Keywords
Knowledge; Practice; Immediate newborn care
Introduction
Neonate is a newborn infant. The neonatal period include the time from birth through the twenty eighth day of life [1]. Immediate Care of Newborn is the care given to the neonate following birth within the delivery room by skilled personnel [2].
Birth is a major challenge to the newborn to negotiate successfully from intrauterine to extra uterine life .The transition from intrauterine to extra uterine life is dramatic one and demands considerable and effective physiological alterations by the baby in order to ensure survival [3]. Newborn Care starts before birth. It starts with caring for pregnant mothers. During pregnancy a mother needs to be adequately nourished, free from infections, and monitored for complications. Good care during pregnancy, labor, and birth is the first step in good newborn care [4].
Immediate proper care of newborn is vitally important for survival, growth and development of a newborn. Despite several studies conducted about maternal and child health care practices, little is known about factors that determine behaviors related to immediate care of newborn. Most people are unaware of importance of immediate care of newborn and many unsafe behavior do exist such as common use of untrained attendants, unsafe cord care, immediate bathing of baby [5].
Maintaining and improving patient care requires active involvement of everyone in health care system, in order to meet the needs for evaluating health care in its totality as well as to identify whether effective and appropriate care has been provided. The quality is the major component of neonatal health care, and it demands participation from nurses rendering care [6].
Immediate care involves: The baby should be dried, placed skin-to-skin with the mother, and covered with dry linen to maintain temperature and to initiate early breast feeding, clear the airway, Evaluate Cardio respiratory function, Clamping and cutting the Umbilical Cord, Vit K and Tetracycline (TTC) eye ointment [7] so that this study was intended to assess the Knowledge and Practice of Immediate New born Care.
Methods and Materials
Study area and period
This study was conducted in Governmental health institutions in Bahir Dar city which is found in North West of Ethiopia 565 km far from Addis Ababa the capital city of Ethiopia in MCH settings from November to June 2008 E.C.
In Bahir Dar city, there are 9 sub cities, in each sub cities there are also kebeles and have a total of 10 governmental health centers and 2 hospitals. In addition there are also private health facilities which provide health care service to the community. There are a total of 141 health professionals who provide delivery, family planning, antenatal and postnatal (newborn) care. The study was conducted from November-June, 2008 E.C.
Study design
An institutional based descriptive cross-sectional study design was used for this study.
Source population
All health professionals who is working in governmental health facilities of Bahir Dar city.
Study population
Health professionals who is working in Maternal, New born and child health units of the selected Health Facilities.
Sample size and sampling procedure
Sample size calculation: A single population proportion formula was used to estimate the sample size and the following assumptions were made: Proportion of practice regarding immediate newborn care 52.4% (p=0.52) (2), level of significance 5% (α=0.05), 95 % confidence level (Z α/2=1.96) and absolute precision or margin of error 5% (d=0.05).

Where, n=sample size
p=proportion of knowledge or practice of health care providers (52.4%)
Z=standard normal distribution curve value for the 95% confidence interval (1.96)
d=the margin of error or accepted error
n=383 health care providers.
Adding a 10% allowance for a non-response rate, the total sample size was 421. But the total number of health professionals at the selected governmental health facilities was 141 therefore we were included all of them.
Sampling procedure: In Bahir Dar city there are 9 sub cities. There are 12 governmental health facilities and seven of them (Han HC, FHRH...) was selected with lottery method. 141 study subjects were included using non probability convenience methods. Those health professionals found working in MCH setting during data collection time.
Inclusion criteria
All health professionals who is working in maternal newborn and child health (MCH) units.
Data collection
Data collection techniques were through self-administered questionnaire and check list.
Tools: self-administered questionnaire (which involves 10 questions for socio demographic characteristics and 53 questions for knowledge) and 29 Observation check list (for practice). The data was collected by group members. Data collection period: Data was collected starting from May 10-24, 2008 E.C.
Data quality assurance
To assure quality of the data the following measures was undertaken: Two week prior to the actual data collection, questionnaire was pre tested on 5% of the sample on health professionals in separate health facilities. After the actual data collection process, the collected data was cross checked for questionnaires consistency and completeness. After data collection, each questionnaire was given a unique code.
