Keywords
Abdominal Pain; Diabetes Mellitus; Insulin; Pancreatitis, Chronic; Quality of Life
Funding
This work was supported by NIH DK096327 (AU); DK097820 (AU).
Disclosures
Consultant, Abbvie Inc. for exocrine pancreatic function testing (AU). No conflicts: HA, RR.
Abbreviations
CFTR cystic fibrosis transmembrane conductance regulator; CP chronic pancreatitis; CTRC chymotrypsin C; CPA1 carboxypeptidase-1; CLDN2 claudin 2; CEL carboxylesterlipase; PNLIP pancreatic triglyceride lipase; ERCP endoscopic retrograde pancreatography; INSPPIRE INternational Study Group of Pediatric Pancreatitis: In search for a cuRE; PRSS1 protease, serine 1; SPINK1 serine protease inhibitor Kazal-type 1; TP/IAT total pancreatectomy with islet autotransplantion; IEQ islet equivalent; PERT Pancreatic enzyme replacement therapy; QOL quality of life; EPI exocrine pancreatic insufficiency
Introduction
Chronic pancreatitis (CP) is a progressive inflammatory process of the pancreas that results in irreversible structural changes, loss of parenchyma and fibrosis, leading to exocrine pancreatic insufficiency (EPI) and diabetes [1]. Children with acute recurrent or chronic pancreatitis often have mutations in the cationic trypsinogen (PRSS1), cystic fibrosis transmembrane generator (CFTR), serine protease inhibitor Kazal type I (SPINK1) and carboxypeptidase 1 (CPA1) genes [2-8]. A strong association between CPA1 mutations and childhood-onset CP [8] suggests that genetic risk factors may determine early onset of CP. The genetic variants in the claudin 2 (CLDN2) [9], and chymotrypsin C (CTRC) genes [10], carboxylesterlipase (CEL) and CELHYB allele (originating from a crossover between CEL and its neighboring pseudogene, CELP) [11, 12] increase the risk for CP in adults with idiopathic CP or already have alcohol and smoking as risk factors. Most high-penetrance PRSS1 variants increase intrapancreatic trypsin activity by stimulating trypsinogen autoactivation and/or by inhibiting CTRC-dependent trypsinogen degradation [13]. Alternatively, some gene mutations (PRSS1 variants, CELHYB, pancreatic triglyceride lipase (PNLIP), CPA1) can cause protein misfolding, which results in intracellular retention/degradation and consequent endoplasmic reticulum stress [8, 11, 13, 14].
The persistent abdominal pain, exocrine pancreatic insufficiency (EPI), diabetes, repeated hospitalizations and procedures, result in overall impaired quality of life (QOL) in children with CP [15-17]. The recurrent exacerbations and unrelenting pain may lead to depression and narcotic analgesic dependence. Patients with hereditary pancreatitis have a high life time risk of EPI, diabetes and pancreatic adenocarcinoma (up to 40%) [18-20]. The diabetes occurs in ~5% of patients with hereditary pancreatitis by 10 years after the onset of symptoms, and 18% by 20 years [18]. This form of diabetes is called type 3c or pancreatogenic diabetes and is the result of partial or complete loss of insulin secretion. The treatment of pediatric CP should be directed at the complications, including chronic pain, EPI and diabetes. This review focuses on total pancreatectomy with islet cell autotransplantation (TP/IAT) as a therapeutic alternative for pediatric CP.
TOTAL PANCREATECTOMY WITH ISLET AUTOTRANSPLANTATION (TP/IAT)
Although TP/IAT is being performed in increasing numbers in children, the literature is limited to publications from a few single centers. In general, the studies are retrospective, study populations are small, and the duration of follow-up is relatively short. The self-reported or guardian-reported measures (telephone surveys, mailed HbA1c kits, selfrecorded glucose levels) may introduce bias.
Total pancreatectomy (TP) is an irreversible operation and often reserved for diffuse pancreatic disease. It involves complete resection of the pancreas on the basis that removing the diseased organ would eliminate the pain. TP removes any cancer risk that those patients may harbor [18-20], but leaves patients deprived of the exocrine and endocrine functions of the pancreas. Whereas it may be relatively simple to substitute the exocrine function of the pancreas with pancreatic enzyme replacement therapy (PERT), replacing the endocrine function is more problematic. Some patients who undergo TP may develop brittle diabetes associated with hypoglycemia and hyperglycemia [21-34], which is particularly difficult to control.
The islet autotransplantation is designed to preserve the beta cell mass in patients undergoing TP. Islet autotransplantation after pancreatectomy was first performed for CP in 1977 [35] with the first pediatric application in 1989 [36]. Unlike the islet cell allotransplants, there is no need for immunosuppression post-operatively since the transplantation is autologous.
