Keywords
Pancreatic Neoplasms; Risk Factors; Clinical Study;
Adjuvant Chemotherapy; Capecitabine
Abbreviations
RTOG Radiation Therapy Oncology Group; OS
Overall Survival; DFS Disease-Free Survival; PET Positron Emission
Tomography; ESPAC European Study Group for Pancreatic Cancer;
GITSG Gastrointestinal Tumor Study Group; IRB Institutional
Review Board; PDAC Pancreatic Ductal Adenocarcinoma; ASCO
American Society of Clinical Oncology; ESMO European Society for
Medical Oncology; NCCN National Comprehensive Cancer Network;
MRI Magnetic resonance imaging; EUS Endoscopic Ultrasound; CT
Computed Tomography
INTRODUCTION
Pancreatic cancer is one of the most lethal solid organ
malignancies. Pancreatectomy offers the only potential for cure but is only possible in a minority of patients [1]. Even
in those patients who receive adjuvant treatment, majority
of them succumb to death due to metastatic disease [2, 3, 4, 5]. The optimal timing and duration of adjuvant therapy is
not established. A focused guideline update on potentially
curable pancreatic cancer from American Society of
Clinical Oncology (ASCO) recommends adjuvant systemic
chemotherapy for six months starting within eight weeks
of surgery, assuming adequate recovery from surgery [1].
There are no randomized trials addressing the impact of
delayed initiation of adjuvant therapy on outcomes or the
effect of a longer duration of therapy [6, 7]. However, at
least some data support the view that delaying treatment
initiation to allow full recovery from surgery does not
compromise the survival benefit, and modern adjuvant
chemotherapy trials have permitted enrollment up to 12
weeks postoperatively as see in the European Study Group
for Pancreatic Cancer-3 (ESPAC-3) trial [8, 9, 10, 11].
Postoperative surveillance studies have shown that
serial determination of CA 19-9 can detect recurrence or
metastasis of pancreatic cancer several months before
finding clinical or radiologic evidence of disease [12, 13, 14, 15, 16, 17]. Radiation Therapy Oncology Group (RTOG)
9704 study has shown that post-resection CA 19-9 levels are
an important predictor of survival [6]. Moreover, another
adjuvant study, ESPAC-3 study showed that completion
of all 6 cycles of planned adjuvant chemotherapy was an
independent prognostic factor after resection [8].
Any survival benefit of an intensified or maintenance
strategy has not been demonstrated in patients with
persistently elevated CA 19-9; despite the pivotal
Gastrointestinal Tumor Study Group (GITSG) study
suggested continuing bolus 5-FU weekly for 24 months
from time of start of adjuvant therapy [2]. It is likely that
pancreatic cancer cells remain locally and systemically
present despite complete surgical resection. Studies in
animal models demonstrate the potential for widely
disseminated disease to occur before a visible primary
tumor is first detected. It is possible that residual
pancreatic cancer cells may lie dormant in G0 arrest and
only infrequently enter the G1/S phase, so additional or
maintenance chemotherapy may be necessary to maintain
pressure on these cells. Limited data exists to support the
idea of maintenance chemotherapy, though it is intriguing
[18].
Prior to beginning adjuvant therapy, all patients should
undergo formal restaging with CT scans and a serum
level of the tumor marker CA 19-9 [19, 20, 21]. Persistent
postoperative elevations of the serum tumor marker CA
19-9 are associated with poor long-term prognosis [22, 23, 24, 25, 26]. However, CA 19-9 levels are prognostic and not
predictive of benefit from adjuvant therapy. While some
suggest withholding adjuvant therapy from such patients
or treating them as if they have advanced metastatic
disease, and some adjuvant therapy protocols, such as
Radiation Therapy Oncology Group (RTOG) 0848, only
allow enrollment if the post-treatment CA 19-9 level is ≤
180 units/mL [16].