Data processing and analysis
After data collection each questionnaire was checked for completeness and consistency. Then the data was entered and analyzed by using statistical package for social science (SPSS) version 20.0. Graphs, charts and tables were used to summarized and presented major findings. Descriptive statistics like number and percent was used to illustrate socio demographic characteristics of the study population.
Ethical consideration
Ethical clearance and approval was obtained from midwifery department, college of Medicine health science, Bahir Dar University. Letters were obtained from department of midwifery to selected health facilities. After explaining about the purpose, the possible benefit of the study, permission was obtained from each respondent before taking interview. Confidentiality was maintained in each level of the response in this study.
Results
Response rate
Out of 141 conveniently selected health professionals 134 participated in the study which gives a response rate of 95%, of which respondents 76 (56.8%) were from hospital and 58 (43.2%) were from health center.
Socio-demographic characteristics of study participants
Out of 134 participants in the study, 81 (60.9%) were males, and majority of participants 63 (47%) were in the group of 25-29. The mean age of respondents was 25 years with a standard deviation 3.6 and range 28. Regarding their religion, Orthodox Christianity was the dominant religion consisting of 123 (91.7%).By their marital status 95 (70.9%) single and 35 (26.1%) were married. By their ethnicity 104 (78.2%) of respondents were Amhara (Table 1).
| Variables |
Frequency (N=134) |
Percent |
| Age |
20-24 |
58 |
43.3 |
| 25-29 |
63 |
47 |
| 30-34 |
7 |
5.2 |
| 35-39 |
5 |
3.7 |
| 40-44 |
0 |
0 |
| 45-49 |
1 |
0.7 |
| 50 and above |
0 |
0 |
| Sex |
Male |
81 |
60.4 |
| Female |
53 |
39.6 |
| Religion |
Orthodox |
122 |
91.7 |
| Muslim |
8 |
6 |
| Protestant |
2 |
1.5 |
| Catholic |
1 |
0.8 |
| Marital status |
Single |
95 |
70.9 |
| Married |
35 |
26.1 |
| Divorced |
3 |
2.2 |
| Widowed |
1 |
0.7 |
| Ethnicity |
Tigray |
16 |
12 |
| Amhara |
104 |
78.2 |
| Oromo |
13 |
9.7 |
| Profession |
Midwifery |
40 |
29.8 |
| Nurse |
44 |
32.8 |
| Doctor |
42 |
31.3 |
| Health Officer |
5 |
3.7 |
| Emergency Surgery |
3 |
2.2 |
| Educational Level |
Diploma |
47 |
35.1 |
| Degree |
83 |
61.9 |
| Master |
4 |
3 |
| Work Environment |
Hospital |
76 |
56.8 |
| Health Centre |
58 |
43.2 |
| Work Experience |
<1 year |
51 |
38.1 |
| 1-5 years |
55 |
41 |
| 6-10 years |
23 |
17.2 |
| 11-15 years |
2 |
1.5 |
| 16-20 years |
2 |
1.5 |
| >21 years |
1 |
0.7 |
| Monthly Salary |
1663-2383 |
24 |
17.9 |
| 2384-3104 |
58 |
43.1 |
| 3105-3825 |
17 |
12.7 |
| 3826-4546 |
10 |
7.5 |
| 4547-5267 |
13 |
9.7 |
| >5268 |
12 |
9 |
Table 1: Socio-demographic characteristics of health professionals at Bahir Dar city governmental health facilities, Amhara region, Ethiopia 2016.
According to participant profession, 40(29.8%) were midwives and 44 (32.8%) were nurses. 79 (59%) were degree and Forty six (34.6%) were diploma (Table 1).
As shown from the pie chart below, among 134 study participants, 75(56%) had good knowledge on immediate new born care and 18 (13.4%) had poor knowledge. The rest 41 (30.6%) of respondent health professionals had fair knowledge on care given to immediately born baby (Figure 1).