Technical Considerations
The largest series have been reported from the University of Minnesota, University of Cincinnati, Medical University of South Carolina and Leicester General Hospital [21, 23- 28, 30-34, 36-44]. The procedure is most often performed by open laparotomy, but there have been few studies using robotic assistance [40]. The first part of the procedure consists of total pancreatic resection, removing second portion of the duodenum, distal common bile duct, and often the spleen, appendix and gallbladder [24, 32, 34]. The bowel continuity is restored with duodenoduodenostomy or duodenojejunostomy and bile continuity with choledochoduodenostomy or chledochojejunostomy. The removed pancreatic tissue is sent for islet cell harvest.
The success of islet isolation depends on an efficient delivery of collagenase enzymes for pancreatic digestion and removal of acinar and ductal tissue. It is challenging to obtain high quality islet yields from fibrotic, calcified tissues of CP. Optimizing perfusion of the collagenases by clamping pancreatic duct leaks may increase the number of isolated islets [45]. Some suggest adjusting the dose of collagenase enzymes for patient’s age and amount of pancreatic fibrosis [46]. A new enzyme mixture consisting of collagenase and neutral proteases has also been proposed to optimize the islet yield [47, 48]. The pancreatic homogenates are then subjected to density gradient purification to purify islets and remove the unwanted exocrine tissue and digestive enzymes [49].
One purified, islets are counted and assessed for viability. The islet yield is quantified in terms of islet equivalents (IEQ), which is the islet mass standardized to an islet size of 150 μm. Obtaining high quantity and excellent quality islets from CP remains a challenge and further refinement of the procedures is required.
After a lengthy isolation and possibly purification process, islets are infused into the hepatic circulation via the portal vein. The islet autotransplantation is currently performed at over 15 academic institutions in the US [50]. The procedure requires unique technical expertise and adherence to strict Food and Drug Administration (FDA) standards for Good Manufacturing Practice involving processed tissue samples.
The animal models have suggested that early hyperglycemia results in impaired revascularization, islet apoptosis, and a substantial reduction in islet mass following transplantation [51-53]. Hence, the patients receive insulin post-operatively, often for three months, to maintain euglycemia and allow the islets the opportunity to engraft and vascularize without functional stress. Insulin is later weaned while keeping satisfactory glucose and HbA1c levels (fasting blood sugar <126 mg/dL, postprandial blood sugar <180 mg/dL, and HbA1c≤6.5%). Other considerations include administering pre-splenectomy vaccinations, initiating PERT, fat-soluble vitamins, and adequate pain control before the procedure.
The portal venous pressure may increase transiently with islet infusion [39, 41]. Although 3-4 % risk of partial portal venous thrombosis can be observed [54], no serious sequelae have been reported in children. If the portal venous pressure becomes persistently high during IAT, the remaining islet cells are often infused into the peritoneal cavity or injected into the mesentery, omentum, bowel subserosa, gastric submucosa or intramuscular space [21, 23]. Although islets transplanted at these alternative sites have been shown to survive in animal models [55], there are no clinical studies comparing islet function and survival between liver vs. other locations. Bellin et al. have shown more physiological glucagon responses to hypoglycemia in patients who received both hepatic and non-hepatic islet transplantation compared to hepatic infusion alone [66]. It is encouraging that the intramuscular islet autotransplantation in a 7-year-old child with hereditary pancreatitis resulted in low insulin requirements and C-peptide positivity for more than 2 years [56]. More studies are needed to establish the best location for islet engraftment and functioning.
Almost half of the islets may be lost during the infusion due to a non-specific inflammatory and thrombotic reaction called instant blood-mediated inflammatory reaction (IBMIR) [57]. IBMIR is characterized by platelet consumption and activation of the coagulation and complement systems. Techniques that minimize IBMR (i.e. culturing islets with low molecular weight dextran sulfate) will diminish the early loss of islets [57]. More studies are needed to define the factors that affect islet cell survival after transplantation.
Indications
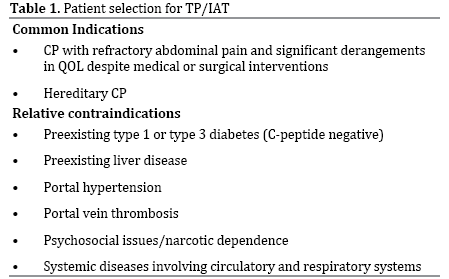
Currently, there are no consensus guidelines for TPIAT eligibility, but parameters that have been developed by individual centers (summarized in Table 1). In general, the children with intractable abdominal pain due to CP who failed other therapies are candidates for this operation. There may be a lower threshold to select patients with PRSS1 mutations because of the risk for pancreatic cancer in the future. The decision for TPIAT requires a multidisciplinary team including pediatric gastroenterologists, pediatric surgeons, pediatric endocrinologists, psychologists, and anesthesiologists. The child’s physical and emotional status in coping with and managing diabetes must be assessed.
