Abbreviations
OA: Osteoarthritis; HRQOL: Health-Related Quality of Life; TKA: Total Knee Arthroplasty
Introduction
Osteoarthritis (OA) is a degenerative, disabling and multifactorial disease with a high prevalence that increases exponentially with age1-3. It is divided into categories as primary or secondary Osteoarthritis, depending on the related cause2. It mainly affects weight bearing joints such as knees and hips, which are the most frequently affected areas1. Knee osteoarthritis is more disabling than any other orthopedic and musculoskeletal disorder2.
The impact of osteoarthritis is huge regarding suffering, function loss and use of social-health resources. Also, it worsens well-being and Health-Related Quality of Life (HRQOL) in its physical, emotional and social aspects2. Consequently, it is important to know the impact of this condition on HRQOL in order to make therapeutic decisions in the context of health policies related to the efficiency and sustainability of the health system4.
Health-Related Quality of Life is expressed as the degree of perception to which the disease or its treatment affects the physical, psychic, emotional and social abilities of an individual5. It is a global index of clinical results in the field of Health which makes it possible to associate the therapeutic/ surgical objectives with the results obtained in the individual and social spheres of the patient. Also, it can be measured with generic or specific health questionnaires6.
On the other hand, total knee arthroplasty (TKA) is the orthoprosthetic operation with the highest clinical success rate, with good prognosis and sustained clinical results in over 95% of the patients after 10 years. Also, it reduces pain and improves function and HRQOL7.
There are few reports on knee OA and its impact on HRQOL in Spain. In other Europe countries like Sweden and the United Kingdom, there are National Registers of Arthroplasty. These registers recover statistic information regarding prosthesis as well as Patient Reported Outcome Measures. This information is used to evaluate the Quality of Services and to plan clinicalbased- decision and cost/effectiveness analysis, thanks to the feedback obtained by this clinical-epidemiological process.
The objective of this study is to assess the influence of knee OA and its clinical intervention (TKA) from the perspective of the perception of the operated patient with regard to HRQOL. The hypothesis of this work is based on the fact that there are no statistically significant clinical differences between the clinical situation and HRQOL of patients with knee osteoarthritis before and after the operation.
Methods
In order to reach our objectives and prove our hypothesis, a quasi-experimental intervention study with a before and after design, was carried out. It is an experimental or intervention study on a sample of patients with knee osteoarthritis who were assessed before and after the operation of TKA. This type of epidemiological study has a good scientific evidence level, according to the categories and classification proposed by the Task Force US and the Centre for Evidence Based Medicine (CEBM) of Oxford8,9.
The clinical research was carried out in the Health Area of Salamanca, which comprises the Clinical University Hospital of Salamanca, and it included all patients with severe knee osteoarthritis who were referred by Primary Care Doctors in order to assess the possibility of a surgical operation.
Our series was made up of 125 patients (46.8%) out of a total of 267 patients. They were all operated by the same orthopedic surgeon and with the same type of prosthesis (Scorpio-Stryker®) between the years 2008 and 2012. All the patients filled out the SF-36 survey before and after the operation, and their clinical history was reviewed in order to obtain the independent variables related with HRQOL, such as age, sex, comorbidities, other arthroplasty, other operations on the locomotor system, and in-hospital stay.
The criteria for inclusion as CASES were: adult patients of any age and sex with a diagnosis of osteoarthritis of the knee who were operated with TKA type Scorpio and/or with diverse comorbidities. The criteria for exclusion were: patients with disorders and/or pathologies that prevented them from knowing, understanding or assessing their clinical situation. Also those in which it was impossible to obtain updated personal data or who failed to attend the post-intervention interview in which the questionnaire was filled out, after the first post-intervention visit, which took place after 2 to 3 months. As a consequence, some cases were lost during the study because they failed to attend, or due to a severe disease caused by any of their comorbidities, death or any other social reason.
The collection of data was carried out with a Clinical and Epidemiological Protocol created by the research team for this study and filled out during a personal interview to each patient. In the assessment of HRQOL we used the SF-36 questionnaire, due to its characteristics of viability, reliability, sensitivity to change and transcultural validation in Spain10,11.