As mentioned earlier that the GITSG study effectively
used a maintenance approach by continuing bolus 5-FU
for up to 2 years [2]. Additionally, several trials have
evaluated maintenance chemotherapy in advanced
pancreatic cancer, but no prospective studies have been
done following adjuvant therapy for patients with resected
pancreatic cancer, including those with elevated tumor
makers [18]. The majority of recurrences after potentially
curative treatment of pancreatic exocrine cancer occurs
within two years, and they can be locoregional or to distant
sites, most often the liver, lung, and peritoneal cavity. In
one autopsy series of patients with known pancreatic
cancer, approximately 30% died with locally destructive
disease without evidence of metastases, while 70% died
with widespread metastatic disease [27].
We performed a retrospective analysis of patients
treated at our centers to investigate any benefit of
maintenance and/or additional chemotherapy following
planned 6 months of adjuvant therapy in these patients. As a
secondary objective, we collected data to describe the toxicity
associated with additional/maintenance chemotherapy.
PATIENTS AND METHODS
We conducted a retrospective chart review of
patients who were treated for pancreatic cancer. Patients
were selected who had pathology-proven pancreatic
adenocarcinoma, had undergone surgical resection with
curative intent from 2005-2017, and had received adjuvant
chemotherapy with or without chemo-radiation. CA 19-9
was performed monthly and CT or MRI every 2-3 months.
Patients who had recurrence of disease while on
adjuvant chemotherapy were excluded. Of the patients
25 met the inclusion criteria: R0 surgery, post-surgery
elevated levels of CA 19-9, absence of radiographic
including EUS evidence of cancer. Recurrent pancreatic
cancer was confirmed either biopsy or PET scan after
a multidisciplinary discussion. These patients received
various chemotherapy regimens: schedule, dosage and
duration were collected. In patients who showed toxicity,
the dose was adjusted according to standard guidelines.
Charts were reviewed to determine adverse events
attributed to chemotherapy.
Primary end points for analysis were disease free
survival (DFS) and overall-survival (OS). Descriptive
statistics (e.g., mean, median, range, and proportion) were
used to describe patients' demographic information. SAS
software (version 9.3; SAS Institute Inc., Cary, NC) was
used to perform the analyses. The study was approved by
our institutional review board (IRB).
RESULTS
The demographics are summarized in Table 1. Seven
patients did not have pre-operative CT scan of chest while
nine patients did not have their pre-operative CA 19-9
measured.

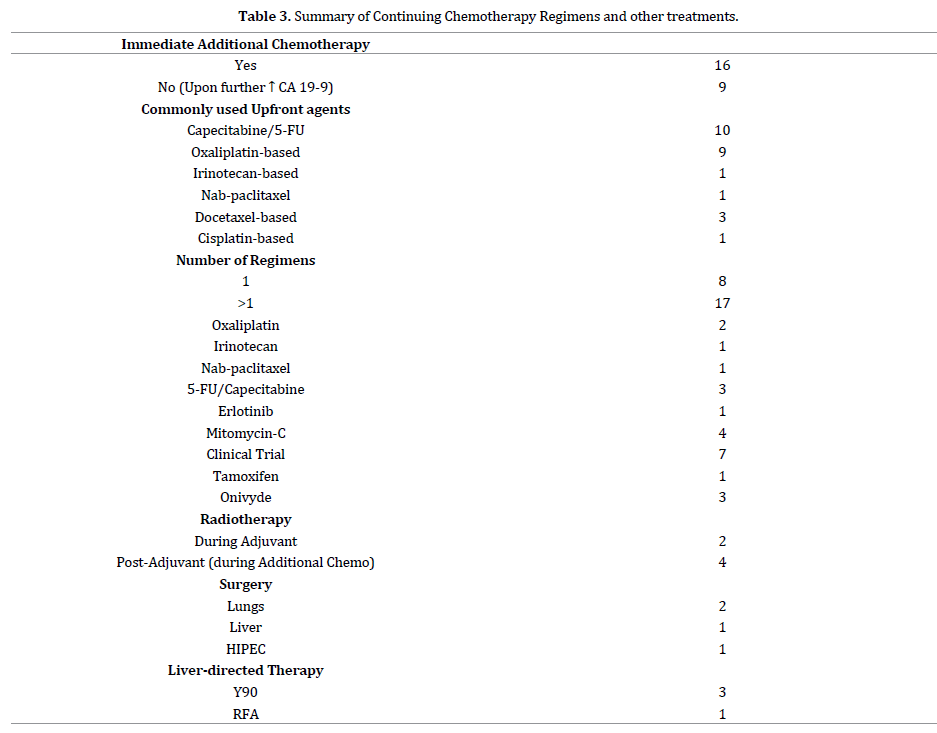
Maintenance chemotherapy agents included 5-FU,
capecitabine, palatinates [cisplatin, oxaliplatin], irinotecan
and nab-paclitaxel. Capecitabine was the most commonly
used agent (n=10), selected due to convenience of oral
administration as well as relatively favorable toxicity,
followed by FOLFOX/XELOX (n=5), gemcitabineoxaliplatin
(n=3), GTX (gemcitabine, docetaxel,
capecitabine) 9n=3) gemcitabine-cisplatin (n=1),
gemcitabine-nab-paclitaxel (n=1) and FOLFIRI (n=1)
(Table 2). Overall the chemotherapy was well tolerated
with expected toxicities.