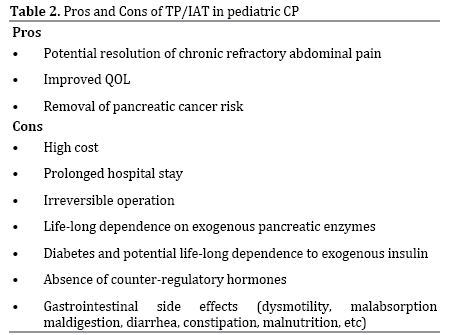
In a rare child who presents with CP and diabetes, TP/IAT may still be considered if the diabetes is mild (C-peptide positive) and there is no evidence of autoimmune diabetes (negative islet autoantibodies) to avoid the development of brittle diabetes in the future [23, 30, 45]. C-peptide values from mixed meal tolerance testing may be useful in predicting the islet cell yield in these children [23, 30]. Intravenous arginine stimulation testing may assess the number of engrafted islets post-transplant [58]. Pros and cons of TP/IAT in children with CP are summarized in Table 2.
Outcome
The most important measure of success after TP/IAT is pain relief while preserving the pancreatic endocrine function. Other endpoints include narcotic independence, QOL, post-operative complications and survival. Below is the summary of outcomes reported in pediatric patients after TP/IAT.
Pain Control
All patients receive IV opioids immediately after surgery that is later changed to oral analgesics. According to studies from the University of Minnesota, the pain improves gradually in children who undergo TP/IAT. Most of this improvement takes place within the first year, with 50-80% of patients becoming narcotic independent on follow-up [21, 26, 29, 32, 33, 43]. The pain improvement is largely sustained at 10-year follow-up, whereby 10-20% of patients continue to take narcotics [32, 33]. In general, the preadolescent children have better responses compared to adolescents (89% achieve narcotic independence vs. 33%) [21, 25]. Chronic narcotic use can result in opioid-induced hyperalgesia and make the postoperative weaning of pain medications challenging [59].
Pancreatic Endocrine Function
In general, higher islet yields are associated with better graft function and a higher likelihood of insulin independence [37, 41]. Patients are more likely to achieve insulin independence if islet yield is over 5,000 IEQ/kg body weight or a total of 100,000 IEQ [29, 32, 33, 45].
The islet yield is strongly influenced by the histopathological changes in the pancreas [25, 33, 41, 60]. IEQ per body weight is significantly lower in the presence of advanced pancreatic fibrosis, acinar atrophy and hereditary/genetic pancreatitis. There is no correlation between the islet yield and the type, degree, location of inflammation, distribution or location of fibrosis or acinar atrophy [25]. Islet yield may be predicted by fasting blood glucose, HbA1c and C-peptide levels prior to surgery [23].
A history of previous pancreatic surgery is inversely correlated with insulin independence, with distal pancreatectomies and drainage procedures (i.e. Puestow procedure) being strongly associated with worse outcomes at the University of Minnesota [24, 26, 33, 52]. This is explained by the fact that partial pancreatectomies remove as much as half to two thirds of the pancreas and thus the islets, whereas drainage procedures dissect the pancreatic duct which could compromise the intraductal perfusion of enzymes during islet isolation [21, 24]. Severe fibrosis and acinar atrophy were found in the pancreas of patients who underwent a prior drainage operation, but it is not knownwhether this is directly related to the intervention itself or indirectly through delaying TP/IAT while CP progressed [25]. There was no difference in islet yield of children with previous pancreatic surgeries vs. those who did not at the University of Cincinnati [43], but the numbers were small. Autotransplanted islets do not resume full function immediately after surgery. They depend on the diffusion of oxygen and nutrients until neovascularization occurs in 2-4 weeks [61, 62].
The blood glucose is closely monitored during and after surgery and strictly controlled with insulin to avoid possible detrimental effect of hyperglycemia on islet engraftment. In general, the islet cell function after TP/ IAT is assessed indirectly by the need for insulin. However, insulin replacement does not substitute for all hormones of the pancreatic islets, including glucagon, somatostatin and pancreatic polypeptide.
In general, children undergoing TPIAT achieve higher rates of insulin independence (~50%) compared to adults (~30%) [21, 32, 43]. It is not known whether the superior response in pediatric patients is due to the extent of pancreatic disease or regenerative capacity of the islets. This could be the result of fewer pancreatic procedures performed on younger patients or shorter course of disease. Younger children (<12 years) are more likely to achieve insulin independence compared to older children [33]. However, it is unknown why the adolescents with shorter disease duration experience less favorable results compared to preadolescents. Poor engraftment, increased loss of islets, decreased islet function may be some of the factors leading to the unfavorable outcome in adolescents [21]. The prepubertal milieu may also be more protective of transplanted islets than that of puberty when insulin resistance is more prominent [25]. Based on the unfavorable results in adolescents compared to prepubertal children, early TP/IAT has been increasingly recommended.