SF-36 is the most widely used generic questionnaire in the world because it makes it possible to compare the impact/result of an intervention, and it has been used with different chronic diseases and in different population groups12. SF-36 measures HRQOL, it provides a profile of the health condition that can be applied to the general population and to the patients, as well as in studies that assess clinical results. It is also used in musculoskeletal and orthopedic clinical studies to obtain a more detailed description of the Health parameters and to research changes in the health condition13-15.
The data collected from the clinical histories and the results of the SF-36 questionnaire were introduced and coded for processing and analysis with the statistical package SPSS® version 21. The statistical analysis included, first of all, a descriptive study (univariate analysis) which calculated the adequate frequency measures to assess the different indexes and indicators, as well as the subsequent descriptive statistics (mean value, standard deviation). Once that the different data were obtained, together with their prevalence and/or proportions we calculated their 95% confidence interval as a measure of precision (Inferential statistics). Chi-square test was used for the qualitative variables and Student’s t-test and ANOVA were used for quantitative variables in order to assess whether the differences observed in the clinical parameters and the components of the SF-36 and other indicators and the abovementioned epidemiological variables regarding the patients were statistically significant or, on the contrary, they could be explained by chance. Finally, a logistic regression model was used so as to assess the influence of the presence or absence of several clinical and epidemiological variables on HRQOL (bivariate and multivariate analysis). The level of statistical significance (error) used by the research team was 5% (degree of statistical significance p<0.05).
Results
The distribution according to sex in our 125 cases was 78 women (62%) and 47 men (38%), with a 1.6:1 man/woman ratio and an average age of 70 years (Figure 1). The most common age was 71 years, with a range between 37 and 86 years (Figure 2). The average time of in-hospital stay was 8.12 days; the most common value was 8 days, and the range was between 4 and 13 days (Figure 3).
Figure 1: Sex as a demographic variable in the analyzed sample.
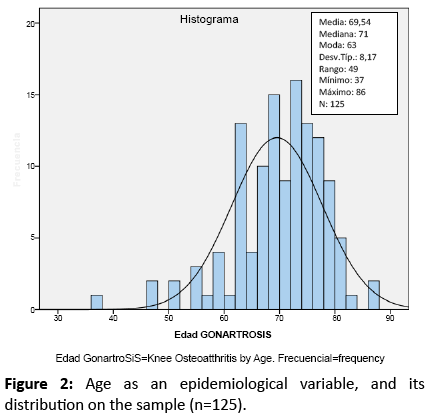
Figure 2: Age as an epidemiological variable, and its distribution on the sample (n=125).
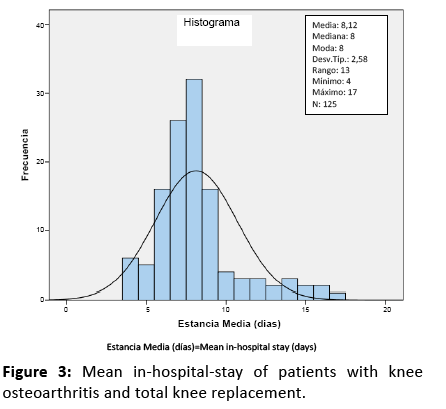
Figure 3: Mean in-hospital-stay of patients with knee osteoarthritis and total knee replacement.
Half of our patients had a prior orthoprosthetic history. 33% had TKA, 13% had a THA (total hip arthroplasty), and 2.5% had both prostheses (Figure 4). Also, 20% of the patients had a prior history of operations in the locomotor system and 31.2% of the patients had a history of other prior surgery.
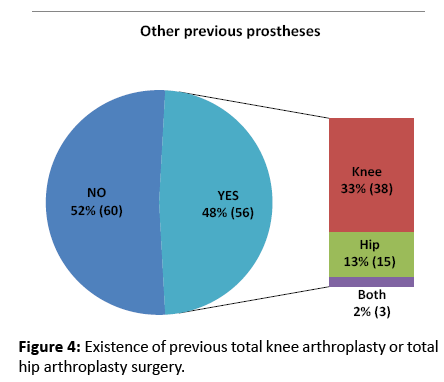
Figure 4: Existence of previous total knee arthroplasty or total hip arthroplasty surgery.
With regard to comorbidity, 95 patients (76%) showed associated comorbidity, 28 patients (22.5%) presented with a single comorbidity and 67 patients (53.6%) revealed two or more comorbidities. Also, in 17 patients (15%), the comorbidity was musculoskeletal and 92 patients (81%) showed other comorbidities.