Most common sites of metastases included liver
(n=12), lungs (n=7), peritoneum (n=4), tumor bed (n=2)
and lymph nodes (n= 2). One patient never showed any
radiological evidence of cancer (Table 2).
The average duration of therapy was 6.42 months
(range, 3-12) till the recurrent or metastatic cancer
was diagnosed. CA 19-9 normalized in 3 patients while
22 remained stable or further elevated. Two patients
underwent metastatectomy. Median DFS was 14.5m (9-
18), OS 29m (19-96) and OS rates were 80 %, 50 % at 1
and 2 years respectively.
DISCUSSION
It is evitable from our study that post-surgery CA 19-9
warns about the persistent cancer or a hidden microscopic
locus [10]. In addition, absence of pre-op CA 19-9 can
further complicate the decision for additional or adjuvant
therapy course. Life expectancy of pancreatic ductal
adenocarcinoma (PDAC) patients is usually short and
selection of the most appropriate treatment is crucial.
Maintenance therapy has become quite a hot topic
especially in metastatic setting for pancreatic cancer
with BRCA mutation as well as in other tumors, such as
colorectal in which oxaliplatin is administered for certain number of cycles and then omitted while continuing
other agents, including targeted agents [28, 29, 30].
Given that we now have more management tools at our
disposal, and as treatments given chronically have become
more tolerable, we tested our strategies by offering a
maintenance approach to patients with pancreatic cancer
with an elevated tumor marker. We believe that the longer
OS of our patients with elevated CA 19-9 post-surgery was
due to additional/maintenance chemotherapy following
the planned 6-months of adjuvant treatment. Ideally, we
could find a biomarker of benefit for patients who should
be managed this way, but thus far we have had no such luck.
We can speculate that survival benefit associated with
the use of additional/maintenance chemotherapy, and not
chemo-radiation as prolonged exposure to therapy, could
potentially maintain pressure on dormant cancer cells that
remain in G0 arrest, by attacking them as they infrequently
enter G1/S. Though no evidence to support this hypothesis
but many adjuvant studies support it. Completion of all
six cycles of planned adjuvant chemotherapy was an
independent prognostic factor after resection according
to the ESPAC-3 study [9]. The study showed that median
OS was 28 months for patients who completed the full
six months of therapy versus 15 months for those who
did not (hazard ratio (HR) for death 0.51, 95% CI 0.44-
0.60). Any survival benefit of an intensified chemotherapy
strategy has not been demonstrated in patients with
persistently elevated CA 19-9. Our study tried to focus on
all these important issues and set the platform for future
prospective clinical trials.