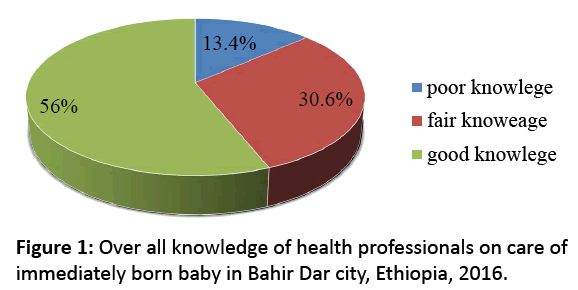
Figure 1: Over all knowledge of health professionals on care of immediately born baby in Bahir Dar city, Ethiopia, 2016.
Concerning knowledge of health professionals on umbilical cord and care 122 (91.1%) of participants were used sterile scissor. 133 (99.3%) of participants were knowledgeable to weigh baby immediately after delivery. Regarding knowledge on the advantage of first milk/colostrum 126 (94%) had general knowledge, 8 (6%) of respondents were not knowledgeable on the importance of colostrum or squeezed out colostrum before feeding the new born baby. A total of 132 (98.5%) of respondents had knowledge on complications of immediately born baby and 116 (86.6%) had knowledge on skin- to-skin contact.
Among respondents who had participated in this survey, 84 (62.7%) received in service training regarding immediate new born care. Of these 44 (32.8%) received one time, 20 (14.9%) two times and 20 (14.9%) of respondents were received the training above two times and were the rest 50 (37.3%) had no training. From the 10 steps of care give to immediately born baby knowledge of respondents were 122 (91%) to deliver baby onto mothers abdomen, dry baby 121 (90.3%) and 119 (88.8%) were assess baby breathing (Table 2).
| Variable |
Frequency (N=134) |
Percent |
| Knowledge of health professionals on steps of care given to immediately born baby |
| Deliver baby onto mothers abdomen |
122 |
91 |
| Dry baby |
121 |
90 |
| Assessing breathing |
119 |
88.8 |
| Cord cutting |
119 |
88.8 |
| Early initiation of breast feeding |
115 |
85.8 |
| Skin-to-skin contact with mother |
116 |
86.6 |
| Apply TTC eye ointment |
115 |
85.8 |
| Giving vitamin K |
115 |
85.8 |
| Weigh baby |
115 |
85.8 |
| Place identification bands on wrist or ankles |
36 |
26.8 |
Table 2: Knowledge of health professionals on the steps of care given to immediately born baby in Bahir Dar city, Ethiopia, 2016.
One hundred nineteen (88.8%) of respondents had knowledge on Asphyxia that is a complication of new born baby. A total of 119 (88.8%) of respondents were knowledgeable that Assess breathing and cord cutting and caring prevent complication of new born baby (Table 3).
| Variable |
Frequency (N=134) |
Percent |
| Knowledge of health professionals on complication of immediately born baby |
| Hypothermia |
116 |
86.6 |
| Asphyxia |
119 |
88.8 |
| Infection |
102 |
76.1 |
| Hypoglycaemia |
17 |
12.6 |
| Neonatal bleeding |
2 |
1.5 |
| Jaundice |
2 |
1.5 |
| Trauma |
1 |
0.75 |
| Knowledge of Preventive methods for complication of new born baby |
| Deliver baby onto mother`s abdomen |
107 |
79.9 |
| Dry baby |
110 |
82.1 |
| Assess breathing |
116 |
86.6 |
| Cord cutting and care |
106 |
79.5 |
| Early initiation of breast feeding |
108 |
80.6 |
| Skin-to-skin-contact with mother |
114 |
85.1 |
| Apply TTC eye ointment |
105 |
78.4 |
| Giving vitamin K |
99 |
73.9 |
| Weigh baby |
90 |
67.1 |
| Resuscitation |
1 |
0.75 |
Table 3: Knowledge of health professionals on complications of immediately born baby and its preventive methods in Bahir Dar city, Ethiopia, 2016.