We have observed that osteoarthritis significantly affects all the dimensions of quality of life (before the intervention). All the dimensions of the SF-36 questionnaire reveal a clinical improvement after the operation (TKA) (Figure 5).
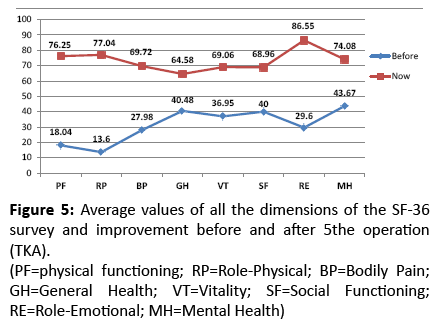
Figure 5: Average values of all the dimensions of the SF-36 survey and improvement before and after 5the operation (TKA).
(PF=physical functioning; RP=Role-Physical; BP=Bodily Pain; GH=General Health; VT=Vitality; SF=Social Functioning; RE=Role-Emotional; MH=Mental Health)
The association study of HRQOL-SF-36 before and after the operation shows a statistically significant improvement in the scales Bodily Pain (BP p=0.000), General health (GH p=0.000), Vitality (VT p=0.005), Social Functioning (SF p=0.000), Role- Emotional (RE p=0.050), and Mental Health (MH p=0.000). One significant aspect is that the operation (TKA) causes no improvement in Physical Functioning (PF p=0.295) and in Role-Physical (RP p=0.385) (Table 1). We have also observed that having a prior knee or hip prosthesis improves Physical Functioning (PF p=0.021) and Mental Health (MH p=0.036).
| |
Before |
After |
Parametric test |
| ITEMS AND DIMENSIONS |
Average |
St. Dev |
Average |
St. Dev. |
p |
| SF-3 |
10.40 |
25.63 |
67.74 |
39.91 |
0.004 |
| SF-4 |
19.20 |
30.96 |
78.63 |
31.34 |
0.385 |
| SF-5 |
22.00 |
33.23 |
75.20 |
30.95 |
0.285 |
| SF-6 |
7.60 |
20.13 |
63.64 |
36.51 |
0.217 |
| SF-7 |
21.77 |
31.39 |
79.84 |
30.52 |
0.219 |
| SF-8 |
8.74 |
21.82 |
63.71 |
36.81 |
0.241 |
| SF-9 |
13.20 |
28.50 |
79.03 |
35.55 |
0.500 |
| SF-10 |
20.80 |
31.22 |
79.03 |
31.94 |
0.159 |
| SF-11 |
32.40 |
37.70 |
87.50 |
26.76 |
0.098 |
| SF-12 |
30.40 |
40.60 |
87.50 |
26.76 |
0.149 |
| DIMENSION Physical Functioning (PF) |
18.04 |
22.12 |
76.25 |
24.73 |
0.295 |
| SF-13 |
16.80 |
37.53 |
79.67 |
40.40 |
0.064 |
| SF-14 |
12.80 |
33.54 |
75.00 |
43.47 |
0.064 |
| SF-15 |
15.20 |
36.04 |
77.42 |
41.98 |
0.211 |
| SF-16 |
9.60 |
29.57 |
77.24 |
42.10 |
0.599 |
| DIMENSION Role-Physical (RP) |
13.60 |
29.70 |
77.04 |
37.42 |
0.385 |
| SF-21 |
27.36 |
21.33 |
69.44 |
23.35 |
0.247 |
| SF-22 |
28.60 |
18.97 |
70.00 |
23.54 |
0.734 |
| DIMENSION Bodily Pain (BP) |
27.98 |
17.35 |
69.72 |
20.83 |
0.000 |
| SF-1 |
24.80 |
19.69 |
55.08 |
23.07 |
0.001 |
| SF-33 |
49.40 |
28.41 |
72.38 |
19.60 |
0.000 |
| SF-34 |
46.57 |
27.66 |
67.94 |
19.27 |
0.000 |
| SF-35 |
41.53 |
21.82 |
62.70 |
20.53 |
0.000 |
| SF-36 |
39.92 |
24.47 |
64.43 |
21.94 |
0.001 |
| DIMENSION General Health (GH) |
40.48 |
19.05 |
64.58 |
15.28 |
0.000 |
| SF-23 |
37.76 |
25.68 |
65.60 |
22.66 |
0.345 |
| SF-27 |
38.21 |
27.22 |
69.35 |
20.94 |
0.000 |
| SF-29 |
35.45 |
28.03 |
72.26 |
19.20 |
0.000 |
| SF-31 |
36.29 |
25.16 |
68.55 |
21.66 |
0.099 |
| DIMENSION Vitality (VT) |
36.95 |
21.84 |
69.06 |
17.11 |
0.005 |
| SF-20 |
45.00 |
30.94 |
77.62 |
22.27 |
0.000 |
| SF-32 |
34.84 |
22.93 |
60.32 |
15.71 |
0.000 |
| DIMENSION Social Functioning (SF) |
40.00 |
25.45 |
68.96 |
16.58 |
0.000 |
| SF-17 |
28.80 |
45.46 |
87.90 |
32.74 |
0.008 |
| SF-18 |
28.00 |
45.01 |
85.48 |
35.36 |
0.005 |
| SF-19 |
32.00 |
46.83 |
86.29 |
34.53 |
0.014 |
| DIMENSION Role-Emotional (RE) |
29.60 |
43.62 |
86.55 |
32.06 |
