Keywords
Drug Therapy; Molecular Targeted Therapy; Pancreatic Neoplasms
Abbreviations
CapOx: capecitabine and oxaliplatin; FOLFIRINOX: oxaliplatin and irinotecan plus fluorouracil and leucovorin; ICE: irinotecan, cetuximab, and everolimus
Introduction
Advanced pancreatic cancer has a dismal outcome with overall survival of less than 6 months. Singleagent gemcitabine has been the standard of care for last two decades with median overall survival of 6 months and 1-year survival rate of 18% [1]. Many large trials have failed to demonstrated further benefit from adding targeted and chemotherapeutic agents to gemcitabine. Two large phase III trials have changed the landscape of pancreatic cancer. FOLFIRINOX regimen (oxaliplatin and irinotecan plus fluorouracil and leucovorin) improved survival from 6.8 months to 11.1 months (P<0.0001) while the Metastatic Pancreatic Adenocarcinoma Clinical Trial (MPACT) study showed nab-paclitaxel and gemcitabine combination can improve overall survival from 6.7 to 8.5 months [2, 3].
What We Knew Before the 2014 ASCO Gastrointestinal Cancers Symposium
Oxaliplatin and 5-FU based chemotherapy has been a standard second line chemotherapy in gemcitabine refractory pancreatic cancer. The Charité Onkologie Clinical (CONKO) III trial demonstrated that addition of oxaliplatin to 5-FU regimen improved overall survival in second line pancreatic cancer patients. The study was originally designed to enroll 165 patients but pre-maturely closed after 46 patients due to poor accrual since many physicians could not support used of best supportive care in control arm. The study randomly assigned combination of oxaliplatin, leucovorin and 5-FU (OFF) regimen versus best supportive care. Although trial was prematurely closed, the treated patients had median overall survival of 4.8 months compared to 2.3 months in best supportive group [4]. Chung et al. conducted a phase II study using 5- FU, leucovorin and oxaliplatin (FOLFOX)-4 regimen in gemcitabine refractory pancreatic cancer. Among 44 patients treated, disease control rate was 40%, median time to progression was 10 weeks and median overall survival was 31 weeks [5]. Although there is no prospective study using FOLFIRINOX in second line setting, a retrospective analysis of 27 patients showed median time to progression of 5.4 months, and median overall survival was 8.5 months in patients who has failed gemcitabine chemotherapy [6]. Another retrospective study from Korea assessed 18 patients with advanced pancreatic cancer and noted disease control rate of 55%, progression free survival of 2.8 months and overall survival of 8.4 months [7].
Nab-paclitaxel (Abraxane®, Celgene Co., Summit, NJ, USA) has activity as a second-line agent in pancreatic cancer. In a phase II trial, in which 19 patients with gemcitabine-refractory advanced pancreatic cancer received single agent nabpaclitaxel (100 mg/m2 on Days 1, 8, and 15 of each 28-day cycle), one patient had a partial response and 6 patients had stable disease with disease control rate of 37%. Median progression free survival was 1.7 months and overall survival was 7.3 months [8]. Peddi et al. retrospectively assessed 20 patients in Siteman Cancer Center (St. Louis, MO, USA) who received nab-paclitaxel monotherapy in refractory pancreatic cancer. Stable disease was noted in 65% with median progression free survival of 3.7 months and overall survival of 5.2 months showing modest clinical benefit [9]. Nanoliposomal irinotecan (PEP02) was investigated in 40 advanced pancreatic cancer patients. Three patients achieved partial response and 17 patients had stabled disease for 6 weeks with disease control rate of 50%. Median progression free survival was 2.4 months and overall survival was 5.2 months showing clinical activity [10]. Larger phase III trial is currently underway in refractory pancreatic cancer patients.
What We Learned at the 2014 ASCO Gastrointestinal Cancers Symposium
A Phase II Study of Ganetespib (G) as Second- or Third-Line Therapy for Metastatic Pancreatic Cancer (MPC) (Abstract #297 [11])
The abstract examined the role of heat shock protein hsp90 inhibitor ganetespib in refractory pancreatic cancer. Seventeen patients were enrolled, and 14 received ganetespib at 175 mg/m2 weekly x 3 in a four week cycle (Table 1) Eight patients had received one prior line of treatment while 6 patient had received two prior lines of therapy. Grade 3 related toxicities included abdominal pain (n=4), fatigue (n=4), diarrhea (n=4) and hyponatremia (n=9). Disease control at 8 weeks was 21%, and overall survival was 2.5 months [11]. The study was closed pre-maturely for lack of clinical efficacy based on a Simon’s two stage design.