One hundred three (76.9%) of respondents had knowledge that skin-to-skin contact helped baby stay warm and prevent from hypothermia and 1 (0.7%) help to expel placenta. If baby not cried immediately after delivery, 92 (68.7%) of respondents had knowledge to suck the air way followed with call a help and start resuscitation 81 (60.4%) but 3 (2.2%) of respondents had no knowledge. Majority of respondents 123 (91.8%) had knowledge to bath new born baby after 24 h of delivery (Table 4).
| Variable |
Frequency (N=134) |
Percent |
| Knowledge of health professionals on advantage of skin-to-skin contact |
| Prevent hypothermia |
25 |
18.7 |
| Help baby stay warm |
6 |
4.5 |
| Both (prevent hypothermia and help to stay warm) |
103 |
76.9 |
| Help expel placenta |
1 |
1.5 |
| Enhance early breast feeding and bonding |
8 |
6 |
| Knowledge of health professionals on measures to be taken for baby unable to cry after delivery |
| Suck the baby |
92 |
68.7 |
| Call a help and start resuscitation |
81 |
60.4 |
| Start cardio-pulmonary resuscitation |
48 |
35.8 |
| Stimulation |
3 |
2.2 |
| Nothing |
3 |
2.2 |
| Knowledge on time of bathing for immediately born baby |
| Before 24 h of delivery |
9 |
6.7 |
| After 24 h of delivery |
123 |
91.8 |
| I do not know |
2 |
1.5 |
| Knowledge on the importance of Providing eye ointment |
| Prevent ophthalmic neonatorm |
21 |
15.7 |
| Prevent breast tingling |
1 |
0.75 |
| Prevent hypothermia |
1 |
0.75 |
| Prevent neonatal conjunctivitis |
94 |
70.2 |
| Prevent trauma |
8 |
6 |
| Prevent blindness |
1 |
0.75 |
| Prevent cord bleeding |
1 |
0.75 |
Table 4: Knowledge of health professionals on some important cares given to immediately born baby in Bahir Dar city, Ethiopia, 2016.
One hundred thirty three (99.2%) of respondents had knowledge that providing eye ointment to new born baby among those 94 (70.2%) had knowledge to prevent neonatal conjunctivitis followed by prevents from ophthalmic neonatorum 21 (15.7%) (Table 4).
One hundred ten (82.1%) of respondents had knowledge on the advantage of colostrum that it prevents new born baby from infection and gives important nutrients to the new born baby (Table 5).
| Variable |
Frequency (N=134) |
Percent |
| Knowledge on advantage of early initiation of breast feeding |
| Enhances bonding of mother and baby |
119 |
88.8 |
| Prevents from hypoglycaemia |
119 |
88.8 |
| Prevents from hypothermia |
99 |
73.9 |
| Prevents from infection |
95 |
70.9 |
| Development and growth |
2 |
1.5 |
| Knowledge on advantage of colostrum |
| Prevents from infection |
6 |
4.5 |
| Gives important nutrient |
17 |
12.8 |
| Both |
109 |
82 |
Table 5: Knowledge of health professionals on advantage of early initiation of breast feeding and colostrum in Bahir Dar city, Ethiopia, 2016.
As shown from the figure above, 128 (95.8%) of respondents had knowledge to initiate breast feeding or new born baby within one hour of delivery and 6 (4.5%) had knowledge of breast feeding after 1 h of delivery (Figure 2).
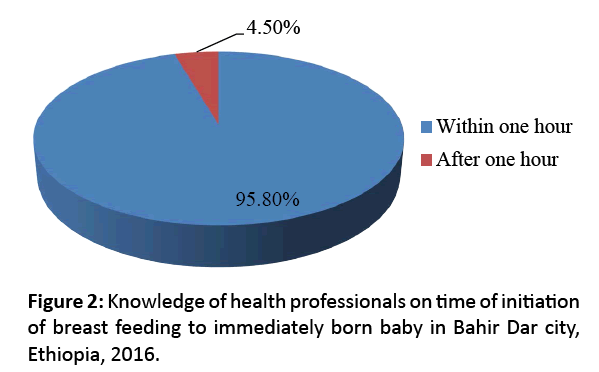
Figure 2: Knowledge of health professionals on time of initiation of breast feeding to immediately born baby in Bahir Dar city, Ethiopia, 2016.
As shown from the graph, most respondents of this study had knowledge to place baby on mother’s abdomen 127 (94.8%), 20 (14.9%) to place baby on clean and separate table (Figure 3).