Additionally, our study underlines the importance
of collecting pre-surgery CA 19-9 and complete staging
including chest as many had those tests missed. Prior to
beginning adjuvant therapy, all patients should undergo
formal restaging with CT scans and a serum level of the
tumor marker CA 19-9. Persistent postoperative elevations
of the serum tumor marker CA 19-9 are associated with
poor long-term prognosis. CA 19-9 exists as an epitope
of sialylated Lewis A blood group antigen and it is not
expressed in subjects with Lewis α-β- genotype, which
accounts for approximately 5-10% of the Caucasian
population [31]. RTOG 9704 study has shown that postresection
CA 19-9 levels are an important predictor of
survival [10]. Patients were grouped as having a postresection
CA 19-9 of >90 or <90. 385 patients had CA
19-9 levels tested and recorded, and of these, 132 were
found to not express CA 19-9, leaving 253 patients for
analysis. 200 (79%) had values <90, 53 (21%) were
>90. The researchers found that these groups were
significant predictors of survival. Median survival for the
<90 group was 22.8 months, compared with 9.6 months
for the >90 group. Three-year survival was 33% in the
<90 group versus 2% in the >90 group. These results
showed that post-resection CA 19-9 values >90 were
associated with significantly worse survival in patients
with pancreatic carcinoma according to RTOG 9704
study [10]. It implies that separating patients into these
groups based on CA 19-9 levels may better clarify who
benefits most from combination therapy in future trials,
something we were able to further support in our study.
Park JW et al recruited 1,446 patients with pancreatic
cancer and excluded those with Lewis antigen negative
or obstructive jaundice to eliminate the false effects
on CA 19-9 level [32]. The clinic-pathologic factors were
reviewed including initial and post-treatment CA 19-9, and
statistical analysis was done to evaluate the association
of clinic-pathologic factors with OS. They observed that
patients with normalized post-operative CA 19-9 had
significantly longer OS and DFS regardless of initial CA
19-9 level.
Previously, some investigators suggested withholding
adjuvant therapy from such patients with elevated CA
19-9 and treating them as if they have advanced metastatic
disease [16]. Postoperative CA 19-9 level was found
higher in patients with microscopically positive surgical
margin as well as with hepatic recurrence and peritoneal
dissemination. Whether and how to use preoperative
levels of the serum CA 19-9 to select the initial therapeutic
strategy remains controversial.
Our experience and other reports also suggest that
elevated levels of CA 19-9 can help to predict the presence
of radiographically occult metastatic disease, the likelihood
of a R0 resection, and long-term outcomes in patients
with potentially resectable pancreatic cancer. We have
practiced that high levels of CA 19-9 may guide surgeons
to better identify the patients who may need staging
laparoscopy. However, it is important to notify here that
the ASCO recommended against the use of CA 19-9 alone
as an indicator of operability [33] and we conclude that a
multi-disciplinary approach must be taken in these cases.
Both National Comprehensive Cancer Network (ESMO)
and National Comprehensive Cancer Network (NCCN)
guidelines lack any recommendation for imaging during
adjuvant therapy. Furthermore, experts do agree that a
neoadjuvant approach can be used before surgery for
patients who had potentially anatomically resectable but
high-risk tumors, including elevated preoperative levels
of CA 19-9. Our study further reassures that serum CA
19-9 levels should also be considered in planning with a
multidisciplinary approach.
Patients who had a treatment-related decline in CA
19-9 levels generally exhibit prolonged median survival.
In a multivariate analysis, a decrease of CA 19-9 during
chemotherapy was found to be an independent prognostic
factor regarding survival [34]. Data suggest that
responders whose CA 19-9 levels were reduced by >50%
of pre-treatment baseline levels have a longer median
survival when compared to CA 19-9 non-responders.
Okusaka et al showed that CA 19-9 responders in locally
advanced pancreatic cancer had a longer median survival
of 10.6 months compared to 4.1 months in non-responders
[35]. Similarly, Ishii et al reported longer median survival
times in CA 19-9 responders of 141 days versus 88 days
in non-responders in advanced pancreatic cancer patients.
The relative risk of cancer death in CA 19-9 responders
versus non-responders was 0.47 (95% CI, 0.21-1.05) [35].
Based on our data, we believe that close monitoring
with monthly CA 19-9 and 3-monthly CT scans also
contributed to a better outcome by identifying any
recurrent or metastatic cancer and by changing treatment.
The median DFS following pancreatectomy and adjuvant
gemcitabine was reported as 13.4 months vs. 6.9 months
for untreated patients in the CONKO-001 trial [5]. Others
have also reported that postoperative surveillance studies
have shown that serial determination of CA 19-9 can detect
recurrence or metastasis of pancreatic cancer several months
before finding clinical or radiologic evidence of disease.