The islet function persists in adults who undergo TPIAT, but the percentage of patients that remain insulinindependent declines over time [29, 38, 42, 60]. The decline is faster in patients with hereditary/genetic pancreatitis [33]. Similar to the narcotic independence, insulin independence is also generally sustained over the 10-year follow-up in the majority of children (~40%) [32]. It appears that transplanted islets are able to uphold their function despite patients’ growth and development. It is unclear how islet cells compensate for the child’s growth, and whether this is due to islet cell replication or neogenesis. Some reports have even raised the question of islet quality versus quantity [21]. The viability or function of the islets may deteriorate over time due to formation of beta cell autoantibodies [63] or amyloid deposition in islets [64]. To date, amyloid deposition has only been reported in islet allografts.
Quality of Life (QOL)
Chronic, relenting pain is common in children with CP. In a multicenter study led by INSPPIRE, ~80% of children with CP reported abdominal pain and the pain was constant requiring narcotic use in ~1/3rd [17]. Chronic pain is linked to anxiety, depression, low self-esteem, and overall decreased QOL. Children with CP and chronic pain experience frequent school absences, decreased social functioning and high level of fatigue [43, 65]. Chronic pain is the leading indication for medical, endoscopic and surgical interventions including TP/IAT.
Both children and adults demonstrate significant improvement in physical and mental health after TP/IAT [26, 33, 43, 66]. The QOL is reported as good to excellent in ~75% of children following TP/IAT, with a slight drop in QOL physical and mental measures ~ 6 months postoperatively that coincides with weaning from narcotics at that time [21]. Two years after surgery, less than 10% of parents report lost school days compared to 87% before surgery. Limited activity days also significantly diminishes by 2 years after surgery [32]. The improvement in QOL is not as remarkable in adults [26].
Gastrointestinal Side Effects
The gastrointestinal symptoms are common complaints for patients with CP both before and after TP/IAT [31, 50]. Diarrhea is the most common complaint with a peak incidence at 6 months after surgery. Steatorrhea is also more prevalent at 6 months and 1 year post-surgically. Constipation is not commonly seen, possibly as a result of discontinuing narcotic therapy. Gastroparesis is common after TP/IAT as the enteric and biliary reconstruction may significantly alter gut motility [67]. The loss of exocrine pancreatic function after TP/IAT inevitably causes maldigestion and malabsorption of nutrients, which in turn impacts the glycemic control [68]. Children also experience weight loss post-operatively, therefore adequate PERT and fat-soluble vitamin replacement is vital in the care of these patients. PERT improves steatorrhea to some degree, but does not seem to have an impact on other GI symptoms. The challenges with PERT include cost, optimal dosing and compliance.
Pancreatic Cancer
TP removes the pancreas, therefore the risk for pancreatic adenocarcinoma associated with CP [18-20]. Very small amounts of acinar and ductal cells may be co-infused into the liver with the islet cell product [69]. However, there are no reports of pancreatic cancer after TP/IAT.
Morbidity and Mortality
Intraoperative complications may include: hypotension (15% patients requiring vasopressors), blood loss (350- 1200 ml), hypothermia (39%) [39]. The post-operative care of the TP/IAT patient requires a dedicated team and close follow-up. In general, children are hospitalized an average of 16-24 days after surgery [21, 25, 43]. The immediate post-operative mortality is low (<2%) and in one case due to enteric perforation from a feeding tube, peritonitis and sepsis [29, 32]. In the largest series to date, the complications occurred in 20 children who underwent TP/IAT (20%), with urinary tract infections (17%), catheter related bacteremias (12.5%), and pneumonia (12.5%) being the most common. Overall, younger children (<12 years) tended to have lower complication rates compared to older children. Prior pancreatic surgery did not seem to affect post-operative complication rates [32] Other post-operative complications are: intraabdominal hematomas/abscesses, splenic tear/bleeding, bile leak, pancreaticocutaneous fistula, gastrointestinal bleeding, median nerve injury, aspiration pneumonia (each <5%) [39].
The long-term survival after surgery is ~90% at five years, 81% at 10 years, and 62% at 20 years in both adults and children [29, 33]. The long-term mortality in most instances is unrelated to the surgery [60].
CONCLUSION
As mentioned earlier, the literature on TP/IAT in children is limited to few single center experiences. The operation is likely to be successful in a group of children with CP, but the long-term consequences of this operation are largely unknown. Therefore, the selection process should be handled with utmost care. Despite the increased use of TP/IAT for pediatric CP, especially within the last decade, many questions remain unanswered. The patient selection and timing of the procedure are the main quandaries. The limitation in the accurate diagnosis of CP is another important confounding factor.
