Keywords
Amyloid; Arteriosclerosis; Biological Phenomena; Diabetes Mellitus; Glucose (toxicity); Insulin Resistance; Oxidation-Reduction; Prediabetic State
Abbreviations
Abbreviations 2hOGTT: two-hour 75 gram oral glucose tolerance test; ACE: American College of Endocrinology; ADA: American Diabetes Association; ADIA: amylin derived islet amyloid; AGE: advanced glycosylation endproducts; ARB: angiotensin receptor blocker; DECODE: Diabetes Epidemiology Collaborative analysis Of Diagnostic criteria in Europe; DHHS: Department of Health and Human Services; DPP: Diabetes Prevention Project; HMGCoA: 3 hydroxy- 3methylglutaryl-coenzyme A; HOPE: Heart Outcomes Prevention Evaluation; HSPG: heparan sulfate proteoglycan; IAPP: islet amyloid polypeptide; IFG: impaired fasting glucose; IGT: impaired glucose tolerance; ISTAPs: intermediate sized toxic amyloid particles; JNC: Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; LIFE study: Losartan Intervention For Endpoint reduction in hypertension study; NCEP: National Cholesterol Education Program; NHBPEP: National High Blood Pressure Education Program; ROS: reactive oxygen species; T2DM: type 2 diabetes mellitus; WOSCOPs: West of Scotland Coronary Prevention study
Background and Historical Perspective
It has now been a century (1901) since Eugene L Opie first described the presence of hyalinosis within the islets of the pancreas in patients with hyperglycemia [1, 2].
This hyalinosis has subsequently been identified as amyloid (Figure 1) and in 1987 two separate investigators in separate laboratories determined it consisted of the monomeric unit - islet amyloid polypeptide (IAPP) or amylin - which when aggregates and polymerizes forms amylin derived islet amyloid (ADIA) [3, 4, 5]. Amylin is a 37 amino acid polypeptide with an amyloidogenic portion between amino acids number 20 and 29 [6]. It is capable of forming amyloid due to a unique amino acid sequence with its associated secondary structural conformation that only occurs naturally in cats and monkeys which develop type 2 diabetes mellitus (T2DM) spontaneously similar to humans [6]. Amylin parallels insulin’s synthesis, secretion, and excretion and may be considered insulin’s fraternal twin of the mother beta cell [7]. The two may act in a synergistic manner in helping to understand insulin resistance, metabolic syndrome, and the progressive nature of T2DM [8].
Figure 1. Amyloid highlighted within a single islet.
ADIA forms between beta cells and between beta cells
and endothelial cells creating a diffusion barrier (space
occupying lesion) resulting in a secretory defect and an
absorptive defect surrounding islet capillaries.
Insulin Resistance and the Metabolic Syndrome
Insulin resistance describes the condition whereby there is a resistance to insulin mediated glucose uptake by cells and is central to the clustering of multiple metabolic abnormalities and clinical syndromes. The clustering phenomenon was first described by Kylin in 1923 when he described the clustering of three clinical syndromes: hypertension, hyperglycemia, and hyperuricemia [9]. In 1936 Himsworth [10] noted that a large number of diabetic patients were insulin insensitive. Yalow et al. in 1965 [11] were first to discover an insulin assay and reported that insulin resistance was a condition in which insulin does not produce the same glucose lowering effects seen in insulin-sensitive individuals. These concepts were rejuvenated and immortalized by Reaven in 1988 given as the Banting lecture [12]. The clustering phenomenon has gone by many names since Reaven first described the metabolic and clinical associations of the many names of Syndrome X [13, 14].
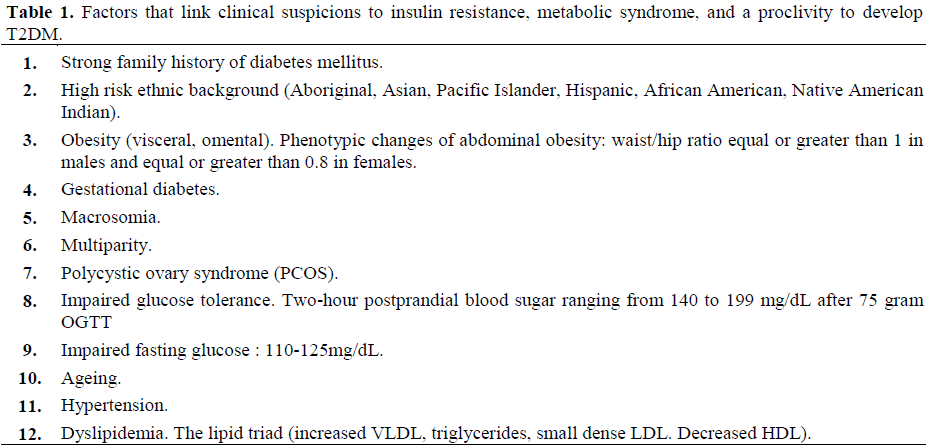
Additionally, there are at least a dozen factors that link clinical suspicions to the metabolic syndrome (Table 1). Factors and findings in this syndrome occur together all to frequently to be considered a coincidence and there are common underlying factors that may explain this coexistence. Namely, the well documented hyperinsulinemia story and the more recent hyperamylinemia and amylin derived islet amyloid story [13, 14, 15].