A Randomized Phase I/II Study of Everolimus, Irinotecan, and Cetuximab versus Capecitabine and Oxaliplatin in Gemcitabine-Resistant Patients with Pancreatic Cancer (Abstract #337 [12])
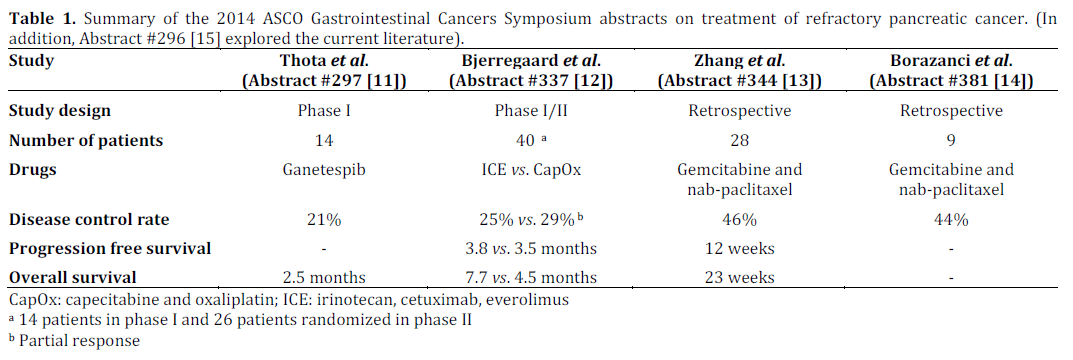
The trial evaluated 40 patients with gemcitabine refractory pancreatic cancer in a phase I/II trial using irinotecan, cetuximab, and everolimus (ICE). Due to dose limiting toxicity (mainly mucositis) at dose level 1 of the phase I trial, the protocol was amended to use everolimus at 2.5 mg daily, irinotecan at 180 mg/m2 and cetuximab at 500 mg/m2 every 14 days. At this dose level patients were randomized to either ICE or capecitabine and oxaliplatin (CapOx). Planned accrual was 90 patients, but due to slow accrual, the study was terminated after randomization of 26 patients. Median progression free survival for the ICE regime was 3.8 months and CapOx was 3.5 months. Median overall survival for ICE was 7.7 and for CapOx 4.5 months [12]. Nine patients cross-overed to alternative regimens: 6 patients from CapOx to ICE, and 3 patients from ICE to CapOx upon progression. Partial response rate for ICE was 25% and 29% for CapOx. As expected, ICE regime had grade III toxicity that included acne-like-rash (20%), fatigue (16%), infection (16%) and thromboembolism (12%). CapOx was associated with grade 3 or greater neuropathy (21%), thromboembolism (14%), pain (21%) and hand foot syndrome (14%).
Second-Line Gemcitabine Plus Nab-Paclitaxel (G+A) for Advanced Pancreatic Cancer (APC) after First- Line FOLFIRINOX: Single Institution Retrospective Review of Efficacy and Toxicity (Abstract #344 [13])
This review retrospectively assessed 28 patients who progressed on first line FOLFIRINOX and treated with nab-paclitaxel and gemcitabine combination at Yale Cancer Center (New Haven, CT, USA) between Dec. 2011 and Dec. 2013. Most of the patients received 6 months of FOLFIRINOX chemotherapy. The study included mostly advanced pancreatic cancer but also included 5 patients with locally advanced pancreatic cancer. There were 5 patients who had partial response and 8 patients who had stable disease for at least 7 weeks. Median time to treatment failure (TTF) was 12 weeks and median overall survival was 23 weeks [13]. However, in these heavily pre-treated patients, the dose intensity of nab-paclitaxel was only 56.9% and 63.5% for gemcitabine. Grade 3 or greater hematologic toxicities included neutropenia (17%), anemia (26%), and thrombocytopenia (26%).
Reinitiating Nab-Paclitaxel Plus Gemcitabine in Patients with Advanced Pancreatic Cancer (Abstract #381 [14])
The small series examined nine patients with advanced pancreatic cancer who were retreated with nab-paclitaxel and gemcitabine combination. The median time between treatments of nabpaclitaxel plus gemcitabine was 7.6 months. 5-FUbased chemotherapy was the most commonly used regimen between treatments [14]. Five of the nine patients received repeat nab-paclitaxel plus gemcitabine more than 6 months after their initial nab-paclitaxel/gemcitabine regimen and four of the nine received repeat nab-paclitaxel plus gemcitabine less than 6 months after their initial treatment. The disease control rate seen for the second treatment with nab-paclitaxel plus gemcitabine was 44% (four of nine patients). Three of nine patients (33%) had treatment a third time with nab-paclitaxel plus gemcitabine, with 2 of 3 of these patients having disease control. In limited number of patients retreatment of nab-paclitaxel plus gemcitabine therapy seems feasible.