The natural history of CP and the factors that predispose to rapid progression of disease (severe pancreatic fibrosis, EPI and diabetes) are not well-known in the pediatric age group. A better understanding of the natural history of CP in children may lead to the development of therapies that interrupt disease progression. It may also help identify the best timing to intervene.
The research priorities should focus on devising guidelines for diagnosing early CP, determining patients who would benefit from TP/IAT and identifying best timing for this operation if necessary [50]. Predicting the islet yields is a key factor in decision-making and pancreatic histological changes seem to correlate with the islet yield and insulin independence. Thus, the development of non-invasive or minimally invasive methods to assess pancreatic fibrosis is crucial to achieve this goal. Optimizing methods for islet isolation and improving islet engraftment, viability and longevity are other targets for future research. Improving QOL and returning to daily activities should be the benchmark of success following treatment.
Conflicting Interest
The authors had no conflicts of interest
References
- Morinville VD, Lowe ME, Ahuja M, Barth B, Bellin MD, Davis H, et al.: Design and implementation of insppire (international study group of pediatric pancreatitis: In search for a cure). J Pediatr Gastroenterol Nutr 2014;59:360-4. [PMID: 24824361]
- Schnur A, Beer S, Witt H, Hegyi P, Sahin-Toth M: Functional effects of 13 rare prss1 variants presumed to cause chronic pancreatitis. Gut 2014; 63: 337-343. [PMID: 23455445]
- Lucidi V, Alghisi F, Dall'Oglio L, D'Apice MR, Monti L, De Angelis P et al. The etiology of acute recurrent pancreatitis in children: A challenge for pediatricians. Pancreas 2011; 40:517-521. [PMID: 21499205]
- Sobczynska-Tomaszewska A, Bak D, Oralewska B, Oracz G, Norek A, Czerska K et al. Analysis of cftr, spink1, prss1 and aat mutations in children with acute or chronic pancreatitis. J Pediatr Gastroenterol Nutr 2006; 43:299-306. [PMID: 16954950]
- Van Geenen EJ, Smits MM, Schreuder TC, van der Peet DL, Bloemena E, Mulder CJ: Smoking is related to pancreatic fibrosis in humans. Am J Gastroenterol 2011; 106:1161-1166; quiz 1167. [PMID: 21577244]
- Sanchez-Ramirez CA, Larrosa-Haro A, Flores-Martinez S, Sanchez-Corona J, Villa-Gomez A, Macias-Rosales R: Acute and recurrent pancreatitis in children: Etiological factors. Acta Paediatr 2007; 96:534-537. [PMID: 17306005]
- Witt H: Gene mutations in children with chronic pancreatitis. Pancreatology 2001; 1:432-438. [PMID: 12120220]
- Witt H, Beer S, Rosendahl J, Chen JM, Chandak GR, Masamune A, et al. Variants in cpa1 are strongly associated with early onset chronic pancreatitis. Nat Genet 2013; 45:1216-1220. [PMID: 23955596]
- Derikx MH, Kovacs P, Scholz M, Masson E, Chen JM, Ruffert C, et al. Polymorphisms at prss1-prss2 and cldn2-morc4 loci associate with alcoholic and non-alcoholic chronic pancreatitis in a european replication study. Gut 2014. [PMID: 25253127]
- LaRusch J, Lozano-Leon A, Stello K, Moore A, Muddana V, O'Connell M, et al. The common chymotrypsinogen c (ctrc) variant g60g (c.180t) increases risk of chronic pancreatitis but not recurrent acute pancreatitis in a north american population. Clinical and translational gastroenterology 2015; 6:e68. [PMID: 25569187]
- Fjeld K, Weiss FU, Lasher D, Rosendahl J, Chen JM, Johansson BB, et al. A recombined allele of the lipase gene cel and its pseudogenecelp confers susceptibility to chronic pancreatitis. Nat Genet 2015. [PMID: 25774637]
- Ragvin A, Fjeld K, Weiss FU, Torsvik J, Aghdassi A, Mayerle J, et al. The number of tandem repeats in the carboxyl-ester lipase (cel) gene as a risk factor in alcoholic and idiopathic chronic pancreatitis. Pancreatology 2013; 13:29-32. [PMID: 23395566]
- Nemeth BC, Sahin-Toth M: Human cationic trypsinogen (prss1) variants and chronic pancreatitis. Am J Physiol Gastrointest Liver Physiol 2014; 306: G466-473. [PMCID: 2793115]
- Szabo A, Xiao X, Haughney M, Spector A, Sahin-Toth M, Lowe ME. A novel mutation in pnlip causes pancreatic triglyceride lipase deficiency through protein misfolding. Biochim Biophys Acta 2015; 1852:1372-1379. [PMID: 25862608]
- Bellin MD, Freeman ML, Schwarzenberg SJ, Dunn TB, Beilman GJ, Vickers SM,et al. Quality of life improves for pediatric patients after total pancreatectomy and islet autotransplant for chronic pancreatitis. Clin Gastroenterol Hepatol 2011; 9:793-799. [PMCID: 3163759]