In 1999, the World Health Organization chose a unifying definition for this syndrome of many names and elected to use the term metabolic syndrome rather than the insulin resistance syndrome because they felt it was not well established that insulin resistance was the cause of all components of the syndrome [16]. Each of us probably have our own “pet term” that we commonly use for this clustering phenomenon but henceforth the appropriate term shall be referred to as the metabolic syndrome with no disrespect to any previous naming of this clustering phenomenon.
Metabolic syndrome affects approximately 47 million or greater Americans [17]. It is currently estimated that only 20% of patients with insulin resistance and hyperinsulinemiahyperamylinemia develop T2DM, while the remaining 80% are able to compensate at least for a period of time through the process of beta cell expansion, hypertrophy, and hyperplasia (utilizing the replicative pool of periductal cells) [18, 19].
Natural History of Type 2 Diabetes Mellitus
There are at least three diabetogenic factors: polygenic, environmental, and the endogenous histological structural defects associated with ADIA which interacts and contributes to the development and the progressive nature of T2DM (Figure 2) [13, 14, 15]. In addition to the contemporary widely accepted two hallmark features of insulin resistance and beta cell dysfunction there is a tight association of T2DM with obesity and sedentary life style.
Definition: “T2DM is a heterogeneous, multifactorial, polygenic disease characterized by a defect in insulin’s secretion (the beta cell secretory defect) and action (insulin resistance)”.
Figure 2. This figure demonstrates the ADIA changes
within the islet: The five stages in the natural history of
T2DM. Stages III and IV are incorporated together in
the newly named “prediabetic” stage.
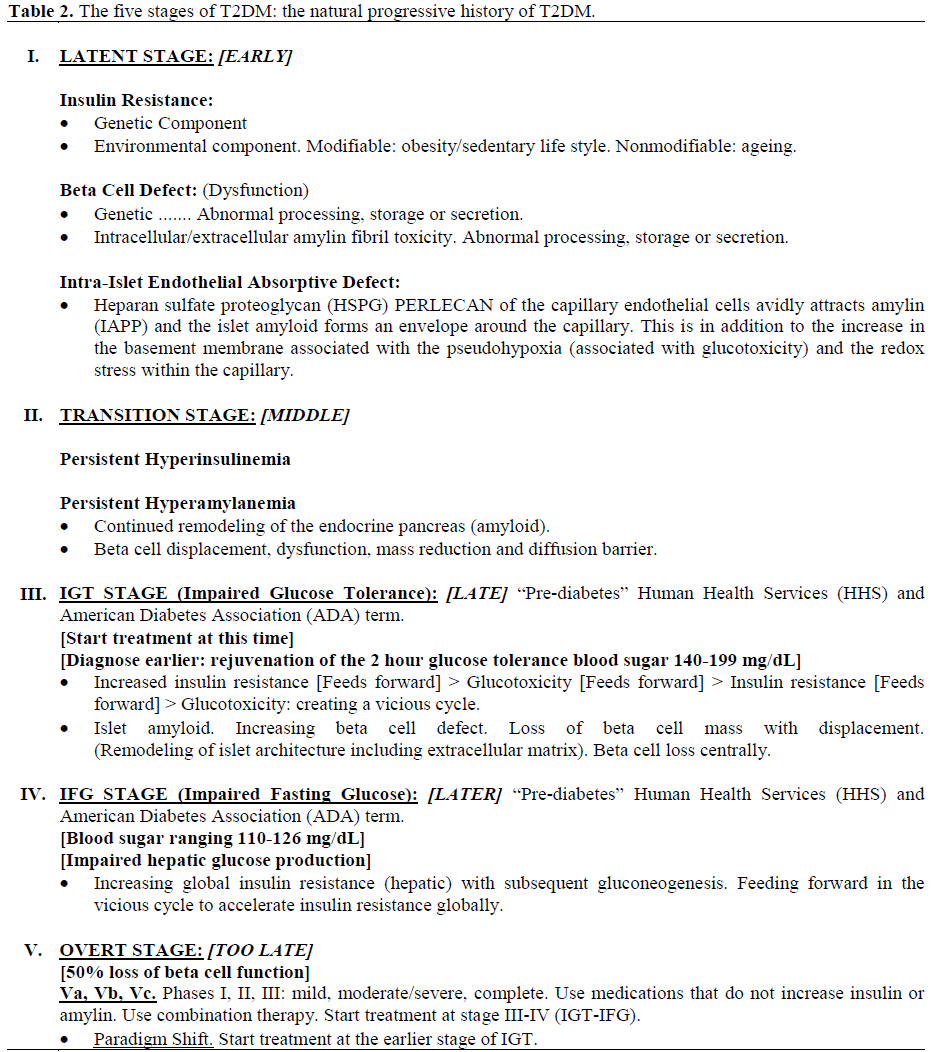
T2DM may be viewed as a continuum consisting of five stages: latent stage, transition stage, impaired glucose tolerance stage, impaired fasting glucose stage, and the overt stage with three subdivisions mild, moderate, and severe based on the degrees of abnormality of HbA1c and insulin levels reflecting the degree of beta cell dysfunction or failure i.e. mild, moderate, severe, and complete.