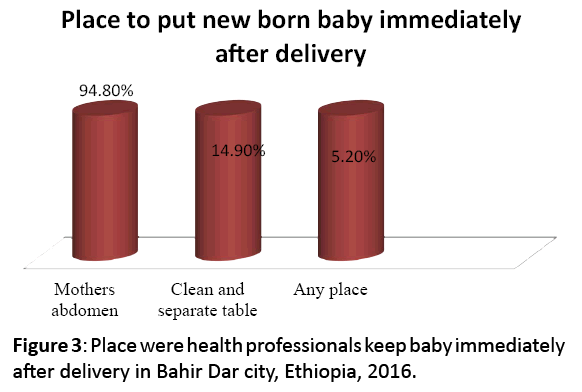
Figure 3: Place were health professionals keep baby immediately after delivery in Bahir Dar city, Ethiopia, 2016.
Knowledge of respondents on importance of vitamin K were, 102 (76.1%) mentioned that it prevents from bleeding and 2 (1.5%) of respondents prevent rickets but 1 (0.75%) responds prevent eye infection (Figure 4).
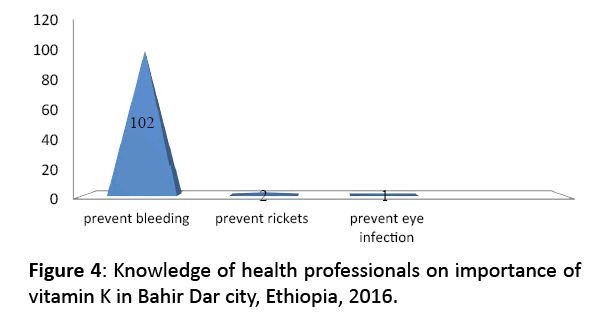
Figure 4: Knowledge of health professionals on importance of vitamin K in Bahir Dar city, Ethiopia, 2016.
Practice of health professionals on immediate new born care
According to the checklists used to asses’ practice of health professionals towards immediate newborn care Greater than half (59.7%) of the respondent had good practice regarding new born care (Figure 5).
Figure 5: Practice of health professionals on immediate newborn care in Bahir Dar city Governmental health facilities, Ethiopia, 2016.
The result of this study shows that about 20 (13.4%) of respondents gave immediate new born care under unclean delivery room, and most of 127 (94.8%) respondents timing for preparation of cord tie and cord clamping were before delivery (Table 6).
| Variable |
Frequency (N=134) |
Percent |
| Delivery room clean |
Yes |
114 |
86.6 |
| No |
20 |
13.4 |
| Cord tie and clamp prepared |
Yes |
127 |
94.8 |
| No |
7 |
5.2 |
| Baby identification material prepared |
Yes |
31 |
23.2 |
| No |
103 |
76.8 |
| Suction devise prepared |
Yes |
101 |
75.4 |
| No |
25 |
18.9 |
| Neonatal ambubag and mask prepared |
Yes |
108 |
80.6 |
| No |
26 |
19.4 |
Table 6: Preparation of equipment’s by health professionals to give immediate new born care in governmental health facilities, in Bahir Dar city, Ethiopia, 2016.
Among the total respondents 123 (90.8%) of respondents put on sterile glove before starting new born care, 100 (74.6%) of respondents did not washes hands with soap and water, dries them with a clean dry cloth or air dries them before and after care and 120 (89.6%) of respondent wiped the eyes and head when the head is delivered (Table 7).
| Variable |
Frequency (N=134) |
Percent |
| Washes hands with soap and water, dried with a clean dry cloth before and after care |
| Perform task |
34 |
25.4 |
| Unable to perform |
100 |
74.6 |
| Wipes the eyes and face when the head is delivered |
| Perform task |
120 |
89.6 |
| Unable to perform |
14 |
10.4 |
| Delivery surface covered with sterile dry towel |
| Perform task |
78 |
58.2 |
| Unable to perform |
56 |
41.8 |
| Deliver baby on mother abdomen |
| Perform task |
100 |
74.6 |
| Unable to perform |
34 |
25.4 |
| Cord tied one at two fingers from the baby’s abdomen and place the second tie at two fingers from the second tie |
| Perform task |
119 |
88.8 |
| Unable to perform |
15 |
11.2 |
| Cord cut with sterile scissor after 2-3 min under a piece of gauze |
| Perform task |
107 |
79.9 |
| Unable to perform task |
27 |
20.1 |
| Take Apgar Score within one hour after delivery |
| Perform task |
101 |
75.4 |
| Unable to perform |
33 |
24.6 |
Table 7: Practice of health professionals on immediate new-born care in Bahir Dar city, Ethiopia in 2016.
