Keywords
Choristoma; Epidermal Cyst; Laparoscopy; Pancreatectomy; Spleen
INTRODUCTION
Accessory spleen is a congenital abnormality consisting of normal splenic tissue in ectopic sites that is found in approximately 10-15% of the general population. However, an intrapancreatic accessory spleen has seldom been reported and multiple epithelial cysts in the intrapancreatic accessory spleen are extremely rare. We herein report a case of 37-year-old woman with two epithelial cysts originating from an intrapancreatic accessory spleen who underwent laparoscopic distal pancreatectomy
CASE REPORT
An asymptomatic, 37-year-old woman was admitted to our hospital for surgery. In 2006, she was determined to have two cystic lesions in the pancreatic tail, 15 and 13 mm in size, respectively. By 2012, these cystic lesions had grown to 40 and 20 mm in size, respectively. She had a history of mixed connective tissue disease and took 2 mg of prednisone per day. Blood chemistry and urinalysis were within normal limits. The tumor markers CA 19-9 (251 U/mL; reference range 0-37 U/mL) and SPAN-1 (38 U/mL; reference range 0-30 U/mL) were increased. Computed tomography showed a multilocular cyst, 40 mm in size, and a unilocular cyst, 20 mm in size, in the tail of the pancreas and gallstones. The cystic component was hypointense on T1-weighted magnetic resonance images and hyperintense on T2-weighted magnetic resonance images (Figure 1). On magnetic resonance cholangiopancreatography, these cysts did not connect with the main pancreatic duct and had no solid components. Fluorine-18fluorodeoxyglucose positron emission tomography (FDG-PET) showed no significant increase in the maximum standard uptake value. Suspecting a mucinous cystic neoplasm or an intraductal papillary mucinous neoplasm with gallstones, a laparoscopic distal pancreatectomy was performed. First, the spleen and the pancreatic tail were mobilized from the retroperitoneum using the four-port technique laparoscopically (Figure 2). After the mobilization, the splenic artery was identified, double clipped, and ligated. The splenic vein was also clipped and dissected. After access was achieved through the 5 cm suprapubic incision, the pancreatic tail and spleen including the two cystic lesions were transected with a linear stapler (Endo GIA Ultra Universal Stapler, 30 mm Black, Covidien, Dublin, Ireland) (Figure 3) and extracted from the peritoneal cavity. A cholecystectomy was also performed. The operative time was 278 min and the blood loss was 50 mL.
Figure 1. Magnetic resonance imaging showed a multilocular
cyst, 40 mm in size, and a unilocular cyst, 20 mm in size, in the
tail of the pancreas.
Figure 2. The laparoscopic procedure was performed using the
four-port technique. The resected spleen and pancreatic tail were
pulled out through a 5 cm long suprapubic incision.
Figure 3. a. Laparoscopic view of the mobilization of the spleen and pancreatic tail. b. The pancreatic tail and spleen including the two cystic
lesions have been transected with a linear stapler.
Macroscopically, the cut surface of the tumor showed a unilocular cyst and a multilocular cyst completely surrounded with a brown solid component that resembled normal spleen. A histopathological examination showed that the walls of the two cysts were composed of fibrous tissue. The inner surface of the cyst was partly covered with non-keratinized stratified squamous epithelium, surrounded by normal splenic tissue.
The final pathological diagnosis was two epithelial cysts originating from an intrapancreatic accessory spleen (Figure 4). The patient had a pancreatic fistula (grade A, based on criteria of the International Study Group of Pancreatic Fistulas) and was managed conservatively. She was discharged on the 21st postoperative day. After the operation, her serum CA 19-9 levels decreased to normal. Over 12 months of follow-up, she continued to do well.
Figure 4. a. Unilocular cyst in the intrapancreatic accessory
spleen. b. Multilocular cyst in the intrapancreatic accessory
spleen. c. The histological section shows that the fibrotic wall (F)
lined with non-keratinized stratified squamous epithelium is
surrounded by accessory spleen tissue (S) in the pancreatic
parenchyma (P).