Unless there is an intervention, T2DM is characterized by a progressive nature and there is “a point of no return” wherein this devastating disease seems to progress regardless of the treatment provided as demonstrated in the United Kingdom Prospective Diabetes Study (UKPDS) [20]. For this very reason a change in the treatment paradigm should be considered and thus an emphasis will be placed on the “impaired glucose tolerance stage - Stage III”. Delaying treatment until there is chronic hyperglycemia places the patient at great risk for the development of not only overt T2DM but also the even more morbid devastating events associated with the development of an accelerated prediabetic and diabetic atherosclerosis (atheroscleropathy) and its inherent 2-4 fold increase in coronary artery disease and up to a 6 fold increase in congestive heart failure which is so costly in terms of morbidity, mortality, quality of life issues, and the financial burden to society. Two important quotes regarding the current situation (the double jeopardy of T2DM and atheroscleropathy) are relevant:
• The impact of cardiovascular disease on mortality and morbidity in people with diabetes has been known for years. Approximately two-thirds of people with diabetes die from cardiovascular disease (coronary heart disease, stroke, and other vascular diseases) [21];
• Diabetes must take its place alongside the other major risk factors as important causes of cardiovascular disease. In fact, from the point of view of cardiovascular medicine, it may be appropriate to say: "diabetes is a cardiovascular disease" [22].
T2DM and the metabolic syndrome have finally gained their proper respect in the 2001 National Cholesterol Educational Program Adult Treatment Panel III (NCEP ATP III) guidelines as T2DM is now considered a coronary risk equivalent and metabolic syndrome is included in the multiple risk factors for the development of atheroscleropathy and cardiovascular disease [23].
Stages in the Natural History of Type 2 Diabetes Mellitus
Stage I of the Continuum (The Latent Stage)
The latent stage may be identified by a strong clinical suspicion (Table 1) or the presence of at least one of the other markers of disease such as hypertension, coronary artery disease, dyslipidemia of the lipid triad (elevated VLDL cholesterol-triglycerides, decreased HDL cholesterol, elevated small dense atherogenic LDL cholesterol) associated with the metabolic syndrome. Histologically, amyloid is probably insignificant at this stage. The HbA1c is not elevated and glucose tolerance is normal with associated early elevations of insulin and amylin levels. A high level of clinical suspicion helps to identify this stage. Lifestyle changes are strongly encouraged both diet and exercise.
Stage II of the Continuum (The Silent Transition Stage)
The transition stage marks the beginning of structural changes within the islet with increasing amyloid aggregation and deposition. This results in a diffusion barrier (a space occupying lesion) and is the time when there is considerable damage to the beta cell due to the direct toxic effects of intermediate sized toxic amyloid particles (ISTAPs) [24]. Walsh et al. found that naturally secreted oligomers (similar to ISTAPs) of amyloid beta protein inhibited hippocampal long-term potentiation in vivo signifying that the oligomers or intermediate sized amyloid particles are toxic to cells similar to the findings of Janson et al. and Walsh et al. [24, 25]. These toxic effects result in apoptosis of the beta cells and for a certain period of time the more primordial ductal cells of the exocrine pancreas (replicative pool) can replace the damaged apoptotic beta cells and continue the compensatory hyperinsulinemia and hyperamylinemia [18] which cause further beta cell damage and contributes to the diffusion barrier. During this time there is development of a basement membrane absorptive defect. ADIA has a proclivity to bind to the heparan sulfate proteoglycan (perlecan) within basement membranes of intra islet capillaries. Thus, basement membranes surrounding islet capillaries are thickened and develop an absorptive barrier which aids in understanding the decreased first phase insulin secretory response through an absorptive defect.
The totality of beta cell function remains intact until there is approximately 50% damage or dysfunction of beta cells or disruption of absorptive capability. Histologically, amyloid would be in the 25- 50% stage (Figure 2). Insulin and amylin levels are increased and HbA1c and glucose tolerance would be normal. This stage is silent and represents a very active disease process without clinical signs or symptoms. The high index of clinical suspicion and associated clinical findings allow clinicians to be alerted to this stage similar to stage I. The time interval from suspecting stage I and II is important as time is not on the patients side unless there has been major changes in lifestyle in regards to diet and exercise.
Stage III of the Continuum (Prediabetes Stage): The Impaired Glucose Tolerance (IGT) Stage
The impaired glucose tolerance (IGT) stage is characterized by an abnormal response to a glucose challenge. The 75 gram oral glucose tolerance test is characterized by a normal fasting glucose with an abnormal 2-hour postprandial glucose in the range of 140-199 mg/dL. In March 2002 the Department of Health and Human Services (DHHS) and the American Diabetes Association (ADA) have provided a new term for this stage: “prediabetes”. The term IGT and impaired fasting glucose (IFG) may be termed “prediabetes”.
This stage represents a histological change within the islet of approximately 50-75% of ADIA involvement of islet architecture (Figure 2) or associated beta cell dysfunction.