As shown from the graph, 116 (86.6) of respondents were immediately dry the whole body including the head and limbs with a cloth/towel while assessing the baby’s breathing. A total of 83 (61.9%) of respondents keep warm by putting the baby skin-to-skin contact with the mother putting a cap on the baby’s head and covering mother and baby together with a blanket (Figure 6). A total of 113 (84.3%) of respondents were initiated breast feeding within 1 h of delivery and 131 (97.8) were give vitamin K to newly born baby. From all participants of this study 103 (76.9%) were not placed new-born’s identification bands on the wrist and ankle of baby and 94 (70.1%) were counselled mother new-borns danger sign before discharge (Table 8).

Figure 6: Practice of health professionals on immediate new born care in Bahir Dar city, Ethiopia, 2016.
| Variable |
Frequency (N=134) |
Percent |
| Initiate breast feeding within one hour after delivery |
| Task performed |
113 |
84.3 |
| Unable to perform |
21 |
15.7 |
| Giving Vit. K to immediately born baby |
| Task performed |
131 |
97.8 |
| Unable to perform |
3 |
2.2 |
| Applying eye ointments |
| Task performed |
127 |
94.8 |
| Unable to perform |
7 |
5.2 |
| Helps mother and baby get in to a good position and attaches for breast feeding |
| Task performed |
79 |
59.4 |
| Unable to perform |
55 |
40.6 |
| Weighs the baby |
| Task performed |
129 |
96.3 |
| Unable to perform |
5 |
3.7 |
| Counsels mother how to bath baby |
| Task performed |
105 |
78.4 |
| Unable to perform |
29 |
21.6 |
| Responds to mothers question positively |
| Task performed |
120 |
89.6 |
| Un able to perform |
14 |
10.4 |
| Explain to mother not to put anything on cord stump |
| Task performed |
56 |
41.8 |
| Unable to perform |
78 |
58.2 |
| Place newborn’s Identification bands on the wrist and ankle |
| Task performed |
31 |
23.1 |
| Unable to perform |
103 |
76.9 |
| Records all care given on the birth record |
| Task performed |
125 |
93,3 |
| Unable to perform |
9 |
6.7 |
Table 8: Practice of health professionals on immediate new born care in Bahir Dar city health facilities, Ethiopia, 2016.
Generally our study result shows that work environment and their professional status affects the knowledge and practice level of health professionals (Table 9).
| Variable |
Knowledge level |
Practice level |
| Poor |
Fair |
Good |
Practiced |
Not practiced |
| Work environment |
|
| Hospital |
10 (12%) |
22 (26.5%) |
51 (61.4%) |
58 (69.8%) |
25 (30.2%) |
| Health center |
8 (15%) |
19 (37%) |
24 (47%) |
22 (43%) |
29 (57%) |
| Health profession |
|
| Midwife |
7 (17.5%) |
12 (30%) |
21 (52.5%) |
21 (52.5%) |
19 (47.5%) |
| Nurse |
8 (18%) |
12 (27%) |
24 (54%) |
19 (43%) |
25 (57%) |
| Doctor |
2 (4.7%) |
13 (30.9%) |
27 (64.2%) |
36 (85.7%) |
6 (14.3%) |
| Health officer |
1 (20%) |
1 (20%) |
3 (60%) |
3 (60%) |
2 (40%) |
| Emergency surgery |
0 |
3 (100%) |
0 |
1 (33%) |
2 (67%) |
Table 9: Cross-tabulation to show relation between work environment and health profession with knowledge and practice level in Bahir Dar city governmental health facilities, Ethiopia, 2016.
Discussion
Delivery and the first few hours of life are critical period for the further growth and development of infant, which is determined by the quality of care that new-born receives [1].
