancreaticojejunal anastomoses for hard pancreatic parenchyma. The handling of a needle during pancreaticojejunal anastomoses for chronic pancreatitis is technically difficult because of the hard pancreatic parenchyma. However, it is well known that the postoperative risk of a pancreatic fistula of a hard pancreas such as that observed in chronic pancreatitis is low [46–48].
Pancreatic fistula is one of the most common and serious complications after pancreatic surgery [49–51]. We suspected that a laparoscopic longitudinal pancreaticojejunostomy for chronic pancreatitis would require a long operative time, but this procedure is safer for chronic pancreatitis. Glaser et al. [35] reported the use of a laparoscopic linear stapler device in laparoscopic longitudinal pancreaticojejunostomy. Anastomosis using a laparoscopic linear stapler is a familiar procedure for the drainage of the pancreatic pseudocyst. This technique is simple, easy and useful when the main pancreatic duct is extremely dilated and there are no residual pancreatic stones or stenosis of the main pancreatic duct.
OPERATIVE OUTCOMES
The main published series of laparoscopic longitudinal pancreaticojejunostomy for chronic pancreatitis are listed in Table 1. A total of 60 patients in the 11 available reports are featured in this review. Conversion to open surgery was required in five patients (8%). The reason for conversion was an inability to detect the main pancreatic duct under laparoscopic guidance in three of the patients and bleeding from branches of the splenic vein in the other two patients. The operating times ranged from 103 to 390 min. The case with the longest operative time was performed by robotic surgery. There were no operative mortalities. Postoperative complications were observed in five of the 60 patients (8%).
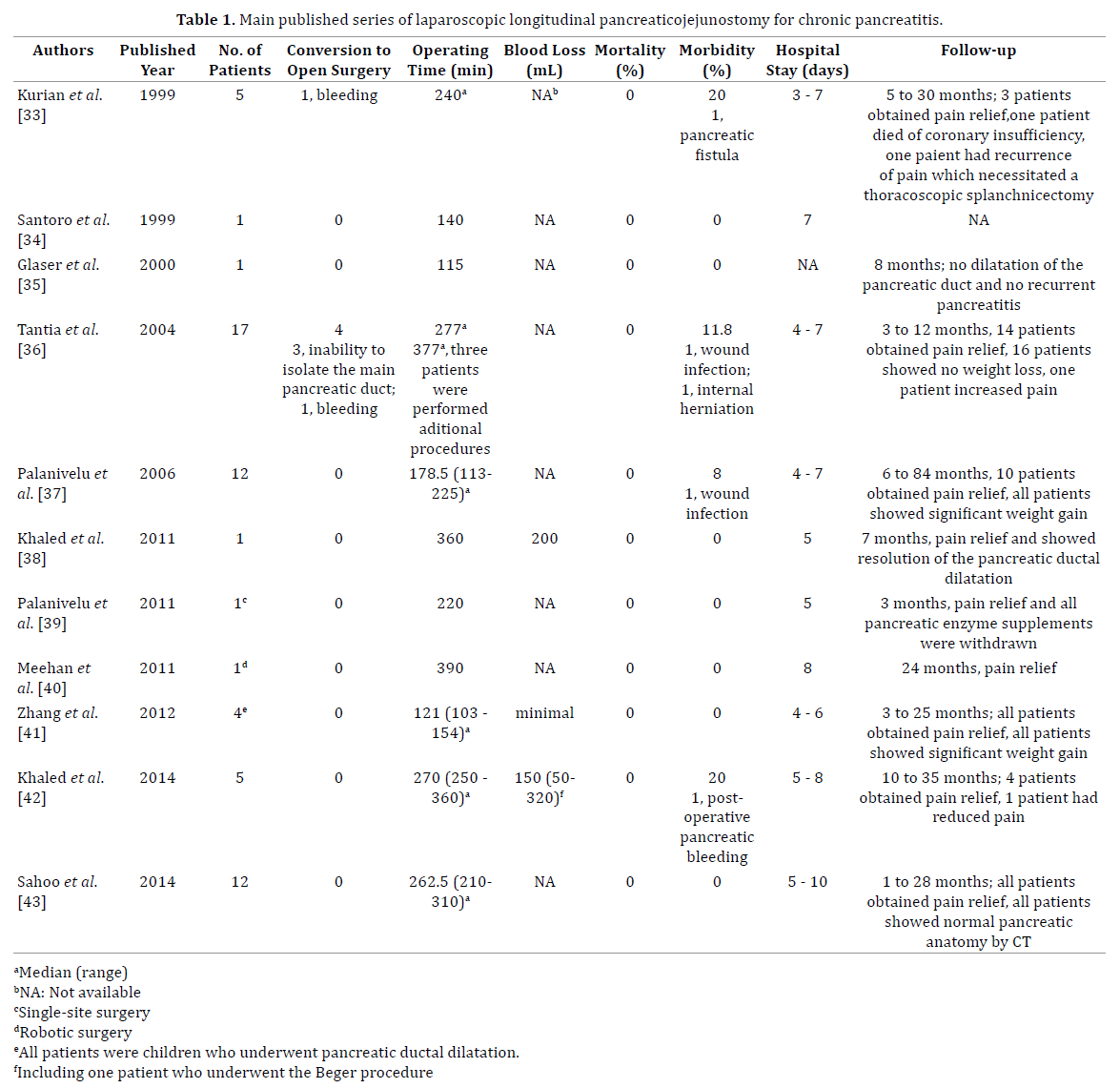
One of the most common and serious complications after pancreatic surgery is pancreatic fistula. In this series, only one patient (2%) showed postoperative pancreatic fistula. Several studies have shown that nonfibrotic pancreas, socalled ‘soft pancreas,’ is one of the most important risk factors for postoperative pancreatic fistula after pancreatic surgery [46–48]. Chronic pancreatitis is characterized by severe pancreatic fibrosis with the destruction of endocrine and exocrine pancreatic function [1–7]. Both pancreatic fibrosis and low pancreatic function are favorable to prevent a pancreatic fistula in chronic pancreatitis. Nealon et al. [12] reported that the complication rate, including pancreatic fistula, in conventional ancreaticojejunostomy for chronic pancreatitis was 4% for 124 patients.