Insulin and amylin levels are increased. Glucose tolerance is now abnormal with HbA1c remaining normal. This stage is extremely important as it is the stage wherein we can identify a large number of patients who will progress to overt stage V unless there is a significant intervention. At this time the clinician can obtain objective laboratory evidence that the transition stage is approaching “a point of no return”. It is known that 50% of patients with IGT will progress to overt (stage V) T2DM within ten years [26, 27, 28] unless there is aggressive intervention (“aggressive” life style changes in diet and exercise or institution of medication such as the insulin sensitizersthiazolidinediones, metformin or the alpha glucosidase inhibitors as these medications will improve non fasting and postprandial glucotoxicity without elevating endogenous insulin or amylin). If this stage is left unattended the natural history of T2DM is progressive. If the patient is non-compliant then this allows the clinician to instruct for careful follow up and monitoring of blood sugars both fasting and 2 hour post challenge. Additionally, Tuomilehto et al. recently found from the Diabetes Epidemiology Collaborative analysis Of Diagnostic criteria in Europe (DECODE) study that the two hour post glucose concentrations are better predictors of mortality than the fasting glucose alone [29].
Stage IV of the Continuum (Prediabetes Stage): The Impaired Fasting Glucose (IFG) Stage
The fasting glucose now becomes abnormal due to a progressive global insulin resistance with the amount of insulin remaining inadequate to compensate for increasing hepatic insulin resistance resulting in excess gluconeogenesis and free fatty acids within the liver resulting in elevations of the fasting glucose but not yet to a diagnostic range for overt diabetes [30]. This stage is associated with a fasting blood glucose of 110-125 mg/dL. Insulin resistance is more global and the insulin and amylin levels remain elevated. Histologically, amyloid would be in the 75% range (Figure 2). HbA1c levels would still be in the normal range and glucose tolerance would be abnormal.
Stage V of the Continuum (Overt T2DM Stage)
This stage is marked by either an abnormal fasting glucose equal to or greater than 126 mg/dL or a postprandial or random blood glucose equal to, or greater than, 200 mg/dL. The histological representation would be between 75-100% involvement of ADIA at this stage (Figure 2).
Stage Va: HbA1c ranging from 6.2 to 7.5%. Insulin resistance: moderate. Insulin levels increased or normal.
Stage Vb: HbA1c ranging from 7.6 to 10.0%. Insulin resistance: moderate/severe. Insulin levels decreasing.
Stage Vc: HbA1c greater than 10.0%. Insulin resistance: severe. Insulin levels markedly decreased to absent (Table 2, Figure 3) [30].
Stages Va, Vb, and Vc are comparable to phases I, II, and III in Lebovitz’s graph (Figure 3) [31, 32]. These stages are not meant to be rigid as the development of T2DM operates over a continuum and is capable of regression until the patient has reached a “point of no return”: beta cell failure. It is important to note that in the graph (Figure 3) there is a 50% reduction in beta cell function at the time of diagnosis of overt T2DM.
Figure 3. At the time of diagnosis of T2DM patients
already have a 50% reduction in beta cell function. As
one moves through the various stages-phases there is a
progressive loss of beta cell function while
concurrently there is increased deposition of amylin
derived islet amyloid. If treatment were started at an
earlier stage in the natural history of T2DM (Stage III:
impaired glucose tolerance or “prediabetes”) in a
manner to control elevated glucose levels without
elevating endogenous insulin or the monomeric
substrate amylin then it may be possible to halt the
progressive nature of T2DM. (Redrawn from Lebovitz
HE [31]).
The old saying that “time is on your side” does not hold true in the natural history of T2DM. In this disease and the associated macrovascular disease the “clock starts ticking” prior to the diagnosis of hyperglycemia and overt T2DM [33]. There is a period of time that may last 5-10 years wherein the metabolic syndrome may be in play, thus, accelerating micro/macrovascular disease and it is widely accepted that aging is a known risk factor for the development of both macrovascular disease and T2DM. At the time of diagnosis of T2DM at least one fourth (or greater) of patients may have developed macrovascular complications [34]. Furthermore, at the time of T2DM diagnosis more than 50% of patients have existing or pre-existing coronary heart disease. This means every other new patient will be affected with this specific macrovascular disease [35]. Global risk reduction is of utmost importance in the T2DM patients as they have a risk equivalent equal to those patients who have previously had a myocardial infarction. Therefore our goal should be secondary prevention in risk reduction (global risk reduction) for all patients with T2DM (Table 3) [35]. Mortality in T2DM is associated primarily with atheroscleropathy.
T2DM is now considered to be a cardiovascular risk equivalent and the National Cholesterol Education Program (NCEP) ATP III guidelines point to aggressive treatment as well as the sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VI guidelines) and the National High Blood Pressure Education Program (NHBPEP) [36]. Grant recently reported that hypercholesterolemia, and hypertension were not managed or screened-for as aggressively as hyperglycemia [37]. Additionally, McFarlane et al. [38] and Sowers and Reed [36] were able to show in urban academic centers that cardiovascular risk factors in patients with diabetes and hypertension obtained the following goals: HbA1c less than 7: 26.7%; blood pressure of 130/85 mmHg: 26.7%; LDL cholesterol of less than 100 mg/dL: 35.5%; antiplatelet therapy: 45.6%. Only 3.2% of patients met the combined ADA goal for blood pressure, LDL cholesterol, and HbA(1c).