Identification of patients with early recurrence of
pancreatic cancer is an extremely important issue, as
regular staging of the tumor during chemotherapeutic
treatment, e.g., using CT scans, allows the selection of an
appropriate regimen and avoids unnecessary cytotoxic
treatment if surgery is an option. It is important to remind
here that CA 19-9 is increased in multiple gastrointestinal
cancers, including benign diseases, such as peptic ulcers,
chronic and acute pancreatitis, cirrhosis, cholangitis, and
obstructive jaundice. Interestingly enough, poorlydifferentiated
pancreatic cancer is found to produce
less CA 19-9 than moderately- or well-differentiated
cancers. The clinical practice guidelines, such as ESMO,
NCCN do not recommend regular imaging, though our
study and the data discussed above clearly demands
a recommendation for staging post-operatively with
an initial postoperative CT scan, followed by regular
staging every 3 months, especially in patients with
elevated CA 19-9 [36]. In the near future there may be
important molecular prognostic factors for the selection
of appropriate chemotherapy regimens will hopefully
lead to better identification of patients for treatment
than CT follow-up screening.
CONCLUSION
In summary, the rising CA 19-9 levels in patients
under observation or in those receiving active therapy
could be an indicator of disease recurrence, progression,
and ineffectiveness of the current regimen, and may
be correlated with shorter survival time. However, the
value of initiating therapy based on rising CA 19-9 levels
remains to be demonstrated. We made these decisions to
initiate or change chemotherapy based on multiple testing,
multidisciplinary discussions and consent of patients. We
therefore, would remind physicians to be mindful of the
limitations when interpreting the significance of a rising
CA 19-9 and decision to initiate or extend chemotherapy
should be made based on universal guidelines and with
help of expertise at your centre. Future prospective studies
are needed to perform a future study to evaluate role of
maintenance or intensified chemotherapy and explore
patient stratification and selection based on biomarkers in
patient selection for treatment.
Conflicts of Interest
All named authors hereby declare that they have no
conflicts of interest to disclose.
References
- Daoud V, Saif MW, Goodman M. Adjuvant treatment for pancreatic cancer. JOP 2014; 15:348-350. [PMID: 25076340]
- Kalser MH, Ellenberg SS. Pancreatic cancer: adjuvant combined radiation and chemotherapy following curative resection. Arch Surg 1985; 120:899-903. [PMID: 4015380]
- Klinkenbijl JH, Jeekel J, Sahmoud T, van Pel R, Couvreur ML, Veenhof CH, et al. Adjuvant radiotherapy and 5-fluorouracil after curative resection of cancer of the pancreas and periampullary region: phase III trial of the EORTC gastrointestinal tract cancer cooperative group. Ann Surg 1999; 230:776-782. [PMID: 10615932]
- Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med 2004; 350:1200-1210. [PMID: 15028824]
- Oettle H, Neuhaus P, Hochhaus A, Hartmann JT, Gellert K, Ridwelski K, et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: the CONKO-001 randomized trial. JAMA 2013; 310:1473-1481. [PMID: 24104372]
- Regine WF, Winter KA, Abrams RA, et al. Fluorouracil vs gemcitabine chemotherapy before and after fluorouracil-based chemoradiation following resection of pancreatic adenocarcinoma: a randomized controlled trial. JAMA 2008; 299:1019-1026.