The length of hospital stay can provide a valid measure of the invasiveness of an operative procedure. In this series of 60 patients, the range of length of hospital stay was from 3 days to 10 days. These length of hospital stay data are probably affected by a bias, because the studies were retrospective and the sample sizes were too small. Another parameter of invasiveness is intraoperative blood loss. Laparoscopic approaches using a magnified view have a potential advantage in that there is improved visualization of the anatomy for the resection of adhesive tissues and vessels along appropriate planes during a laparoscopic longitudinal pancreaticojejunostomy for chronic pancreatitis. However, there has been no randomized controlled study on laparoscopic versus conventional open longitudinal pancreaticojejunostomy for chronic pancreatitis, and it is thus difficult to determine whether a laparoscopic longitudinal pancreaticojejunostomy is less invasive compared to an open conventional operation.
Pain relief is the most important endpoint in evaluating the success of a longitudinal pancreaticojejunostomy for chronic pancreatitis [1–7]. In the present series, Tantia et al. [36] reported that 82% of their 17 patients were painfree. In reports of more than 10 cases, Palanivelu et al. [37] reported the rate of 83% of complete pain relief, and Sahoo et al. [43] reported the rate of 100% pain relief. However, a consensus statement by the American Gastroenterological Association following a review of studies evaluating the conventional longitudinal pancreaticojejunostomy for chronic pancreatitis stated that 60%–70% of the patients achieved continued pain relief [31]. These findings suggest that there are no significant differences between the laparoscopic and conventional procedures concerning pain control.
Another important endpoint is the preservation of pancreatic function. One of the postoperative advantages of longitudinal pancreaticojejunostomy compared to pancreatic resection for chronic pancreatitis is the preservation of the pancreatic function based on the preservation of the pancreatic parenchyma. Palanivelu et al. [37] reported that all 10 patients (100%) who underwent a laparoscopic longitudinal pancreaticojejunostomy achieved significant weight gain due to the improvement of their nutrition state. A recent systemic review by Yang et al. [52] supported early surgical treatment for chronic pancreatitis patients, not only for pain management but also for a reduced risk of pancreatic insufficiency. In the near future, laparoscopic longitudinal pancreaticojejunostomy at the early stage will be justified as a minimally invasive treatment for chronic pancreatitis.