DISCUSSION
An accessory spleen is a congenital focus of healthy splenic tissue that is separated from the main body of the spleen. It results from failed fusion of the splenic anlage, which is located in the dorsal mesogastrium. This condition is observed in 10-30% of patients at autopsy. The splenic hilum is the most common site of an accessory spleen, followed by the pancreatic tail. In autopsy studies of 3,000 patients, 61 of 364 (17%) accessory spleens identified were found in the pancreatic tail [1]. Mortelé et al. performed abdominal CT scans in 1,000 consecutive patients. Of these patients, 156 (15.6%) had at least one accessory spleen, and intrapancreatic accessory spleens were seen in two patients (0.2%) [2].
However, cysts found within intrapancreatic accessory spleens are extremely rare. Nevertheless, a well-documented series of case reports can be found in the literature. Since the first case was described by Davidson et al [3] in 1980, 39 such cases, including the present report, have been documented in English language case reports (PubMed keywords: epithelial cyst, epidermoid cyst (epithelial inclusion cyst), intrapancreatic accessory spleen) [3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32] (Table 1). However, to the best of our knowledge, this report is the first to describe macroscopically multiple epithelial cysts within an accessory spleen.
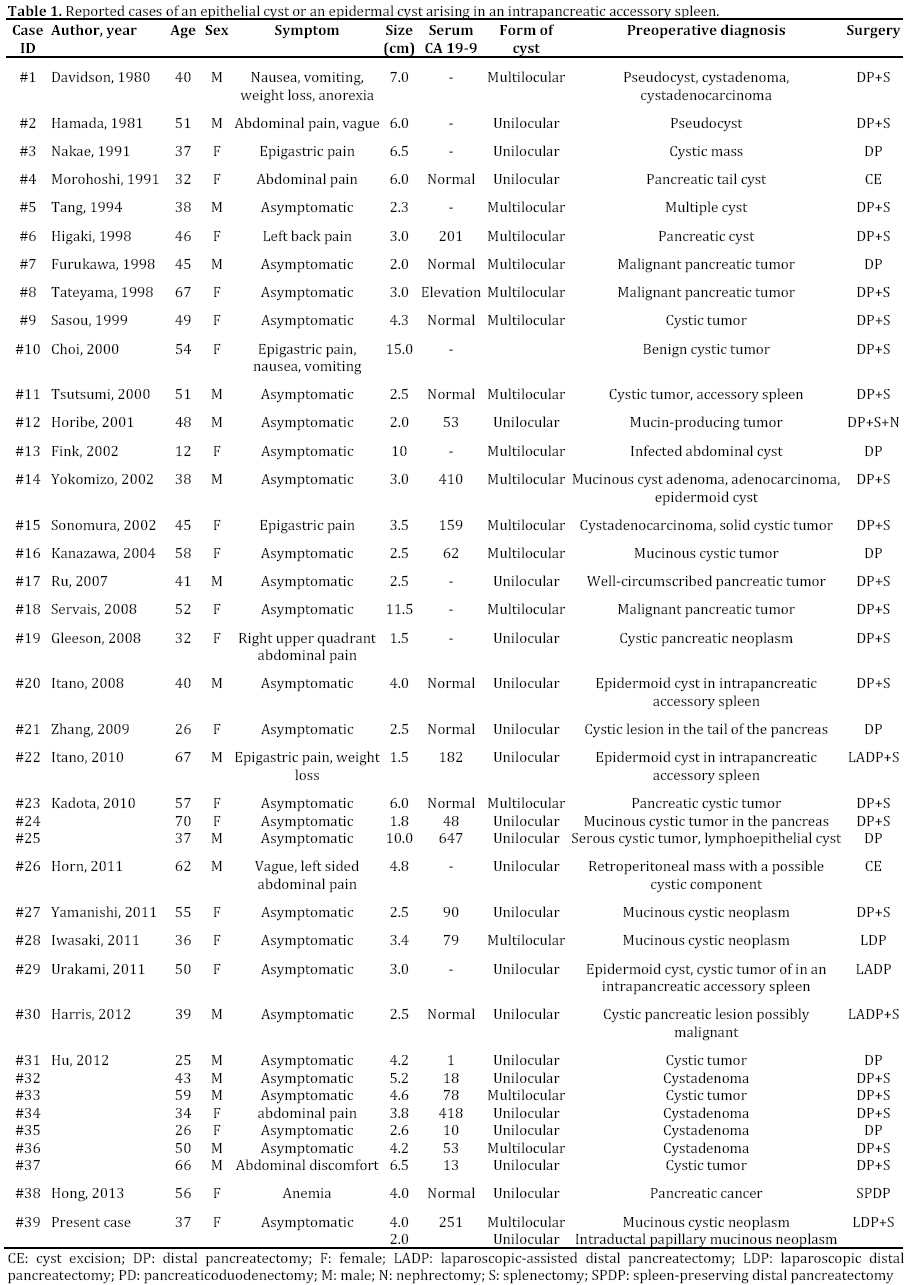
A review of previously reported cases reveals that these lesions can occur equally in men and women (18 men, 21 women) and occur most frequently in middle age, with a median age of 45 years (range: 12 to 70 years). All of the lesions were located in the tail of the pancreas. Over half of the presentations were asymptomatic (26 of 39), and several patients had various symptoms including abdominal pain, epigastric pain or discomfort (n=10), weight loss (n=2), nausea and vomiting (n=2), and so on. Serum CA 19-9 levels were elevated in 15 of 39 cases. The median maximum diameter of the cystic lesions was 3.65 cm (range: 1.5 to 11.5 cm). This entity can mimic a cystic