Redox Stress and Amyloid Formation
There is a tremendous amount of redox stress - the process of generating un-paired electrons, reactive oxygen species (ROS), oxygen free radicals (toxic oxygen) by the process of reduction or oxidation - within the islets and the arterial vessel wall of the insulin resistant, metabolic syndrome, and T2DM patient [13, 14]. ROS contribute to and are a result of advanced glycosylation endproducts (AGE) formation. This glycation and glycoxidation process modifies proteins, lipids, and nucleic acids and results not only in damage to the islet and islet proteins but also greatly accelerates the process of atheroscleropathy within the arterial vessel wall. Redox stress is silent but results in a vulnerable islet prone to remodeling with the aggregation and polymerization of ADIA which adds to the progressive nature of this disease. Once ADIA has formed it is extremely resistant to the proteolytic enzymes within the extra cellular matrix. It seems paradoxical that ADIA deposition does not induce a chronic inflammatory response within the islet. Badman et al. and de Koning et al. were able to demonstrate that ADIA did not induce an inflammatory state within the islets and even though ADIA was internalized by macrophages it resisted proteolytic degradation [39, 40]. However, Opie in 1901 and 1910 was able to show a mononuclear inflammatory reaction in the exocrine portion of the pancreas with associated ADIA [1, 2]. It is important to place a quote by Badman et al. and de Koning et al. since we are discussing the progressive nature of T2DM: “Islet amyloidosis is progressive, apparently irreversible and is associated with destruction of insulin-secreting cells”.
Amyloid deposits (AL amyloid in multiple myeloma) have been shown to regress with the use of 123I-labeled serum amyloid P component scintigraphically when the disease state producing the monomeric unit is placed in remission so this provides a great hope for the future that the same will be true for ADIA in T2DM [41, 42].
There are multiple toxicities associated with insulin resistance, metabolic syndrome and T2DM. In an effort to categorize these toxicities the following mnemonic was created: A-FLIGHT toxicities [13, 14, 15]. Each of these toxicities are associated with the production of ROS and produce an unstable environment within the islet that can be compared to a violent lightning storm within the vulnerable islet. The damaging effects of unpaired electrons re-pairing creates a damaging effect to proteins, lipids, and nucleic acids. The ROS may cause an unfolding of the native secondary structure of amylin [13, 14]. Once this compact folded native amylin is unfolded it then becomes possible (due to the amyloidogenic nature of amino acids 20-29) for the beta pleated sheet conformation to realign into a newly formed secondary conformational antiparallel crossed beta pleated sheet structure: ADIA [13, 14]. These monomeric units undergo a prolific free radical polymerization due to the presence of ROS. Thus, ROS may not only contribute the unfolding of the native amylin structure allowing it to refold into antiparallel crossed beta pleated sheets but also allow for the rapid polymerization into mature islet amyloid. If we can decrease the substrates of the A-FLIGHT toxicities, and thus decrease the ROS, we may be able to have a positive effect on the progressive nature of amyloid formation and subsequently have a positive effect on the progressive natural history of T2DM [13, 14, 15].
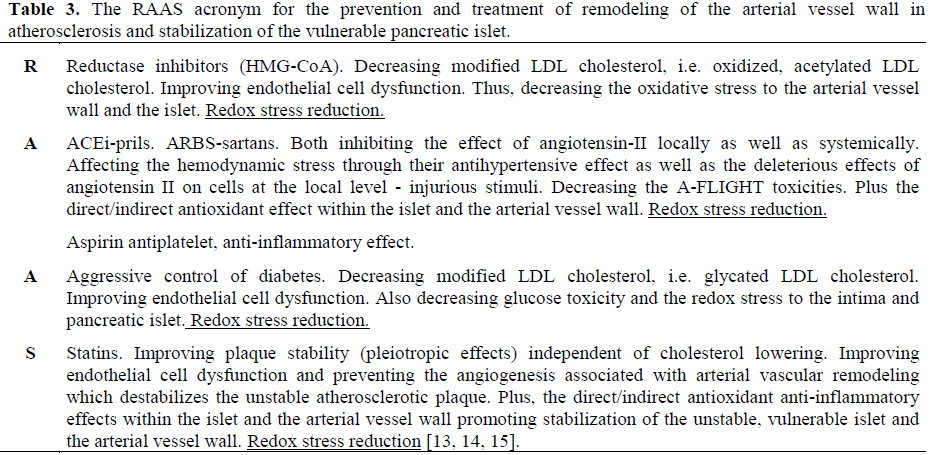
Currently, we have available newer medications (alpha glucosidase inhibitors, metformin, thiazolidinediones, the newer glinide analogs repaglinide and netaglinide, and soon the inhaled form of insulin ExuberaTM and the oral buccally absorbed insulin spray OralinTM) which will have a positive effect on each of these toxicities [43, 44, 45]. Specifically, we can decrease the glucotoxicity without elevating endogenous insulin or its fraternal twin: the amyloidogenic native substrate amylin. Also we can utilize the RAAS acronym (Table 3) to decrease the redox stress and the ROS produced by the A-FLIGHT toxicities of insulin resistance, metabolic syndrome, and T2DM [13, 14]. Recently, the angiotensin converting enzyme inhibitor ramipril (Heart Outcomes Prevention Evaluation, HOPE study), the 3 hydroxy-3methylglutarylcoenzyme A (HMGCoA) reductase inhibitor pravastatin (West of Scotland Coronary Prevention study, WOSCOPs), metformin (Diabetes Prevention Project, DPP), and the angiotensin II receptor antagonist (angiotensin receptor blocker: ARB) losartan (Losartan Intervention For Endpoint reduction in hypertension study, LIFE study) have been shown to reduce the relative risk of developing T2DM by 34%, 30%, 31%, and 25%, respectively (Table 3) [46, 47, 48, 49, 50, 51].