0.050 |
| SF-24 |
45.00 |
31.19 |
76.64 |
17.54 |
0.000 |
| SF-25 |
46.34 |
32.11 |
79.52 |
16.55 |
0.000 |
| SF-26 |
38.70 |
25.44 |
68.16 |
22.01 |
0.000 |
| SF-28 |
47.32 |
30.75 |
76.13 |
17.42 |
0.000 |
| SF-30 |
41.77 |
28.17 |
70.00 |
21.86 |
0.000 |
| DIMENSION Mental Health (MH) |
43.67 |
26.15 |
74.08 |
14.35 |
0.000 |
| Health Transition ItemSF-2 |
35.04 |
27.01 |
68.13 |
22.67 |
0.041 |
Table 1: Association HRQOL-SF36 before and after the intervention.
Discussion
Knee osteoarthritis is one of the diseases with the highest impact regarding the functional disability, and one which greatly affects the personal autonomy of patients. Also, its incidence increases with age and it affects more than 33% of people over 70 years in Spain16. The average age in our series at the time of operation is 70 years, and the age distribution shows a normal curve, in accordance with national studies which have shown average ages of 66.5 ± 6.2 years17,18 and 74 ± 2.3 years19-21, with a progressive ageing in the population. International studies have reported ages of 68 years21 and 72 years22. Consequently, the average age of the patients who were operated and monitored in our series is higher, due to the social and demographic characteristics of the general population of reference, which corresponds to the area of the city and province of Salamanca, part of the Autonomous Community of Castile and León, which has one of the highest indexes of population ageing in Spain.
Osteoarthritis usually affects the knee, and its incidence increases exponentially with age, with a clear predominance on women. The observed women/men ratio is 1.6:1, in accordance with other national studies, with ratios of 2.7:115, 3:117-19, 4:116, 4.9:120; and with international studies, with ratios of 1.5:122, 1.6:123, and 2.2:121.
Adult and symptomatic patients with osteoarthritis generally have more than one affected weight bearing joint, be it the knee, the hip or a similar contralateral joint24. Some experts also report that 90% of the patients with knee pain report bilateral symptoms. With regard to the presence of previous joint prostheses, all the studies report an orthoprosthetic history. In our series, 33% of the patients had a previous prosthesis in the knee, 13% in the hips and 2% in both. National studies have revealed contralateral surgery in 24.6% of the patients <75 years old and 33% in patients >75 years old20; and other international studies have found contralateral surgery of the knee in 17%25 of the patients; in 20% of the patients <80 years old and in 54% of the patients >80 years old, and 35% of the patients showed THA26. These results prove that osteoarthritis is a bilateral condition that particularly affects weight bearing joints. All the studies reveal orthoprosthetic records similar to those of our series and these records are higher in older groups. The results observed in patients with previous prosthesis of the knee or the hips are associated with a faster and steadier improvement of Physical Functioning and Mental Health, and this improvement may be due to the better mental predisposition of the patients caused by the previous surgical experiences and by the process of adaptation to living with prosthesis.