The immediate care of new-born is performed for saving the newborn life so 62.7% of respondents had received in service training courses on immediate care of newborn, in spite of this; the study populations of this survey had poor knowledge regarding care of new-born at birth (13.4%). Similar study done in Tigray regional state shows that 126 (85.7%) received in-service training regarding immediate newborn care but 25.2% had poor knowledge and in Sudan study shows that 93% of study population had training but 56.6% of them got poor knowledge [1]. This might be due to participation of Doctors, Health Officers and Emergency Surgeries in our study.
Practice of respondents towards immediate newborn care in this study were 59.7% which is slightly higher than that was found in the study done in Tigray Ethiopia and Sudan Khartoum which is 52.4% and 41.1% respectively [1,2]. This might be due to the descriptive statistics used at both study areas, that is the study done in Sudan had taken mean whereas in this study practice was calculated from median.
This study that 74.6% of health professionals placed immediately born baby on mother’s abdomen, 94% immediately dried the whole body of the baby with a cloth and 54.9 removed wet cloth used to dry the baby; a study done in Tigray regional state showed that 95.9% of midwives placed immediately born baby on mother’s abdomen and 98.6% immediately dried the whole body of baby with a cloth. Of this 90.5% removed wet cloth used to dry the baby [1] and a similar study done in Tanzania by MAISHA program and 77% in 2012 immediately placed newborn on the mother's abdomen, 91% in 2010 and 95% in 2012 immediately dried baby with towel and 93% in 2010 and 93% in 2012 discarded wet towel [8].
The difference might be related to the in-service training received on immediate care of newborn is lower as compared to other studies.
Regarding knowledge of cutting umbilical cord 91.1% of respondents in this study were used sterile scissor to cut the umbilical cord of baby between clamps; a study in Ethiopia showed that 100% of respondents were used sterile scissor to cut the umbilical cord of baby between clamps [2]. Clean cord cutting and care minimizes infection and further complication of newborn baby. Most respondents in both study area are aware of the infection a newborn baby will acquired during cord cutting. This might be due to work experience of the respondents that is work experience of our study participants was relatively lower than other studies and availability of the cutting material.
In this survey 61.9% practiced Keeping baby warm by putting skin-to-skin contact with the mother. This study finding is comparatively lower than similar study in Tigray regional state where 72.1% practiced it [2] and comparatively higher than a study done in Haryana, India where 67% respondents had heard about skin to skin contact but only 57% of them knew how to do it and only 5% practiced it [9]. Practicing skin to skin contact could make the newborn baby prevented from neonatal complication (hypothermia) and reduces other complications which follow hypothermia. The difference might be related to the in-service training received on immediate care of newborn and government concern.
The finding of this study showed that 97.8% of respondents had knowledge on the advantage of early initiation of breast feeding, 99.3% had knowledge on advantage of first milk/ colostrum’s and but 85.1% started to initiate breast feeding to the baby within 1 h after delivery. A similar study shows that 97.3% had knowledge on advantage of first milk/colostrum. Among this, 76.2% of respondents practiced to initiate early breast feeding to immediately born baby [2]. This difference might be due to good educational level of respondents that is in this study Degree were higher than diploma.
Babies born with the help of respondent health professionals in this study will benefit from the advantage of early initiation of breast feeding and from colostrum’s that will have strong bonding with their mother and could be free from infections and nutrition related problems. This might be due to increased concern of government and other nongovernmental bodies on early initiation of breast feeding.
Concerning with knowledge of providing eye ointment 99.2% of respondents in this study apply TTC for immediately born baby and 95.5% practiced it. This result is relatively consistent with those studies in Tigray regional state where 99.3% practiced to apply eye ointment to immediately born baby [2].
Regarding knowledge of health professionals towards importance of vitamin K about 85.8% of the respondents were knowledgeable and 97.8% of Health professionals practiced of giving vitamin K to immediately born baby; and this is slightly higher than study done in Egypt which revealed that 30.5% of midwives administer vitamin K to the immediately new born baby [10] and a study done in Haryana India 76% of study participants had good knowledge of importance of vitamin K and only 55% had practice of giving vitamin K to immediately born baby [9]. Small number of respondents in this study was gave vitamin K without knowing its importance, this might be due to strong emphasis given by ministry of health on maternal and newborn care and supply of vitamin K to the health facilities.