Conclusion
We should strongly consider rejuvenating the two-hour 75 gram oral glucose tolerance test (2hOGTT) which will allow clinicians to diagnose the impaired glucose tolerance stage III (blood sugars: 140-199 mg/dL) at an earlier stage in the natural history of T2DM. In order to identify those who will be more likely to progress to the stage V (overt T2DM; Table 2) we can utilize the 2hOGTT for stress testing those patients considered at high risk for development of stage V (overt T2DM; Table 1) just as we currently use the exercise and pharmacological stress testing for those suspected of having coronary heart disease.
For those who feel the inconvenience and cost of the 2-hour post glucose challenge are prohibitive a new “clinical model” was recently described by Stern et al. [52]. This clinical model which includes the clinical variables of age, sex, fasting glucose, body mass index, systolic blood pressure, HDLcholesterol, family history, and high risk ethnic background was used to compare results of predicting the probability of developing T2DM over a 7.5 year follow up study. So in the future we may be able to use this clinical model to calculate the probability of developing overt stage V T2DM from the clinical history and laboratory values we are accustomed to using similar to using the Framingham risk calculation in the NCEP ATP III guidelines. This model was shown to be of equal value and even superior to predicting the onset of T2DM when compared to the 75 gram 2hOGTT to determine impaired glucose tolerance. Aggressive changes in life style (weight reduction and exercise) as employed in the diabetes prevention program which revealed a 58% reduction in the development of overt T2DM are clearly recommended [49].
Consideration for intervening with drug therapy with newer medications to prevent or slow the development of glucotoxicity with its associated multiple complicating diabetic opathies. and being aggressive in treating patients to those HbA1c levels known to be protective (HbA1c of 7% or less). The American College of Endocrinology (ACE) consensus statement on guidelines for glycemic control white paper has recently recommended newer goals of HbA1c levels to 6.5% being careful to avoid hypoglycemia especially in the elderly [53].
Also, employ newer medications that lower glucose and HbA1c values without elevating endogenous insulin or amylin. By lowering the amyloidogenic substrate amylin (in addition to the other substrates of the AFLIGHT toxicities) we may be able to slow or prevent the progressive ADIA deposition within the islet and preserve beta cell function.
Be prepared to use these newer medications not only alone but also in combination therapy in order to achieve the desired HbA1c levels.
Consider using the medications in the RAAS acronym (Table 3) known to decrease the excess redox stress with a positive effect on the multiple A-FLIGHT toxicities associated with insulin resistance, metabolic syndrome, and overt T2DM [13, 14, 15].
By following this paradigm shift in the diagnosis, treatment, and prevention of the progressive nature of the natural history of T2DM we may be able to save the vulnerable islet, and prevent progressive ADIA deposition.
We are dealing with a disease of epidemic proportion in the United States and globally.
In the US there are 17 million people with diabetes and 90% (15.3 million) have T2DM. A review of four autopsy studies (two in the US, one in Germany, and one in Japan) revealed an average of 70% of T2DM patients have islet amyloid by light microscopy. This would correspond to an excess of 10 million patients with T2DM having positive amyloid staining (Congo red) with light microscopy.
Obviously, the presence of ADIA is huge and is felt to play a significant role in the remodeling of the endocrine pancreas as well as the natural progressive history of T2DM [13, 14, 15].
Translating a century old finding may allow us to not only better understand the progressive nature of T2DM but also have a greater opportunity to have a positive affect on the natural progressive history of this malicious, chronic debilitating disease.
This is especially important in light of the current exponential growth globally of T2DM not only in our aging population but also in our adolescent youth [54].
In summary, we can become enhanced “EDUCATORS” for our at risk T2DM patients.
1. Earlier Diagnosis. Earlier intervention with life style modifications and drug therapy.
2. Use of newer medications to decrease glucotoxicity without elevating endogenous insulin or the amyloidogenic amylin.
3. Combination therapy.
4. Aggressive Treatment to obtain the desired blood pressure, LDL-Cholesterol, and HbA1c levels known to be protective of the multiple complicating diabetic Opathies.
5. Use of those medication in the RAAS acronym to Reduce Redox stress.
6. Save, Stabilize, and preserve the beta cell and the vulnerable pancreatic islet.
Currently, we have available the technology and pharmacology to achieve these goals in order to have a positive effect on the horrendous cost (both quality of life issues and financial) to our society both at home and abroad.
Acknowledgement
In honor of the professors of Endocrinology University of Missouri, Columbia, Missouri, USA: TW Burns, DM Klachko, DW Gardner, and R James, for their devotion to teaching medical students and patients
References
- Opie EL. The relation of diabetes mellitus to lesions of the pancreas: hyaline degeneration of the islands of Langerhans. J Exp Med 1901; 5:527-54.
- Opie EL. Disease of the Pancreas: It’s Cause and Nature. 2nd ed. Philadelphia: JB Lippincott, 1910.