CONCLUSION
Laparoscopic longitudinal pancreaticojejunostomy is a feasible, safe and effective surgical procedure for chronic pancreatitis patients with a dilated main pancreatic duct in the absence of an inflammatory pancreatic head mass, as well as conventional open surgery. However, at the present time, laparoscopic longitudinal pancreaticojejunostomy is still in the early phase of introduction, and we recommend that this procedure is performed only in carefully selected patients by highly skilled laparoscopic pancreatic surgeons with an experienced surgical team at a high-volume pancreatic surgery center.
Conflicting Interest
There is no conflict of interest to report on the part of any author.
References
- Klöppel G and Maillet B. Pathology of acute and chronic pancreatitis. Pancreas 1993;8:659-70. [PMID: 8255882]
- Steer ML, Waxman I, Freedman S. Chronic pancreatitis. N Engl J Med 1995;332:1482-90. [PMID: 7739686]
- Strate T, Knoefel WT, Yekebas E, Izbicki JR. Chronic pancreatitis: etiology, pathogenesis, diagnosis, and treatment. Int J Colorectal Dis 2003;18:97-106. [PMID: 12548409]
- Pezzilli R, Bini L, Fantini L, Baroni E, Campana D, Tomassetti P, et al. Quality of life in chronic pancreatitis. World J Gastroenterol 2006;12:6249-51. [PMID: 17072944]
- Witt H, Apte MV, Keim V, Wilson JS. Chronic pancreatitis: challenges and advances in pathogenesis, genetics, diagnosis, and therapy. Gastroenterology 2007;132:1557-73. [PMID: 17466744]
- Winstead NS and Wilcox CM. Clinical trials of pancreatic enzyme replacement for painful chronic pancreatitis: a review. Pancreatology 2009;9:344-50. [PMID: 19451744]
- Braganza JM, Lee SH, McCloy RF, McMahon MJ. Chronic pancreatitis. Lancet 2011;377:1184-1197. [PMID: 21397320]
- Bradley EL III. Pancreatic duct pressure in chronic pancreatitis. Am J Surg 1982;144:313-6. [PMID: 7114368]
- Drewes AM, Krarup A, Detlefsen S, Malmstrøm ML, Dimcevski G, Funch-Jensen P. Pain in chronic pancreatitis: the role of neuropathic pain mechanisms. Gut 2008;57:1616-27. [PMID: 18566105]
- Bouwense SA, de Vries M, Schreuder LT, Olesen SS, Frøkjaer JB, Drewes AM, et al. Systemic mechanism-oriented approach to chronic pancreatitis pain. World J Gastroenterol 2015;21:47-59. [PMID: 25574079]
- Izbicki JR, Bloechle C, Broering DC, Knoefel WT, Kuechler T, Broelsch CE. Extended drainage versus resection in surgery for chronic pancreatitis. Ann Surg 1998;228:771-9. [PMID: 9860476]
- Nealon WH and Matin S. Analysis of surgical success in preventing recurrent acute exacerbations in chronic pancreatitis. Ann Surg 2001;233:793-800. [PMID: 11371738]
- Riediger H, Adam U, Fischer E, Keck T, Pfeffer F, Hopt UT, et al. Long-term outcome after resection for chronic pancreatitis in 224 patients. J GastointestSurg 2007;11:949-60. [PMID: 17534689]
- Issa Y, van Santvoort HC, van Goor H, Cahen DL, Bruno MJ, Boermeester MA. Surgical and endoscopic treatment of pain in chronic pancreatitis: a multidisciplinary update. Dig Surg 2013;30:35-50. [PMID: 23635532]
- D’Haese JG, Ceyhan GO, Demir IE, Tieftrunk E, Friess H. Treatment options in painful chronic pancreatitis: a systemic review. HPB 2014;16:512-21. [PMID: 24033614]
- Hirota M, Asakura T, Kanno A, Shimosegawa T. Endoscopic treatment for chronic pancreatitis: indications, technique, results. J HepatobiliaryPancreatSci 2010;17:770-5. [PMID: 19826752]