About 23.1% of participants in this study were not practiced to put baby identification bands on the wrist and ankle of baby after delivery. This is better than the study done in Tigray regional state, was 99.3% of respondents not practiced [2], this is similar with the study in Khartoum, Sudan, were 2.1% of nurse midwives were put baby identification bands before cutting the cord [1]. This will increases misshaping or exchange of babies in busy delivery room or time. This might be related to the careless behaviour of respondents on using newborns identification on both areas and availability of the material.
Regarding response of health professionals to mother’s question, 90.3% of respondents respond positively to and 70.1% were counsel’s mother new-born’s danger sign. But this study is higher than the study in Egypt, were 52.2% respond to mother’s questions [10]. Responding positively to mother’s question might increase delivery service at health facilities and increases care provided for newborn baby and counselling mother on newborn danger sign causes the mother to appreciate newborn complication and take appropriate measures on time which decreases further problems a baby will face. This might be due to increased commitment of the health facilities to give health education for mothers.
Conclusion
Almost all health professionals who responded for this study had gap on where to place the newly born baby and putting of identification band on the baby’s wrist or ankle.
Significant number of health professionals did not practice well cord tie and cuts cord soon after delivery. Cutting the cord soon after delivery can decrease the amount of blood that is transfused to the baby from placenta; it is likely to result in subsequent and repeated infections.
Most respondent’s health professionals didn’t wash hands with soap and water before and after delivery and a significant number of health professionals conducted delivery under unclear delivery room. This could facilitate transmission of infection to the mother, newborn baby, and health care provider and may affect the future health of baby.
Recommendation
Based on the result findings from this study, the following recommendations are forwarded:
• Strengthen in-service training given to health professionals on immediate newborn care periodically and regularly, for governmental and nongovernmental health organizations.
• Upgrade educational status of those health professionals giving immediate newborn care, for regional health bureau.
• Provide motivation to those who have knowledge and practiced well on the care given immediately after delivery, for health facility leaders.
• Education curriculum for the student should be including all steps given to immediately born baby, for college of medicine and health science.
• Further detail investigation on knowledge and practice of health professionals on immediate newborn care, for anyone who is interest.
Strength and Limitation of the Study
Strength of the study
• Instruments (Questionnaire) used to collect data was adopted from previously published study with required modification after pretested.
• Strict supervision by principal advisors.
Limitation of the study
Due to the limitation of time allocated and budget constraint
• we did only in Bahir Dar City had it been all over the region covering large area it would be very nice
• only studied the descriptive part but it would be very nice and broad and specific if we add associated factors
Declaration
The authors declare that the undersigned agrees to that this research finding is the original article and there is no conflict of interest regarding the publication of this paper.
References
- Ali F, Taha N. Assessment of knowledge, attitude and practices of nurse midwives towards immediate care of the new-born in Khartoum state teaching hospitals. J Am Sci 2013; 9.
- Tsegaye T. KAP of immediate new born care among midwives. University Addis Ababa 2015.
- Chuni N, Chandrashekhar TS. Early pregnancy termination with a simplified mifepristone – medical abortion outpatient regimen. Kathmandu University Medical Journal 2009; 3: 331.
- Cunningham F, Leveno K, Bloom S, Hauth J, Rouse D. William Obstetrics (23rd Ed). Med Health Sci 2010; 8: 590.
- Gurung G. Practices on immediate care of new-born in the communities of Kailali district. Nepal Med Coll J 2008; 10: 41-44.
- Dalia T, Asma H. Assessment of standards of quality care and nurse’s performance in neonatal units at governmental hospitals in the West Bank. 2011.
- World Health Organization (WHO). Managing complications in pregnancy and child birth. WHO, Geneva 2000.
- MAISHA program. MAISHA Quality, Joseph dy of maternal and new-born care study. Key findings: Immediate essential new-born care and resuscitation. Tanzania 2010-2012.
- Louis D, Kumar P, Gupta A. Practitioners’ series knowledge and practices of healthcare providers about essential new-born care and resuscitation In a district of Haryana. J Indian Med Assoc 2013; 111.
- Abd El Fattah N, El Dein NAZ. Assessment of quality of nursing care provided immediately after birth at university hospital in El kom-Minoufiya, Egypt. Life Sci J 2012; 9.

