Tatsuya Kin, James Shapiro, Edmond A Ryan, Jonathan RT Lakey
Clinical Islet Transplant Program, University of Alberta and Capital Health Authority, Edmonton, Alberta, Canada
- *Corresponding Author:
- Jonathan RT Lakey
1074 Dentistry/Pharmacy Building
University of Alberta
Edmonton, Alberta
Canada T6G 2N8
Phone: +1-780.492.3077
Fax: +1-780.492.6335
E-mail: jlakey@ualberta.ca
Received February 18th, 2005 - Accepted March 17th, 2005
Keywords
Abnormalities; Diabetes Mellitus; Islets of Langerhans
Abbreviations
IE: islet equivalent
INTRODUCTION
Annular pancreas is a rare congenital anomaly formed by a thin band of normal pancreatic tissue that completely or partially encircles the second portion of the duodenum. During embryonic development, the ventral pancreatic primordium moves to the right and rotates posteriorly until it comes to lie to the left of the duodenum, subsequently fusing to the dorsal primordium. Annular pancreas is believed to be due to a defect in the normal rotation of the ventral primordium [1]. Although the genetic and molecular basis for this anomaly remains obscure, Indian hedgehog or sonic hedgehog inactivation in mice has been shown to cause overgrowth of ventral pancreatic tissue, a phenotype strikingly similar to annular pancreas [2].
Since 1986, our Clinical Islet Transplant Program at the University of Alberta has obtained more than 900 human pancreata from cadaveric donors for islet isolation. We report our first case of islet isolation and transplantation from an annular pancreas.
CASE REPORT
A 32-year-old male who did not have notable medical history was admitted for head trauma secondary to a vehicle accident. The laboratory tests including serum amylase levels were within normal range. After diagnosis of brain death and obtaining consent, his pancreas was procured at a distant hospital and sent to our laboratory. The pancreas was preserved by the two-layer method for 11.5 hours prior to islet isolation.
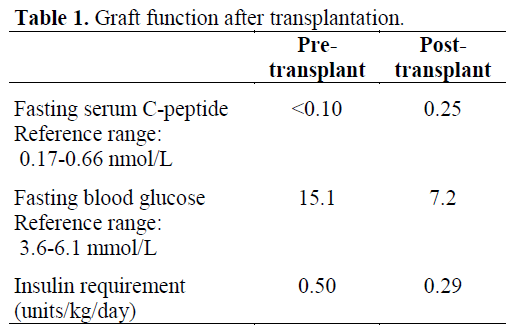
Upon arrival, the organ was visually inspected as usual and diagnosis of annular pancreas was easily made based on its anatomical structure (Figure 1). Any other abnormal findings were not observed. Two catheters (16 G) were inserted into the main duct and directed towards the head and tail of the pancreas following dissection of the main duct in the mid-body of the pancreas. Then the pancreas was distended with collagenase solution through the catheters. During the 10 min of intraductal delivery of enzyme, uniform distension of the gland, including the ring of pancreatic tissue was observed. Leakage of the solution was observed only from the orifice of Wirsung’s duct. The orifice of Santorini duct was not detected. The pancreas was transferred to a digestion chamber device for mechanical and enzymatic digestion. There was 13.7 g of undigested tissue remaining in the chamber after digestion, while initial weight of the pancreas was 110.2 g. Islet yield after digestion was 388,365 islet equivalent (IE). Islets were purified by continuous gradients of Ficoll using a refrigerated cell processor. After culture for 18 hours and subsequent repurification of less pure preparation, a total of 276,064 IE were recovered in 4.0 mL of pelletted volume. The viability of the islet tissue was 92% as measured using a membrane integrity test (SYTO-13/ethidium bromide) [3]. The islets were transplanted into a type 1 diabetic patient. Islet infusion was clinically uneventful and did not significantly affect portal pressure. Immediate islet function was demonstrated by the rapid elevation of serum C peptide, and confirmed by the significant decrease in the daily dose of exogenous insulin (Table 1).
Figure 1. Photograph of the annular pancreas during
intraductal collagenase perfusion.
DISCUSSION
Annular pancreas is an extremely rare anomaly, with an incidence of three in 20,000 autopsies [4]. During the past 19 years, we obtained more than 900 pancreata from braindead donors for islet isolation, and this is the first case of annular pancreas we encountered. The coexistence of annular pancreas with pancreas divisum is well documented [1]. Previous studies have demonstrated a higher frequency of pancreas divisum in individuals with annular pancreata than in the general population [5]. In our case, the donor did not have pancreas divisum, as the orifice of Santorini duct was obliterated.
To our knowledge, this is the first reported case of an islet isolation and transplantation from an annular pancreas, although whole organ transplantation of an annular pancreas has been reported previously [6, 7]. Intraductal collagenase perfusion and uniform distention of the gland are crucial to pancreatic digestion during clinical islet isolation. Therefore, pancreata with parenchymal damage are not ideal for islet isolation. In cases of annular pancreas, special care must be taken to avoid parenchymal injury when dissecting the duodenum. Regarding cannulation methods, some centers employ a single catheter insertion from the head of pancreas. Our method of cannulation following exposure of the duct in the midpancreas seemed to enable to get adequate distention of the ring portion of the pancreas. In conclusion, we have reported a successful case of islet isolation and transplantation from an annular pancreas. Bearing in mind the shortage of donors, patients with this anomalous condition should not be excluded as potential organ donors.
References
- Ladd AP, Madura JA. Congenital duodenal anomalies in the adult. Arch Surg 2001; 136:576-84. [PMID 11343551]
- Hebrok M, Kim SK, St Jacques B, McMahon AP, Melton DA. Regulation of pancreas development by hedgehog signaling. Development 2000; 127:4905-13. [PMID 11044404]
- Barnett MJ, McGhee-Wilson D, Shapiro AMJ, Lakey JRT. Variation in human islet viability based on different membrane integrity stains. Cell Transplant 2004; 13:481-8. [PMID 15565860]
- Ravitch MM, Woods AC Jr. Annular pancreas. Ann Surg 1950; 132:1116-27. [PMID 14790583]
- Baggott BB, Long WB. Annular pancreas as a cause of extrahepatic biliary obstruction. Am J Gastroenterol 1991; 86:224-6 [PMID 1992639]
- Barone GW, Henry ML, Elkhammas EA, Tesi RJ, Ferguson RM. Whole-organ transplant of an annular pancreas. Transplantation 1992; 53:492-3. [PMID 1738944]
- Romagnoli J, Papalois VE, Hakim NS. Transplantation of an annular pancreas with enteric drainage. Int Surg 1998; 83:36-7. [PMID 9706515]