The average in-hospital stay in our study is 8.2 days, with a range between 4 and 17 days. All the studies that have been carried out, both national16,20 and international27,28, show similar periods of average in-hospital stay, and they all report a decreasing evolution of this factor. This decrease has been made possible thanks to the improvements in the surgical techniques and the program for immediate postoperative rehabilitation treatment which has been implemented in the medical-surgical protocols in order to improve the quality of the care process, its effectiveness and efficiency.
Regarding HRQOL, we have observed a clinical improvement in all the dimensions of the SF-36, and this improvement is significant in all sections except for Role- Physical and Physical Functioning. This result may seem in conflict with what was reported by other experts on TKA, who state that it substantially improves Physical Functioning, as published by some researchers21, and it is only observed in patients with a previous prosthesis. Nevertheless, it may be due to the conditioning of age and comorbidity, which are variables that affect the immediate postoperative period in which the HRQOL questionnaires were filled out. This means that patients need more time to notice a significant clinical improvement with regard to Physical Functioning (PF). Some authors state that a previous joint prosthesis does not lead to worse results after the operation, as was observed in our series22. Other researchers have observed that preoperative factors are predictors for mobility and results27,29,30.
In line with what was observed in our series, most of the studies14,16,21,22,24,26 report that total replacement arthroplasty improves pain, Physical Functioning, Mental Health, Social Activity and HRQOL. Knee osteoarthritis produces limitations in Activities of Daily Living and therefore limits social functioning, and although after the operation there is an improvement in all other dimensions, and particularly pain and physical functioning, it is difficult for older patients to recover the lost social functioning due to their advanced age and the fact that they have comorbidities, as has already been shown by other studies31-33.
On the other hand, when the results from the different components of HRQOL in SF-36 in our series are compared with the general population in Spain11, which is our standard population of reference, only Social Functioning is lower, while five of them show similar levels and two of them, Role-Emotional and Mental Health, show an improvement. Consequently, we can state that the operation of total knee arthroplasty is justified according to the perception of clinical improvement and the improvement of HRQOL reported by the patients.
Conclusion
According to what was observed in this study, our typical patient is a 70 year old woman with a previous prosthesis, comorbidity and knee osteoarthritis that affects her HRQOL, we can state that TKA significantly improves HRQOL in all its dimensions and components, except for Physical Functioning and Physical-Role, although they also improve over time after the operation.
Competing Interests
Each author certifies that he or she has no commercial associations that might pose a conflict of interest in connection with the submitted article. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Author’s Contribution
ME Fernández-Cuadros participated in acquisition of patients’ data, drafting and designed of the article and analysis and interpretation of results. OS Pérez-Moro participated in acquisition of patients’ data. JA Mirón-Canelo participated in the conception and design of the study, designed the manuscript, supervised and interpretation of results.
All authors read and approved the final version of the manuscript.
Acknowledgments
In memory of Dr. José Antonio de Pedro-Moro, Surgeon and Professor of Salamanca’s University Hospital, responsible for the study design and the surgical treatment of the sample that constituted this quasi-experimental study. Without his help this clinical research could not be accomplished.
References
- Thandi Puoane, Lungiswa, David Sanders and Whadiah Parker. Chronic Non-Communicable Diseases. South Africa.
- World Health Organization (WHO).Non communicable disease. Available from: https://www.who.int/mediacentre/factsheets/fs355/en/ (accessed in Oct.14 2015 at 01:25 am)
- World Health Organization (WHO). Chronic diseases and health promotion. Available from: https://www.who.int/chp/en/(cited 2015-09-05).
- World Health Organization (WHO). Chronic Diseases. Available from: https://www.who.int/topics/chronic_diseases/en(cited 2015-09-04).
- Centers for Disease Control and Prevention (2015) (CDC). CDC Global Noncommunicable Disease (NCDs). Available from:https://www.cdc.gov/globalhealth/healthprotection/ncd/(accessed in Oct.14 2015 at 01:31am)
- Stephanie Lauvergeon, Bernard Burnand and Isabelle Peytremann (2012) Chronic disease management: A qualitative study investigating the barriers, facilitators and incentives perceived by Swiss healthcare stakeholders, 12:176).
- Grant M. Russell, Simone Dabrouge, William Hogg, Robert Geneau, Laura Muldoon and Meltem (2009). Managing Chronic Disease in Ontario, Primary Care: The Impact of Organizational Factors. Ontario, Canada, Vol.7, No.4).
- Canadian Family Physician. Use of Chronic disease management tools. Available from: https://www.ncbi.nlm.gov/pmc/articles/PMC3237522(cited 5/09/2015).