- Pohl JF, Limbers CA, Kay M, Harman A, Rollins M, Varni JW: Health-related quality of life in pediatric patients with long-standing pancreatitis. J Pediatr Gastroenterol Nutr 2012; 54:657-663. [PMID: 22094900]
- Schwarzenberg SJ, Bellin M, Husain SZ, Ahuja M, Barth B, Davis H et al.: Pediatric chronic pancreatitis is associated with genetic risk factors and substantial disease burden. J Pediatr 2014. [PMID: 25556020]
- Howes N, Lerch MM, Greenhalf W, Stocken DD, Ellis I, Simon P, et al. Clinical and genetic characteristics of hereditary pancreatitis in europe. Clin Gastroenterol Hepatol 2004; 2:252-261. [PMID: 15017610]
- Vitone LJ, Greenhalf W, Howes NR, Neoptolemos JP: Hereditary pancreatitis and secondary screening for early pancreatic cancer. Rocz Akad Med Bialymst 2005; 50:73-84. [PMID: 16358943]
- Howes N, Neoptolemos JP.Risk of pancreatic ductal adenocarcinoma in chronic pancreatitis. Gut 2002; 51:765-766. [PMCID: 1773485]
- Bellin MD, Carlson AM, Kobayashi T, Gruessner AC, Hering BJ, Moran A, et al. Outcome after pancreatectomy and islet autotransplantation in a pediatric population. J Pediatr Gastroenterol Nutr 2008; 47:37-44. [PMID: 18607267]
- Sutherland DE, Gruessner AC, Carlson AM, Blondet JJ, Balamurugan AN, Reigstad KF, et al. Islet autotransplant outcomes after total pancreatectomy: A contrast to islet allograft outcomes. Transplantation 2008; 86:1799-1802. [PMID: 19104425]
- Bellin MD, Blondet JJ, Beilman GJ, Dunn TB, Balamurugan AN, Thomas W, et al. Predicting islet yield in pediatric patients undergoing pancreatectomy and autoislet transplantation for chronic pancreatitis. Pediatr Diabetes 2010; 11:227-234. [PMID: 19708905]
- Bellin MD, Sutherland DE: Pediatric islet autotransplantation: Indication, technique, and outcome. Curr Diab Rep 2010; 10:326-331. [PMID: 20680524]
- Kobayashi T, Manivel JC, Bellin MD, Carlson AM, Moran A, Freeman ML, et al. Correlation of pancreatic histopathologic findings and islet yield in children with chronic pancreatitis undergoing total pancreatectomy and islet autotransplantation. Pancreas 2010; 39:57-63. [PMID: 19745778]
- Bellin MD, Freeman ML, Schwarzenberg SJ, Dunn TB, Beilman GJ, Vickers SM,et al. Quality of life improves for pediatric patients after total pancreatectomy and islet autotransplant for chronic pancreatitis. Clin Gastroenterol Hepatol 2011; 9:793-799. [PMCID: 3163759]
- Kobayashi T, Manivel JC, Carlson AM, Bellin MD, Moran A, Freeman ML, et al. Correlation of histopathology, islet yield, and islet graft function after islet autotransplantation in chronic pancreatitis. Pancreas 2011; 40:193-199. [PMID: 21404456]
- Bellin MD, DE RS, Robertson RP.Pancreatectomy and autologous islet transplantation for painful chronic pancreatitis: Indications and outcomes. Hosp Pract (1995) 2012; 40:80-87. [PMID: 23086097]
- Sutherland DE, Radosevich DM, Bellin MD, Hering BJ, Beilman GJ, Dunn TB, et al. Total pancreatectomy and islet autotransplantation for chronic pancreatitis. J Am Coll Surg 2012; 214:409-424. [PMID: 22397977]
- Bellin MD, Beilman GJ, Dunn TB, Pruett TL, Chinnakotla S, Wilhelm JJ, et al. Islet autotransplantation to preserve beta cell mass in selected patients with chronic pancreatitis and diabetes mellitus undergoing total pancreatectomy. Pancreas 2013; 42:317-321. [PMID: 23146918]
- Bellin MD, Freeman ML, Gelrud A, Slivka A, Clavel A, Humar A, et al. Total pancreatectomy and islet autotransplantation in chronic pancreatitis: Recommendations from pancreasfest. Pancreatology 2014; 14:27-35. [PMID: 24555976]
- Chinnakotla S, Bellin MD, Schwarzenberg SJ, Radosevich DM, Cook M, Dunn TB, et al. Total pancreatectomy and islet autotransplantation in children for chronic pancreatitis: Indication, surgical techniques, postoperative management, and long-term outcomes. Ann Surg 2014; 260:56-64. [PMID: 24509206]
- Chinnakotla S, Radosevich DM, Dunn TB, Bellin MD, Freeman ML, Schwarzenberg SJ, et al. Long-term outcomes of total pancreatectomy and islet auto transplantation for hereditary/genetic pancreatitis. J Am Coll Surg 2014; 218:530-543. [PMID: 24655839]
- Bellin MD, Gelrud A, Arreaza-Rubin G, Dunn TB, Humar A, Morgan KA, et al. Total pancreatectomy with islet autotransplantation: Summary of anniddk workshop. Ann Surg 2015; 261:21-29. [PMID: 25599324]
- Sutherland DE, Matas AJ, Najarian JS: Pancreatic islet cell transplantation. Surg Clin North Am 1978; 58:365-382.