- Westermark P, Wernstedt C, O'Brien TD, Hayden DW, Johnson KH. Islet amyloid in type 2 human diabetes mellitus and adult diabetic cats contain a novel putative polypeptide hormone. Am J Pathol 1987; 127:414-7. [AN 87238835]
- Cooper GJ, Willis AC, Clark A, Turner RC, Sim RB, Reid KB. Purification and characterization of a peptide from amyloid-rich pancreas of type 2 diabetic patients. ProcNatlAcadSci USA 1987; 84:8628-32. [AN 88068642]
- Cooper GJ, Leighton B, Dimitriadis GD, Parry- Billings M, Kowalchuk JM, Howland K, et al. Amylin found in amyloid deposits in human type 2 diabetes mellitus may be a hormone that regulates glycogen metabolism in skeletal muscle. ProcNatlAcadSci USA 1988; 85:7763-6. [AN 89017278]
- Hoppener JW, Ahren B, Lips CJ. Islet amyloid and type 2 diabetes mellitus. New Eng J Med 2000; 343:411-9. [AN 20373846]
- Ludvik B, Kautzky-Willer, Prager R, Thomaseth K, Pacini G. Amylin: history and overview. Diabetes Medicine. 1997; 14(Suppl 2): S9-13.
- Ye JM, Lim-Fraser M, Cooney GJ, Cooper GJ, Iglesias MA, Watson DG, et al. Evidence that amylin stimulates lipolysis in vivo: a possible mediator of induced insulin resistance. Am J PhysiolEndocrinolMetab 2001; 280: E562-9. [AN 21155594]
- Kylin E. Studienueber das Hypertonie- Hyperglyka ”mie-Hyperurika” miesyndrom. Zentralblattfuer Innere Medizin 1923; 44:105-27.
- Himsworth H. Diabetes mellitus: a differentiation into insulin-sensitive and insulin-insensitive types. Lancet 1936; 1:127-30.
- Yalow RS, Glick SM, Roth J. Berson SA. Plasma insulin and growth hormone levels in obesity and diabetes. Ann NY AcadSci 1965; 131:357-73.
- Reaven GM. Banting Lecture 1988. Role of insulin resistance in human disease. Diabetes 1988; 37:1595-607. [AN 89052953]
- Hayden MR, Tyagi SC. Islet redox stress: the manifold toxicities of insulin resistance, metabolic syndrome and amylin derived islet amyloid in type 2 diabetes mellitus. JOP. J Pancreas (Online) 2002; 3:86- 108. [AN 22106694]
- Hayden MR, Tyagi SC. ‘A’ is for amylin and amyloid in type 2 diabetes mellitus. JOP. J Pancreas (Online) 2001; 2:124-39. [AN 21864435]
- Hayden MR, Tyagi SC. Remodeling of the endocrine pancreas: the central role of amylin and insulin resistance. South Med J 2000; 93:24-8. [AN 20116761]
- Alberti KGM, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med 1998; 15:539-53. [AN 98349482]
- Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults: findings from the third national health and nutrition examination survey. JAMA 2002; 287:356-9. [AN 21650872]
- Jones LC, Clark A. Beta cell neogenesis in type 2 diabetes mellitus. Diabetes 2001; 50(Suppl 1):S186-7. [AN 21088715]
- Guiot Y, Sempoux C, Moulin P, Rahier J. No decrease of the beta cell mass in type 2 patients. Diabetes 2001; 50(Suppl 1):S188. [AN 21088716]
- Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998; 352:837-53. [AN98413908]
- Clark CM Jr, Fradkin JE, Hiss RG, Lorenz RA,Vinicor F, Warren-Boulton E. The National Diabetes Education Program, changing the way diabetes is treated: comprehensive diabetes care. Diabetes Care 2001; 24:617-8. [AN 21212411]
- Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV, et al. Diabetes and cardiovascular disease: a statement for healthcare professionals from the American Heart Association. Circulation 1999; 100:1134-46. [AN 99406602]
- Brewer HB Jr. Rising to the challenge of the new NCEP ATP III guidelines: exceeding current therapeutic limitations. Am J Manag Care 2002; 8(Suppl 2):S23-8. [AN 21844481]
- Janson J, Soeller WC, Roche PC, Nelson RT, Torchia AJ, Kreutter DK, Butler PC. Spontaneous diabetes mellitus in transgenic mice expressing human islet amyloid polypeptide. ProcNatlAcadSci USA 1996; 93:7283-8. [AN 96293516]
- Walsh DM, Klyubin I, Fadeeva JV, Cullen WK, Anwyl R, Wolfe MS, et al. Naturally secreted oligomers of amyloid beta protein potently inhibit hippocampal long-term potentiation in vivo. Nature 2002; 416:535-9. [AN 21930460]
- Zimmet P, Alberti KG, Shaw J. Global and societal implications of the diabetes epidemic. Nature 2001; 414:782-7. [AN 21617700]
- Zimmet P. Globalization, coca-colonization and the chronic disease epidemic: can the Doomsday scenario be averted? J Intern Med 2000; 247:301-10. [AN 20225891]
- Shaw JE, Zimmet PZ, de Courten M, Dowse GK, Chitson P, Gareeboo H, et al. Impaired fasting glucose or impaired glucose tolerance. What best predicts future diabetes in Mauritius? Diabetes Care 1999; 22:399-402. [AN 99197990]
- Tuomilehto J, Qiao Q, Balkau B, Borch-Johnson K. Glucose tolerance and all-cause mortality. Cardiol Rev 2001; 18:241-53.