Survival Benefit of Second-Line Chemotherapy in Advanced Pancreatic Adenocarcinoma: A Systematic Review of the Literature (Abstract #296 [15])
This abstract explored the current literature on patients receiving first and second line chemotherapy in clinical trials. Twenty first line clinical trials with 42 treatment arms with total of 5,768 patients were analyzed. Overall survival was positively correlated with use of second-line chemotherapy (r=0.65; P=0.012). Sixty-one secondline studies were identified with total of 2,562 patients in 66 treatment arms. Combination treatment was associated with an improved response rate (P=0.045) and progression free survival (P=0.024) when compared to single agent therapy. In this exploratory analysis, these data suggest that there is a small benefit of second-line chemotherapy in pancreatic cancer [15].
Discussion
Pancreatic cancer carcinogenesis involve abnormal expression of Pdx1, hedgehog signaling, K-ras oncogenes and aberration of tumor suppressor genes like p16, p53, and DPC4 [16]. These pathways are fed-forward by frequently cited mutations and aberrant expression of the DNA sequences with many redundant pathways. Therefore the use of single agent targeted therapy will most likely not be effective in pancreatic cancer. Although ganetespib (hsp90 inhibitor) may regulate EGFR, IGF-1_R, cmet and several other pathways, single agent hsp inhibition did not have clinical activity in pancreatic cancer as presented in Abstract #297 [11].
Bjerregaard et al. (Abstract #337 [12]) investigated triplet regime using irinotecan, cetuximab and everolimus (ICE) to block both EGFR and mTOR pathways in pancreatic cancer. The response rate was comparable to CapOx 25% vs. 29% but overall survival was significantly prolonged (7.7 months vs. 4.5 months). Due to early dose limiting toxicity (mucositis) in the initial cohort; the regimen used only 2.5 mg of everolimus. It is uncertain if full blockade of mTOR pathway is exhibited at this dose level. Although the improvement of overall survival is interesting; it is difficult to make any definite conclusion from this small study. Better accrual and collaborations are needed so that we can answer important scientific questions in pancreatic cancer. Current Southwest Oncology Group (SWOG) study S1115 explores if two targeted therapies blocking akt and mek pathway will be beneficial in refractory pancreatic cancer. The study is well-designed and is supported by multiple institutions and will potentially lay out a solid foundation for future second line therapies in pancreatic cancer.
The study conducted by Zhang et al. (Abstract #344 [13]) using gemcitabine and nab-paclitaxel in patients who fails FOLFIRINOX has clinical significance since this is the current practice in United States. The retrospective study confirms that this combination has clinical activity with median time to progression of 12 weeks and overall survival of 23 weeks which is comparable to other active second line regimen. However, the dose intensity used in first line setting of 125 mg/m2 of nab-paclitaxel may not be feasible in heavily pretreated patient population due to myelosuppression. Future studies incorporating single agent nab-paclitaxel and perhaps using Day 1 and 8 of every 3 weeks should be explored in this setting.
Borazanci et al. (Abstract #381 [14]) investigated the clinical utility of re-initiating gemcitabine and nab-paclitaxel after its failure in third and fourth line setting. Although the disease control rate of 44% was noted in this refractory group of patients, it is not clear if these patients actually progressed on the previous therapy or the regimen was changed due to toxicity or logistic reasons. Due to its small sample size the clinical utility of reinitiating gemcitabine and nab-paclitaxel is limited.
Take Home Points
Overall most of the studies presented at the2014 ASCO Gastrointestinal Cancers Symposium were limited by small sample size and two of the abstracts presented were retrospective studies. There is emerging interest in refractory pancreatic cancer at the 2014 ASCO GI Cancers Symposium. Recent review of pancreatic cancer clinical trials in 2011 and 2012 revealed that among 11,786 patients needed for enrollment about 15% of target patients were enrolled in 2011 [17]. At this rate most of the studies will take 6-7 years to complete patient accrual and science behind most studies will be outdated. Higher level of collaboration between academia, community practice and pharmaceutical industry is definitely needed to increase the population of patients who will be enrolled in clinical trials leading to larger randomized studies. In the future we hope that rational randomized clinical design can be initiated and completed to answer critical questions in refractory pancreatic cancer.