neoplasm of the pancreas, and it is often difficult to diagnose preoperatively. Only 3 of 39 cases had a precise diagnosis of epithelial cyst arising in an intrapancreatic accessory spleen. The remaining diagnoses were as follows: cystic tumor (n=11); mucinous cystic neoplasm, including a mucin-producing pancreatic tumor (n=7); cystadenoma/ cystadenocarcinoma (n=6); benign/ malignant pancreatic tumor (n=5); pancreatic cyst (n=4); or pancreatic pseudocyst (n=2).
The serum CA 19-9 levels were elevated preoperatively but decreased postoperatively in the present case, as well as in previous cases [8, 27]. Although further studies are needed to clarify the mechanism that elevates serum CA 19-9 levels, some cases might show this elevation, and this should be taken into consideration in the differential diagnosis.
Distal pancreatectomy was performed under a preoperative diagnosis of pancreatic cystic neoplasms, possibly malignant tumors, in most cases. Only five cases were managed laparoscopically [24, 28, 29, 30, 32]. Laparoscopic technique has made significant strides and is thought to an effective method of surgical management in cases of pancreatic and splenic cystic lesions, avoiding the shortcomings of open surgery [33]. For unspecified tumors, such as the current case, that appear benign, even though malignancy cannot be completely ruled out, a laparoscopic procedure would therefore be one of the best ways to avoid the drawbacks of open surgery, such as considerable pain, a prolonged hospitalization, and a poor cosmetic result. In the current case, the patient was a young woman and she benefited from the good cosmetic result of laparoscopic surgery (Figure 5).
Figure 5. Postoperative scar at 3 months after surgery.
In conclusion, when an asymptomatic intrapancreatic mass is detected, even if multiple masses are present, the possibility of epithelial cysts originating from an accessory spleen should be considered. Laparoscopic distal pancreatectomy might be a safe and effective procedure and provide a good cosmetic result for benign or low-grade malignant cysts in the pancreas.