- Reasner CA, Defronzo RA. Treatment of type 2 diabetes mellitus: a rational approach based on its pathophysiology. Am Fam Physician 2001; 63:1687-9 4. [AN 21249623]
- Lebovitz HE. Insulin secretagogues: old and new. Diabetes Reviews 1999; 7:139-53.
- UK prospective diabetes study 16. Overview of 6 years? therapy of type II diabetes: a progressive disease. Diabetes 1995; 44:1249-58. [AN 96026173]
- Haffner SM, Stern MP, Hazuda HP, Mitchell BD, Patterson JK. Cardiovascular risk factors in confirmed prediabetic individuals. Does the clock for coronary heart disease start ticking before the onset of clinical diabetes? JAMA 1990; 263:2893-8. [AN 90250823]
- Dagogo-Jack S, Santiago JV. Pathophysiology of type 2 diabetes and modes of action of therapeutic interventions. Arch Intern Med 1997; 157:1802-16. [AN 97435872]
- Lenaers M. Cardiac complications of type 2 diabetes. Rev Med Brux 2000; 21:149-56. [AN 20381649]
- Sowers JR, Reed J. 1999 Clinical Advisory Treatment of Hypertension and Diabetes. J ClinHypertens (Greenwich) 2000; 2:132-3. [PMID 11416636]
- Grant RW, Cagliero E, Murphy-Sheehy P, Singer DE, Nathan DM, Meigs JB. Comparison of hyperglycemia, hypertension, and hypercholesterolemia management in patients with type 2 diabetes. Am J Med 2002; 112:603-9. [AN 22030031]
- McFarlane SI, Jacober SJ, Winer N, Kaur J, Castro JP, Wui MA, et al. Control of cardiovascular risk factors in patients with diabetes and hypertension at urban academic medical centers. Diabetes Care 2002; 25:718-3. [AN 21916838]
- Badman MK, Pryce RA, Charge SB, Morris JF, Clark A. Fibrillar islet amyloid polypeptide (amylin) is internalised by macrophages but resists proteolytic degradation. Cell Tissue Res 1998; 291:285-94. [AN 98089101]
- deKoning EJ, van den Brand JJ, Mott VL, Charge SB, Hansen BC, Bodkin NL, et al. Macrophages and pancreatic islet amyloidosis. Amyloid 1998; 5:247-54. [AN 99155607]
- Hawkins PN, Richardson S, MacSweeney JE, King AD, Vigushin DM, Lavender JP, Pepys MB. Scintigraphic quantification and serial monitoring of human visceral amyloid deposits provide evidence for turnover and regression. Q J Med 1993; 86:365-74. [AN 94225044]
- Hawkins PN. Diagnosis and monitoring of amyloidosis. BaillieresClinRheumatol 1994; 8:635- 59. [AN 95042805]
- Gerber RA, Cappelleri JC, Kourides IA, Gelfand RA. Treatment satisfaction with inhaled insulin in patients with type 1 diabetes: a randomized controlled trial. Diabetes Care 2001; 24:1556-9. [AN 21413641]
- Pankaj M, Marko M. Replacement of s.c. injections with Oralin in treatment of diabetes. Abstract #179-OR. Philadelphia: Pennsylvania, American Diabetes Association: June 25th, 2001.
- Modi P, Mihic M, Lewin A. The evolving role of oral insulin in the treatment of diabetes using a novel RapidMist(trade mark) System. Diabetes Metab Res Rev 2002; 18(Suppl 1):S38-42. [AN 21916874]
- Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus: results of the HOPE study and MICROHOPE substudy. Heart Outcomes Prevention Evaluation Study Investigators. Lancet 2000; 355:253- 9. [AN 20137536]
- Webster MW. The HOPE study and diabetes. Heart Outcomes Prevention Evaluation. Lancet 2000; 355:1181-2. [AN 20250037]
- Freeman DJ, Norrie J, Sattar N, Neely RD, Cobbe SM, Ford I, et al. Pravastatin and the development of diabetes mellitus: evidence for a protective treatment effect in the West of Scotland Coronary Prevention Study. Circulation 2001; 103:357-62. [AN 21112837]
- Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002; 346:393-403. [AN 21822558]
- Dahlof B, Devereux RB, Kjeldsen SE, Julius S, Beevers G, Faire U, et al. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomized trial against atenolol. Lancet. 2002; 359:995-1003. [AN 21935633]
- Lindholm LH, Ibsen H, Dahlof B, Devereux RB, Beevers G, de Faire U, et al. Cardiovascular morbidity and mortality in patients with diabetes in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet 2002; 359:1004-10. [AN 21935634]
- Stern MP, Williams K, Haffner SM. Identification of persons at high risk for type 2 diabetes mellitus: do we need the oral glucose tolerance test? Ann Intern Med 2002; 136:575-81. [AN 21952277]
- American College of Endocrinology Consensus Statement on Guidelines for Glycemic Control. ACE Guidelines for Glycemic Control. EndocrPract 2002; 8(Suppl 1):5-11.
- Pinhas-Hamiel O, Standford D, Daniels SR. A persistent increase of noninsulin-dependent diabetes mellitus (NIDDM) among adolescents. Int J Obes 1998; 206(Suppl 3):414.