- Oza VM and Kahaleh M. Endoscopic management of chronic pancreatitis. World J GastrointestEndosc 2013;5:19028. [PMID: 23330050]
- ShenY, Liu M, Chen M, Li Y, Lu Y, Zou X. Covered metal stent or multiple plastic stents for refractory pancreatic ductal strictures in chronic pancreatitis: a systemic review. Pancreatology 2014;14:87-90. [PMID: 24650959]
- Seicean A and Vultur S. Endoscopic therapy in chronic pancreatitis: current perspectives. ClinExpGastroenterol 2015;8:1-11. [PMID: 25565876]
- Dite P, Ruzicka M, Zboril V, Novotny I. A prospective, randomized trial comparing endoscopic and surgical therapy for chronic pancreatitis. Endoscopy 2003;35:553-8. [PMID: 12822088]
- Cahen DL, Gouma DJ, Yung N, Rauws EAJ, Boermeester MA, Busch OR, et al. Endoscopic versus surgical drainage of the pancreatic duct in chronic pancreatitis. N Engl J Med 2007;356:676-84. [PMID: 17301298]
- Laramée P, Wonderling D, Cahen DL, Dijkgraaf MG, Gouma DJ, Bruno MJ, et al. Trial-based cost-effectiveness analysis comparing surgical and endoscopic drainage in patients with obstructive chronic pancreatitis. BMJ Open 2013;3:e003676. [PMID: 24065699]
- Takaori K and Tanigawa N. Laparoscopic pancreatic resection: the past, present, and future. Surg Today 2007;37:535-45. [PMID: 17593471]
- Gumbs AA, Rodriguez Rivera AM, Milone L, Hoffman JP. Laparoscopic pancreatoduodenectomy: a review of 285 published cases. Ann SurgOncol 2011;18:1335-41. [PMID: 21207166]
- Venkat R, Edil BH, Schulick RD, Lidor AO, Makary MA, Wolfgang CL. Laparoscopic distal pancreatectomy is associated with significantly less overall morbidity compared to the open technique: a systemic review and meta-analysis. Ann Surg 2012;255:1048-59. [PMID: 22511003]
- Bausch D and Keck T. Laparoscopic pancreatic resections. Langenbecks Arch Surg 2013;398:939-45. [PMID: 24006117]
- Boggi U, Amorese G, Vistoli F, Caniglia F, De Lio N, Perrone V, et al. Laparoscopic pancreaticoduodenectomy: a systemic literature review. SurgEndosc 2015;29:9-23. [PMID: 25125092]
- Davies MM, Oshodi TO, Havard TJ, Lewis MH. Long term results of longitudinal pancreatico-jejunostomy for chronic pancreatic pain. HPB Surgery 1996;10:83-6. [PMID: 9184861]
- Mayo-Smith WW, Iannitti DA, Dupuy DE. Intraoperative sonographically guided wire cannulation of the pancreatic duct for patients undergoing a Puestow procedure. AJR 2000;175:1639-40. [PMID: 11090393]
- O’Neil SJ,Aranha GV. Lateral pancreaticojejunostomy for chronic pancreatitis. World J Surg 2003;27:1196-202. [PMID: 14534819]
- Ceppa EP, Pappas TN. Modified Puestow lateral pancreaticojejunostomy. J GastrointestSurg 2009;13:1004-8. [PMID: 18622654]
- Isaji S. Has the Partington procedure for chronic pancreatitis become a thing of the past? A review of the evidence. J HepatobiliaryPancreatSci 2010;17:763-9. [PMID: 19779664]
- Kurian MS,Gagner M. Laparoscopic side-to-side pancreatectomy (Partington-Rochelle) for chronic pancreatitis. J HepatobiliaryPancreatSurg 1999;6:382-6. [PMID: 10664286]
- Santoro E, Carlini M, Carboni F. laparoscopic pancreatic surgery: indications, techniques and preliminary results. Hepatogastroenterology 1999;46:1174-80. [PMID: 10370687]
- Glaser C, Müller W, Zerz A, Szinicz G. Laparoscopic laterolateralpancreatojejunostomy. Chirurg 2000;71:456-7. [PMID: 10840617]
- Tantia O, Jindal MK, Khanna S, Sen B. Laparoscopic lateral pancreaticojejunostomy: our experience of 17 cases. SurgEndosc 2004;18:1054-7. [PMID: 15156382]