- Neoptolemos JP, Stocken DD, Bassi C, Ghaneh P, Cunningham D, Goldstein D, et al. Adjuvant chemotherapy with fluorouracil plus folinic acid vs gemcitabine following pancreatic cancer resection: a randomized controlled trial. JAMA 2010; 304:1073-1081. [PMID: 20823433]
- Neoptolemos JP, Palmer DH, Ghaneh P, Psarelli EE, Valle JW, Halloran CM, et al.Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): a multicentre, open-label, randomised, phase 3 trial. Lancet 2017; 389:1011-1024. [PMID: 28129987]
- Conroy T, Hammel P, Hebbar M, Abdelghani MB, Wei AC, et al.FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N Engl J Med 2018; 379:2395-2406. [PMID: 30575490]
- Uesaka K, Boku N, Fukutomi A, Okamura Y, Konishi M, Matsumoto I, et al.Adjuvant chemotherapy of S-1 versus gemcitabine for resected pancreatic cancer: a phase 3, open-label, randomised, non-inferiority trial (JASPAC 01). Lancet 2016; 388:248-257. [PMID: 27265347]
- Valle JW, Palmer D, Jackson R, Cox T, Neoptolemos JP, Ghaneh P, et al. Optimal duration and timing of adjuvant chemotherapy after definitive surgery for ductal adenocarcinoma of the pancreas: ongoing lessons from the ESPAC-3 study. J Clin Oncol 2014; 32:504-512. [PMID: 24419109]
- Micke O, Bruns F, Kurowski R, Horst E, deVries AF, Hausler JW, et al. Predictive value of carbohydrate antigen 19-9 in pancreatic cancer treated with radiochemotherapy. Int J Radiat Oncol Biol Phys 2003; 57:90-97. [PMID: 12909220]
- Hata S, Sakamoto Y, Yamamoto Y, Nara S, Esaki M, Shimada K, et al. Prognostic impact of postoperative serum CA 19-9 levels in patients with resectable pancreatic cancer. Ann Surg Oncol 2012; 19:636-641. [PMID: 21863360]
- Berger AC, Meszoely IM, Ross EA, Watson JC, Hoffman JP. Undetectable preoperative levels of serum CA 19-9 correlate with improved survival for patients with resectable pancreatic adenocarcinoma. Ann Surg Oncol 2004; 11:644–649. [PMID: 15197014]
- Kang CM, Kim JY, Choi GH, Kim KS, Choi JS, Lee WJ, et al. The use of adjusted preoperative CA 19-9 to predict the recurrence of resectable pancreatic cancer. J Surg Res 2007; 140:31-35. [PMID: 17418869]
- Berger AC, Garcia M Jr, Hoffman JP, Regine WF, Abrams RA, Safran H, et al. Postresection CA 19-9 predicts overall survival in patients with pancreatic cancer treated with adjuvant chemoradiation: a prospective validation by RTOG 9704. J Clin Oncol 2008; 26:5918–5922. [PMID: 19029412]
- Kondo N, Murakami Y, Uemura K, Hayashidani Y, Sudo T, Hashimoto Y, et al. Prognostic impact of perioperative CA 19-9 levels in patients with resectable pancreatic cancer. Ann Surg Oncol 2010; 17:2321-2329. [PMID: 20336387]
- Saif MW, Ledbetter L, Kaley K, Garcon MC, Rodriguez T, Syrigos KN. Maintenance therapy with capecitabine in patients with locally advanced unresectable pancreatic adenocarcinoma. Oncol Lett 2014; 8:1302-1306. [PMID: 25120712]
- Montgomery RC, Hoffman JP, Riley LB, Rogatko A, Ridge JA, Eisenberg BL. Prediction of recurrence and survival by post-resection CA 19-9 values in patients with adenocarcinoma of the pancreas. Ann Surg Oncol 1997; 4:551–556. [PMID: 9367020]
- Ferrone CR, Finkelstein DM, Thayer SP, Muzikansky A, del Castillo CF, Warshaw AL. Perioperative CA 19-9 levels can predict stage and survival in patietns with resectable pancreatic adenocarcinoma. J Clin Oncol 2006; 4:2897-902. [PMID: 16782929]
- Motoi F, Rikiyama T, Katayose Y, Egawa SI, Unno M. Retrospective evaluation of the influence of postoperative tumor marker status on survival and patterns of recurrence after surgery for pancreatic cancer based on RECIST guidelines. Ann Surg Oncol 2011; 18:371–379. [PMID: 20842460]