Conflict of interest
None of the authors have any conflicts of interest to declare
References
- Gayer G, Zissin R, Apter S, Atar E, Portnoy O, Itzchak Y. Apter S. CT findings in congenital anomalies of the spleen. Br J Radiol 2001; 74: 767-72. [PMID: 11511506]
- Mortelé KJ, Mortelé B, Silverman SG. CT features of the accessory spleen. AJR Am J Roentgenol 2004;183:1653-7. [PMID: 15547205]
- Davidson ED, Campbell WG, Hersh T. Epidermoid splenic cyst occurring in an intrapancreatic accessory spleen. Dig Dis Sci 1980;25:964-7. [PMID: 7449592]
- Hamada T, Isaji S, Mizuno S, Tabata M, Yamagiwa K, Yokoi H, et al. Laparoscopic spleen-preserving pancreatic tail resection foran intrapancreatic accessory spleen mimicking a nonfunctioning endocrine tumor: report of a case. Surg Today 2004;34:878-81. [PMID: 15449162]
- Nakae Y, Hayakawa T, Kondo T, Shibata T, Kitagawa M, Sakai Y, et al. Epidermoid cyst occurring in a pancreatic accessory spleen. J Clin Gastroenterol 1991;13:362-4. [PMID: 2066557]
- Morohoshi T, Hamamoto T, Kunimura T, Yoshida E, Kanda M, Funo K, et al. Epidermoid cyst derived from an accessory spleen in the pancreas. A case report with literature survey. Acta Pathol Jpn 1991;41:916-21. [PMID: 1785350]
- Tang X, Tanaka Y, Tsutsumi Y. Epithelial inclusion cysts in an intrapancreatic accessory spleen. Pathol Int 1994;44:652-4. [PMID: 7952152]
- Higaki K, Jimi A, Watanabe J, Kusaba A, Kojiro M. Epidermoid cyst of the spleen with CA19-9 or carcinoembryonic antigen productions: report of three cases. Am J Surg Pathol 1998;22:704-8. [PMID: 9630177]
- Furukawa H, Kosuge T, Kanai Y, Mukai K. Epidermoid cyst in an intrapancreatic accessory spleen: CT and pathologic findings. AJR Am J Roentgenol. 1998;171:271. [PMID: 9648813]
- Tateyama H, Tada T, Murase T, Fujitake S, Eimoto T. Lymphoepithelial cyst and epidermoid cyst of the accessory spleen in the pancreas. Mod Pathol 1998;11:1171-7. [PMID: 9872647]
- Sasou S, Nakamura S, Inomata M. Epithelial splenic cysts in an intrapancreatic accessory spleen and spleen. Pathol Int 1999;49:1078-83. [PMID: 10632928]
- Choi SK, Ahn SI, Hong KC, Kim SJ, Kim TS, Woo ZH, et al. A case of epidermoid cyst of the intrapancreatic accessory spleen. J Korean Med Sci 2000;15:589-92. [PMID: 11068999]
- Tsutsumi S, Kojima T, Fukai Y, Kanoh K, Shimura T, Mochiki E, et al. Epidermoid cyst of an intrapancreatic accessory spleen-a case report. Hepatogas- troenterology 2000;47:1462-4. [PMID: 11100377]
- Horibe Y, Murakami M, Yamao K, Imaeda Y, Tashiro K, Kasahara M. Epithelial inclusion cyst (epidermoid cyst) formation with epithelioid cell granuloma in an intrapancreatic accessory spleen. Pathol Int 2001;51:50-4. [PMID: 11148465]
- Fink AM, Kulkarni S, Crowley P, Crameri JA. Epidermoid cyst in a pancreatic accessory spleen mimicking an infected abdominal cyst in a child. Am J Roentgenol 2002;179:206-8. [PMID: 12076937]
- Yokomizo H, Hifumi M, Yamane T, Hirata T, Terakura H, Murata K, et al. Epidermoid cyst of an accessory spleen at the pancreatic tail: diagnostic value of MRI. Abdom Imaging 2002;27:557-9. [PMID: 12172997]
- Sonomura T, Kataoka S, Chikugo T, Hirooka T, Makimoto S, Nakamoto T, et al. Epidermoid cyst originating from an intrapancreatic accessory spleen. Abdom Imaging 2002;27:560-2. [PMID: 12172998]