- Palanivelu C, Shetty R, Jani K, Rajan PS, Sendhilkumar K, Parthasarthi R, et al. Laparoscopic lateral pancreaticojejunostomy. SurgEndosc 2006;20:458-61. [PMID: 16424983]
- Khaled YS, Ammori MB, Ammori BJ. Laparoscopic lateral pancreaticojejunostomy for chronic pancreatitis: a case report and review of the literature. SurgLaparoscEndoscPercutan Tech 2011;21:e36-40. [PMID: 21304372]
- Palanivelu C, Ahluwalia JS, Parthasarathi R, Palanisami S, Vaithiswaran V, Rajapandian S, et al. Laparoendoscopic single-site lateral pancreaticojejunostomy. Pancreatology 2011;11:500-5. [PMID: 22042294]
- Meehan JJ and Sawin R. Robotic lateral pancreaticojejunostomy (Puestow). J Pediatr Surg 2011;46:E5-8. [PMID: 21683190]
- Zhang JS, Li L, Liu SL, Hou WY, Diao M, Zhang J, et al. Laparoscopic pancreaticojejunostomy for pancreatic ductal dilatation in children. J Pediatr Surg 2012;47:2349-52. [PMID: 23217904]
- Khaled YS and Ammori BJ. Laparoscopic lateral pancreaticojejunostomy and laparoscopic Berne modification of Beger procedure for the treatment of chronic pancreatitis: the first UK experience. SurgLaparoscEndoscPercutan Tech 2014;24:e178-82. [PMID: 24710258]
- Sahoo MR and Kumar A. Laparoscopic longitudinal pancreaticojejunostomy using cystoscope and endoscopic basket for clearance of head and tail stones. SurgEndosc 2014;28:2499-503. [PMID: 24962852]
- Kuroki T,Adachi T, Okamoto T, Kanematsu T. Single-incision laparoscopic distal pancreatectomy. Hepatogastroenterology 2011;58:1022-4. [PMID: 21830435]
- Nakamura Y, Matsumoto S, Uchida E, Tajiri T, Jo Y, Inoue T. Use of endoscopic surgical spacer during laparoscopic pancreatic tumor enucleation. J Nippon Med Sch 2010;77:106-10. [PMID: 20453423]
- Kawai M, Kondo S, Yamaue H, Wada K, Sano K, Motoi F, et al. Predictive risk factors for clinically relevant pancreatic fistula analyzed in 1,239 patients with pancreaticoduodenectomy: multicenter data collection as a project study of pancreatic surgery by the Japanese Society of Hepato-Biliary-Pancreatic Surgery. J HepatobiliaryPancreatSci 2011;18:601-8. [PMID: 21491103]
- Harada N, Ishizawa T, Inoue Y, Aoki T, Sakamoto Y, Hasegawa K, et al. Acoustic radiation force impulse imaging of the pancreas for estimation of pathologic fibrosis and risk of postoperative pancreatic fistula. J Am CollSurg 2014;219:887-94. [PMID: 25262282]
- Casadei R, Ricci C, Taffurelli G, D’Ambra M, Pacilio CA, Ingaldi C, et al. Are there preoperative factors related to a “soft pancreas” and are they predictive pancreatic fistulas after pancreatic resection? Surg Today 2015;45:708-14. [PMID: 25331230]
- Aranha GV, Aaron JM, Shoup M, Pickleman J. Current management of pancreatic fistula after pancreaticoduodenectomy. Surgery 2006; 140:561-9. [PMID: 17011903]
- McMillan MT and Vollmer CM. Predictive factors for pancreatic fistula following pancreatectomy. Langenbecks Arch Surg 2014;399:811-24. [PMID: 24962147]
- Sell NM, Pucci MJ, Gabale S, Leiby BE, Rosato EL, Winter JM, et al. The influence of transection site on the development of pancreatic fistula in patients undergoing distal pancreatectomy: a review of 294 consecutive cases. Surgery 2015; 157:1080-7. [PMID: 25791028]
- Yang CJ, Bliss LA, Schapira EF, Freedman SD, Ng SC, Windsor JA, et al. Systemic review of early surgery for chronic pancreatitis: impact on pain, pancreatic function, and reintervention. J GastrointestSurg 2014; 18:1863-9. [PMID: 24944153]