- Kinsella TJ, Seo Y, Willis J, Stellato TA, Siegel CT, Harpp D, et al. The impact of resection margin status and postoperative CA 19-9 levels on survival and patterns of recurrence after postoperative high-dose radiotherapy with 5-FU-based concurrent chemotherapy for resectable pancreatic cancer. Am J Clin Oncol 2008; 31:446-453. [PMID: 18838880]
- Rapellino M, Piantino P, Pecchio F, Ruffini E, Cavallo A, Scappaticci E, et al. Disappearance curves of tumor markers after radical surgery. Int J Biol Markers 1994; 9:33–37. [PMID: 8051433]
- Boeck S, Stieber P, Holdenrieder S, Wilkowski R, Heinemann V. Prognostic and therapeutic significance of carbohydrate antigen 19-9 as tumor marker in patients with pancreatic cancer. Oncology 2006; 70:255-264. [PMID: 16899980]
- Brennan MF, Kattan MW, Klimstra D, Conlon K. Prognostic nomogram for patients undergoing resection for adenocarcinoma of the pancreas. Ann Surg 2004; 240:293–298. [PMID: 15273554]
- Stemmler J, Stieber P, Szymala AM, Schalhorn A, Schermuly MM, Wilkowski R, et al. Are serial CA 19-9 kinetics helpful in predicting survival in patients with advanced or metastatic pancreatic cancer treated with gemcitabine and cisplatin? Onkologie 2003; 26:462-467. [PMID: 14605463]
- Hishinuma S, Ogata Y, Tomikawa M, Ozawa I, Hirabayashi K, Igarashi S. Patterns of recurrence after curative resection of pancreatic cancer, based on autopsy findings. J Gastrointest Surg 2006; 10:511-518. [PMID: 16627216]
- Saif MW. Does OPTIMOX strategy ("stop-and-go" approach) also work in treatment of pancreatic cancer with oxaliplatin-based regimens? JOP 2008; 9:658-663. [PMID: 18762700]
- Relias V, Maloney A, Smith MH, Saif MW. Does "OPTINAB" strategy ("stop-and-go") work in treatment of advanced pancreatic cancer (APC) with nab-paclitaxel-gemcitabine? Cancer Chemother Pharmacol 2017; 80:371–375. [PMID: 28664225]
- Golan T, Hammel P, Reni M, Cutsem EV, Macarulla T, Hall MJ, et al. Maintenance olaparib for germline BRCA-mutated metastatic pancreatic cancer. N Engl J Med 2019; 381: 317–327. [PMID: 31157963]
- Tempero MA, Uchida E, Takasaki H, Burnett DA, Steplewski Z, Pour PM. Relationship of carbohydrate antigen 19-9 and Lewis antigens in pancreatic cancer. Cancer Res 1987; 47:5501-5503. [PMID: 3308077]
- Park JK, Paik WH, Ryu JK, Kim YT, Kim YJ, Kim J, et al. Clinical Significance and Revisiting the Meaning of CA 19-9 Blood Level Before and After the Treatment of Pancreatic Ductal Adenocarcinoma: Analysis of 1,446 Patients from the Pancreatic Cancer Cohort in a Single Institution. 2013; 8:e78977. [PMID: 24250822]
- Locker GY, Hamilton S, Harris J, Jessup JM, Kemeny N, Macdonald JS, et al. ASCO 2006 update of recommendations for the use of tumor markers in gastrointestinal cancer. J Clin Oncol 2006; 24:5313-5327. [PMID: 17060676]
- Parmar A, Chaves-Porras J, Saluja R, Perry K, Rahmadian AP, Santos SD, et al. Adjuvant treatment for resected pancreatic adenocarcinoma: A systematic review and network meta-analysis. Crit Rev Oncol Hematol 2020; 145:102817. [PMID: 31955005]
- Okusaka T, Okada S, Sato T, Wakasugi H, Saisho H, Furuse J,et al. Tumor markers in evaluating the response to radiotherapy in unresectable pancreatic cancer. Hepatogastroenterology 1998; 45:867-872. [PMID: 9684148]
- Ishii H, Okada S, Sato T, Wakasugi H, Saisho H, Furuse J, et al. CA 19-9 in evaluating the response to chemotherapy in advanced pancreatic cancer. Hepatogastroenterology 1997; 44:279-283. [PMID: 9058159]