- Wahoff DC, Paplois BE, Najarian JS, Farney AC, Leonard AS, Kendall DM, et al. Islet autotransplantation after total pancreatectomy in a child. J Pediatr Surg 1996; 31:132-135. [PMID: 8632266]
- Ahmad SA, Lowy AM, Wray CJ, D'Alessio D, Choe KA, James LE, et al. Factors associated with insulin and narcotic independence after islet autotransplantation in patients with severe chronic pancreatitis. J Am Coll Surg 2005; 201:680-687. [PMID: 16256909]
- Clayton HA, Davies JE, Pollard CA, White SA, Musto PP, Dennison AR.Pancreatectomy with islet autotransplantation for the treatment of severe chronic pancreatitis: The first 40 patients at the leicester general hospital. Transplantation 2003; 76:92-98. [PMID: 12865792]
- Manciu N, Beebe DS, Tran P, Gruessner R, Sutherland DE, Belani KG. Total pancreatectomy with islet cell autotransplantation: Anesthetic implications. J Clin Anesth 1999; 11:576-582. [PMID: 10624643]
- Marquez S, Marquez TT, Ikramuddin S, Kandaswamy R, Antanavicius G, Freeman ML, et al. Laparoscopic and da vinci robot-assisted total pancreaticoduodenectomy and intraportal islet autotransplantation: Case report of a definitive minimally invasive treatment of chronic pancreatitis. Pancreas 2010; 39:1109-1111. [PMID: 20861698]
- Wahoff DC, Papalois BE, Najarian JS, Kendall DM, Farney AC, Leone JP, et al. Autologous islet transplantation to prevent diabetes after pancreatic resection. Ann Surg 1995; 222:562-575. [PMIC ID: 1234892]
- Webb MA, Illouz SC, Pollard CA, Gregory R, Mayberry JF, Tordoff SG, et al. Islet auto transplantation following total pancreatectomy: A long-term assessment of graft function. Pancreas 2008; 37:282-287. [PMID: 18815550]
- Wilson GC, Sutton JM, Salehi M, Schmulewitz N, Smith MT, Kucera S, et al. Surgical outcomes after total pancreatectomy and islet cell autotransplantation in pediatric patients. Surgery 2013; 154:777-783. [PMID: 24074415]
- Wang H, Desai KD, Dong H, Owzarski S, Romagnuolo J, Morgan KA, et al. Prior surgery determines islet yield and insulin requirement in patients with chronic pancreatitis. Transplantation 2013; 95:1051-1057. [PMID: 23411743]
- Bottino R, Bertera S, Grupillo M, Melvin PR, Humar A, Mazariegos G, et al. Isolation of human islets for autologous islet transplantation in children and adolescents with chronic pancreatitis. Journal of transplantation 2012; 2012:642787.
- Anazawa T, Balamurugan AN, Bellin M, Zhang HJ, Matsumoto S, Yonekawa Y, et al. Human islet isolation for autologous transplantation: Comparison of yield and function using serva/nordmark versus roche enzymes. Am J Transplant 2009; 9:2383-2391. [PMID: 19663895]
- Balamurugan AN, Breite AG, Anazawa T, Loganathan G, Wilhelm JJ, Papas KK et al. Successful human islet isolation and transplantation indicating the importance of class 1 collagenase and collagen degradation activity assay. Transplantation 2010; 89:954-961. [PMID: 20300051]
- Balamurugan AN, Loganathan G, Bellin MD, Wilhelm JJ, Harmon J, Anazawa T, et al. A new enzyme mixture to increase the yield and transplant rate of autologous and allogeneic human islet products. Transplantation 2012; 93:693-702. [PMID: 22318245]
- Johnson PR, Jones KE: Pancreatic islet transplantation. Seminars in pediatric surgery 2012; 21:272-280.