Conflict of interest
Dr. Choi received honorarium from Celgene Co. (Summit, NJ, USA). No funding was received for this study. The other authors report no conflicts of interest in this work.
References
- Burris HA, III, Moore MJ, Andersen J et al. Improvements in survival and clinical benefit with gemcitabine as first- line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol. 1997;15:2403-2413.
- Conroy T, Desseigne F, Ychou M, Bouche O, Guimbaud R, Becouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. The New England Journal of Medicine. 2011 May 12;364(19):1817.
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. The New England Journal of Medicine. 2013 Oct 31;369(18):1691-703.
- Pelzer U, Schwaner I, Stieler J, Adler M, Seraphin J, Dörken B et. al. Best supportive care (BSC) versus oxaliplatin, folinic acid and 5-fluorouracil (OFF) plus BSC in patients for second-line advanced pancreatic cancer: a phase III-study from the German CONKO-study group. Eur J Cancer. 2011;47(11):1676.
- Chung JW, Jang HW, Chung MJ et.al. Folfox4 as a rescue chemotherapy for gemcitabine refractory pancreatic cancer. Hepatogastroenterology 2013 Mar-Apr; 60(122):363-7.
- Assaf E, Verlinde-Carvalho M, Delbaldo C, et al. 5-fluorouracil/leucovorin combined with irinotecan and oxaliplatin (FOLFIRINOX) as second-line chemotherapy in patients with metastatic pancreatic adenocarcinoma. Oncology 2011; 80:301.
- Lee MG, Lee SH, Lee SJ, et. al. 5-Fluorouracil/Leucovorin Combined with Irinotecan and Oxaliplatin (FOLFIRINOX) as Second-Line Chemotherapy in Patients with Advanced Pancreatic Cancer Who Have Progressed on Gemcitabine-Based Therapy. Chemotherapy 2014 Jan 18;59(4):273-279.
- Hosein PJ, Pastorini VH, Gomez CM, A phase II trial of nab-paclitaxel (NP) in patients with advanced pancreatic cancer Am J Clin Oncol. 2013 Apr;36(2):151-6.
- Peddi PF, Co M, Wang J, et.al. Nab-paclitaxel montherapy in refractoy pancreatic adenocarcinoma J Gastrointest Oncol 2013 Dec;4(4):370-3.
- Ko AH, Tempero MA, Shan YS, et. al. A mutinational phase 2 study of nanoliposomal irinotecan surcosofate (PEP02, MM-398) for patients with gemcitabine refractory metastatic pancreatic cnacer. Br J Cancer. 2013 Aug 20;109(4):920-5.
- Thota R, Goff LW, Chan E. et.al. A phase II study of ganetespib (G) as second- or third-line therapy for metastatic pancreatic cancer (MPC). 2014 ASCO Gastrointestinal Cancers Symposium. Abstract No. 297.
- Bjerregaard JK, Ladekarl M, Farr KP et. al. , A randomized phase I/II study of everolimus, irinotecan, and cetuximab versus capecitabine and oxaliplatin in gemcitabine-resistant patients with pancreatic cancer. 2014 ASCO Gastrointestinal Cancers Symposium. Abstract No.337.
- Zhang Y, Hochster HS, Stein S et. al. , Second-line gemcitabine plus nab-paclitaxel (G+A) for advanced pancreatic cancer (APC) after first-line FOLFIRINOX: Single institution retrospective review of efficacy and toxicity. 2014 ASCO Gastrointestinal Cancers Symposium. Abstract No.344.
- Borazanci E, Schroeder K , Jameson GS et. al. , Reinitiating nab-paclitaxel plus gemcitabine in patients with advanced pancreatic cancer. 2014 ASCO Gastrointestinal Cancers Symposium. Abstract No.381.
- Nagrial A, Chin VT, Sjoquist K et. al. . Survival benefit of second-line chemotherapy in advanced pancreatic adenocarcinoma: A systematic review of the literature. . 2014 ASCO Gastrointestinal Cancers Symposium. Abstract No. 296.
- Vincent A, Herman J, Schulick R, Hruban RH, Goggins M. Pancreatic cancer. Lancet. 2011 Aug 13;378(9791):607-20.
- Hoos WA, James PM, Rahib L, et.al. Pancreatic cancer clincial trials and accrual in the United States. J. Clin Oncol. 2013 Sep 20:31 (2&):3432-8.