- Unwin N, and Alberti KG (2006). Chronic non-communicable diseases .Newcastle. UK; 100(5-6):455-64. Available from: https://www.ncbi.nlm.nih.gov/pubmed/16899148(accessed Oct 14 2015 at 12:24 am).
- J.N Struijs (2008). The future health (care) burden of chronic diseases in the Netherlands (PhD Thesis). Netherlands.
- Hani Abdeen (2006). Chronic Diseases in Palestine: The Rising Tide: Israeli-Palestinian Public Health Magazine (Bridges). Volume 2, Issue 3.
- Heidar Abu Ghosh, Jihad Mashal, NadimBarghuti and SuheilAqabneh (2007). Diabetes Control in 3 Villages in Palestine: A Community-Based Quality Improvement Intervention. J Ambulatory Care Manage.Vol. 30, No. 1, pp. 74-78.
- WAFA-Palestinian News & Info Agency. Available from: https://english.wafa.ps/index.php?action=detail&id=22068(accessed 6 Oct. 2015).
- Palestinian Medical Relief Society (PMRS) (2003). Enhancing the Capacity of Primary Healthcare Clinics to Better Manage None-communicable Diseases. Palestine.
- Dodhia H and Phillips K (2008) Measuring the burden of disease in two London boroughs using Disability Adjusted Life Years (DALYs). London, UK, Vol.30, No.3,pp: 313-321.
- Brecht D, Arie H, Charline M and others (2014) Calculating disability-adjusted life years to quantify burden of disease. SSPH+ Swiss.
- Genova-Maleras R, Alvarez-Martin E, Morant-Ginestar C (2012). Measuring the burden of disease and injury in Spain using disability-adjusted life years (DALYs): An updated and policy-oriented overview. Spain. I024-I03I.
- Palestinian Central Bureau of Statistics (PCBS) (2016). Palestinian Family Survey 2010. Available from: https://www.pcbs.gov.ps/PCBS-Metadata-en-v4.2/index.php/catalog/168/study-description. (Cited in 10 march, 2016).
- Palestinian Health Information Center- Ministry of Health (MOH) (2011). Annual Health report; West Bank, Palestine.
- Palestinian Health Information Center- Ministry of Health (MOH) (2011). Annual Health report; Gaza Strip, Palestine.
- WIKIPEDIA. Disability-adjusted Life Years. Available from: https://en.wikipedia.org/wiki/Disability-adjusted_life_year (accessed 14 Oct2015).
- Disabled World. What is Disability Adjusted Life Year (DALY) (2015). Available from: https://www.disabled-world.com/definitions/daly.php (accessed 14 Oct2015)
- World Health Organization (WHO) (2015). Health statistics and information systems (National tools). Available from: https://www.who.int/healthinfo/global_burden_disease/tools_national/en/ (accessed 14 Oct.2015).
- C Murray, A Lopez and D Jamison (1994). The global burden of disease (GBD) in 1990: sensitivity analysis, Summary results, and future directions. (WHO). 72, 429-445.
- Dele OA, Colin DM, Taghreed A (2007). The burden and costs of chronic diseases in low-income and middle-income countries. Lancet; 370:1929-38.
- Food and Agriculture Organization of the United Nations (FAO) (2015). Nutrition assessment. Available from: https://www.fao.org/food/nutrition-assessment/nutrition-country-profiles/near-east/palestine/en/(accessed 18).
- Ministry of Health(MOH) (2014). Non-communicable disease and risk factors: global epidemics. Ramallah, Palestine.
- Palestinian Health Information Center- Ministry of Health (MOH) (2012). Annual report -MOH. Palestine.
- Mousa H, S Yousef, Riccardo F (2010). Hyperglycemia, hypertension and their risk factors in Palestine refugees served by UNRWA. 2010, EMHJ. Vol. 16 No.6.
- Lancet. Non-communicable diseases in Arab countries- Lancet. 2014.
- UNRWA. Annual Health report 2014 (2014) -department of health. Amman, Jordan pp: 37-38.
- Ministry of Health(MOH) (2013). Annual Health report of primary health care services. Gaza strip-Palestine. p.11-12.
- Institute for Health Metrics and Evaluation (IHME) (2010). Global Burden of Diseases, injuries and Risk Factors Study, Palestine.