- Kanazawa H, Kamiya J, Nagino M, Uesaka K, Yuasa N, Oda K, et al. Epidermoid cyst in an intrapancreatic accessory spleen: acase report. Journal of hepato-biliary-pancreatic surgery 2004;11:61-3. [PMID: 15754048]
- Ru K, Kalra A, Ucci A. Epidermoid cyst of intrapancreatic accessory spleen. Dig Dis Sci 2007;52:1229-32. [PMID: 17385039]
- Servais EL, Sarkaria IS, Solomon GJ, Gumpeni P, Lieberman MD. Giant epidermoid cyst within an intrapancreatic accessory spleen mimicking a cystic neoplasm of the pancreas: case report and review of the literature. Pancreas 2008;36:98-100. [PMID: 18192891]
- Gleeson FC, Kendrick ML, Chari ST, Zhang L, Levy MJ. Epidermoid accessory splenic cyst masquerading as a pancreatic mucinous cystic neoplasm. Endoscopy 2008;40:E141-2. [PMID: 18633876]
- Itano O, Shiraga N, Kouta E, Iri H, Tanaka K, Hattori H, et al. Epidermoid cyst originating from an intrapancreatic accessory spleen. J Hepatobiliary Pancreat Surg 2008;15:436-9. [PMID: 18670847]
- Zhang Z, Wang JC. An epithelial splenic cyst in an intrapancreatic accessory spleen. A case report. JOP 2009;10:664-6. [PMID: 19890189]
- Itano O, Chiba N, Wada T, Yuasa Y, Sato T, Ishikawa H, et al. Laparoscopic resection of an epidermoid cyst originating from an intrapancreatic accessory spleen: report of a case. Surg Today 2010;40:72-5. [PMID: 20037845]
- Kadota K, Kushida Y, Miyai Y, Katsuki N, Hayashi T, Bando K, et al. Epidermoid cyst in an intrapancreatic accessory spleen:three case reports and review of the literatures. Pathol Oncol Res 2010;16:435-42. [PMID: 19949910]
- Horn AJ, Lele SM. Epidermoid cyst occurring within an intrapancreatic accessory spleen. A case report and review of the literature. JOP 2011;12:279-82. [PMID: 21546709]
- Yamanishi H, Kumagi T, Yokota T, Koizumi M, Azemoto N, Watanabe J, et al. Epithelial Cyst Arising in an Intrapancreatic Accessory Spleen: A Diagnostic Dilemma. Intern Med 2011;50:1947-52. [PMID: 21921374]
- Iwasaki Y, Tagaya N, Nakagawa A, Kita J, Imura J, Fujimori T, et al. Laparoscopic resection of epidermoid cyst arising from anintrapancreatic accessory spleen: a case report with a review of the literature. Surg Laparosc Endosc Percutan Tech 2011;21:e275-9. [PMID: 22002295]
- Urakami A, Yoshida K, Hirabayashi Y, Kubota H, Yamashita K, Hirai T, et al. Laparoscopy-assisted spleen-preserving pancreatic resection for epidermoid cyst in an intrapancreatic accessory spleen. Asian J Endosc Surg 2011;4:185-8. [PMID: 22776306]
- Harris AC, Chaudry MA, Menzies D, Conn PC. Laparoscopic resection of an epidermoid cyst within an intrapancreatic accessory spleen: a case report and review article. Surg Laparosc Endosc Percutan Tech 2012;22:e246-9. [PMID: 22874714]
- Hu S, Zhu L, Song Q, Chen K. Epidermoid cyst in intrapancreatic accessory spleen: computed tomography findings and clinical manifestation. Abdom Imaging 2012;37:828-33. [PMID: 22327420]
- Hong R, Choi N, Sun K, Lim S, Han Y. Epidermoid cyst arising from an intrapancreatic accessory spleen: A case report and review of the literature. Oncol lett 2013:5:469-72. [PMID: 23420784]
- Iacobone M, Citton M, Nitti D. Laparoscopic distal pancreatectomy: up-to-date and literature review. World J Gastroenterol 2012:18:5329-37. [PMID: 23082049]