- Bellin MD, Gelrud A, Arreaza-Rubin G, Dunn TB, Humar A, Morgan KA, et al. Total pancreatectomy with islet autotransplantation: Summary of a national institute of diabetes and digestive and kidney diseases workshop. Pancreas 2014; 43:1163-1171. [PMID: 25599324]
- Andersson A, Korsgren O, Jansson L: Intraportally transplanted pancreatic islets revascularized from hepatic arterial system. Diabetes 1989; 1:192-195. [PMID: 2492004]
- Korsgren O, Jansson L, Andersson A. Effects of hyperglycemia on function of isolated mouse pancreatic islets transplanted under kidney capsule. Diabetes 1989; 38:510-515. [PMID: 2494093]
- avalli AM, Scaglia L, Zangen DH, Hollister J, Bonner-Weir S, Weir GC.Vulnerability of islets in the immediate posttransplantation period.Dynamic changes in structure and function.Diabetes 1996; 45:1161-1167. [PMID: 8772716]
- Wilhelm JJ, Bellin MD, Dunn TB, Balamurugan AN, Pruett TL, Radosevich DM et al. Proposed thresholds for pancreatic tissue volume for safe intraportal islet autotransplantation after total pancreatectomy. Am J Transplant 2013; 13:3183-3191. [PMID: 24148548]
- Rajab A: Islet transplantation: Alternative sites. CurrDiab Rep 2010; 10:332-337. [PMID: 20665132]
- Rafael E, Tibell A, Ryden M, Lundgren T, Savendahl L, Borgstrom B, et al. Intramuscular autotransplantation of pancreatic islets in a 7-year-old child: A 2-year follow-up. Am J Transplant 2008; 8:458-462. [PMID: 18093267]
- Naziruddin B, Iwahashi S, Kanak MA, Takita M, Itoh T, Levy MF.Evidence for instant blood-mediated inflammatory reaction in clinical autologous islet transplantation.Am J Transplant 2014; 14 428-437. [PMID: 24447621]
- Robertson RP, Bogachus LD, Oseid E, Parazzoli S, Patti ME, Rickels MR, et al. Assessment of beta-cell mass and alpha- and beta-cell survival and function by arginine stimulation in human autologous islet recipients. Diabetes 2015; 64:565-572. [PMID: 25187365]
- Angst MS, Clark JD: Opioid-induced hyperalgesia: A qualitative systematic review. Anesthesiology 2006; 104:570-587. [PMID: 16508405]
- Wilson GC, Sutton JM, Abbott DE, Smith MT, Lowy AM, Matthews JB, et al. Long-term outcomes after total pancreatectomy and islet cell autotransplantation: Is it a durable operation? Ann Surg 2014; 260:659-665. [PMID: 25203883]
- Hathout E, Chan NK, Tan A, Sakata N, Mace J, Pearce W, et al. In vivo imaging demonstrates a time-line for new vessel formation in islet transplantation. Pediatr Transplant 2009; 13:892-897. [PMID: 19017287]
- Speier S, Nyqvist D, Cabrera O, Yu J, Molano RD, Pileggi A, et al. Noninvasive in vivo imaging of pancreatic islet cell biology. Nat Med 2008; 14:574-578. [PMID: 18327249]
- Bellin MD, Moran A, Wilhelm JJ, O'Brien TD, Gottlieb PA, Yu L, et al. Development of autoimmune-mediated beta cell failure after total pancreatectomy with autologous islet transplantation. Am J Transplant 2015[PMID: 25765064]
- Westermark GT, Westermark P, Berne C, Korsgren O, Nordic Network for Clinical Islet T: Widespread amyloid deposition in transplanted human pancreatic islets. N Engl J Med 2008; 359:977-979. [PMID: 18753660]
- Pohl JF, Limbers CA, Kay M, Pnp AH, Rollins M, Varni JW: Health-related quality of life in pediatric patients with long-standing pancreatitis. J Pediatr Gastroenterol Nutr 2011. [PMID: 18753660]
- Walsh RM, Saavedra JR, Lentz G, Guerron AD, Scheman J, Stevens T, et al. Improved quality of life following total pancreatectomy and auto-islet transplantation for chronic pancreatitis. J Gastrointest Surg 2012; 16:1469-1477. [PMID: 22673773]
- Parmar AD, Sheffield KM, Vargas GM, Pitt HA, Kilbane EM, Hall BL, et al. Factors associated with delayed gastric emptying after pancreaticoduodenectomy. HPB (Oxford) 2013; 15:763-772. [PMID: 23869542]
- Berry AJ: Pancreatic enzyme replacement therapy during pancreatic insufficiency. Nutr Clin Pract 2014; 29: 312-321.
- Webb MA, Chen JJ, Illouz SC, Pollard CA, Dennison B, West KP, et al. The impact of potential islet precursor cells on islet autotransplantation outcomes. Cell Transplant 2013; 22:1041-1051. [PMID: 23007077]

