Vujasinovic Miroslav1, Martin Tretjak2, Bojan Tepes3, Apolon Marolt2, Cirila Slemenik Pusnik2, Mateja Kotnik Kerbev2, Sasa Rudolf4
1Medicinkliniken, Vrinnevisjukhuset, Gamla Övägen 25, 603 79 Norrköping, Sweden
2Department of Internal Medicine, Slovenj Gradec General Hospital, Gosposvetska 1, 2380 Slovenj Gradec, Slovenia
3Abakus Medico Diagnostic Centre, Prvomajska 29, 3250 Rogaska Slatina, Slovenia
4Department of Radiology, University Medical Centre Maribor, Ljubljanska 5, 2000 Maribor, Slovenia
*Corresponding Author:
Miroslav Vujasinovic
Medicinkliniken, Vrinnevisjukhuset
Gamla Övägen 25, 603 79 Norrköping, Sweden
Phone +46 10 104 3554
E-mail mvujas@gmail.com
Received: October 16th, 2015 Accepted: December 10th, 2015
Keywords
Exocrine Pancreatic Insufficiency; Heart Failure
Abbreviations
CHF chronic heart failure; FE1 faecal elastase-1; PEI pancreatic exocrine insufficiency; NYHA New York health association
INTRODUCTION
Pancreatic exocrine insufficiency (PEI) is associated with various pancreatic illnesses and could be associated with extrapancreatic diseases [1]. Chronic heart failure (CHF) is a multi-organ disease with increasing evidence for the involvement of the gastrointestinal (GI) system in this syndrome [2].
The pancreas is an exocrine and endocrine gland of the digestive system. The exocrine segment represents 95-99% of the total pancreatic mass and consists of serous acini of highly polarized cells that produce digestive enzymes (amylase, lipase, phospholipase) as well as proenzymes (elastase, procarboxypeptidase, trypsinogen, pepsinogen, deoxyribonuclease, ribonuclease). Once secreted with water and bicarbonates into the lumen of the acinus, they become activated and forwarded through the ductal network to the duodenum, for the intestinal digestion of nutrients [3]. The pancreas is a highly vascularized organ, which has been confirmed with realtime, multidimensional in vivo imaging [4]. The splanchnic circulation normally receives approximately one-quarter of the cardiac output [5]. In all CHF patients, the splanchnic circulation is decreased, and if this state is prolonged, tissue damage to the splanchnic organs is possible.
On the basis of the known data on the splanchnic circulation, we hypothesized that PEI is possible in CHF patients.
The aims of this study were to determine whether the exocrine pancreatic function is impaired in patients with CHF and to assess its clinical significance.
To the best of our knowledge, this study is the first to report on a possible association between PEI and CHF.
METHODS
Patients
The patients were selected from the cardiology outpatient clinic at Slovenj Gradec General Hospital. The medical records were analysed, and a detailed medical history, physical examination and laboratory testing were performed. The patients were Slovene (Caucasians) and over 18 years old, and each patient provided informed consent prior to participating in the study.
Measurement of Laboratory Tests
Faecal elastase-1 (FE) measurements were performed using the enzyme-linked immunosorbent assay (ELISA) method and a commercial kit from ScheBo Biotech (Giessen, Germany). The FE1 results are expressed in μg/g of stool. Levels of >200 μg/g, 100-200 μg/g and <100 μg/g were considered as normal pancreatic exocrine function, mild pancreatic exocrine insufficiency and severe pancreatic insufficiency, respectively. In the patients with low FE (<200 μg/g), a further work-up was performed including the following laboratory measurements: the serum haemoglobin, mean corpuscular volume, lymphocytes, iron, ferritin, transferrin, vitamin B12, folic acid, ionized calcium, phosphorus, magnesium, selenium, zinc, manganese, copper, potassium, sodium, chloride, aspartate aminotransferase, alanine aminotransferase, gamma glutamyl transferase, alkaline phosphatase, bilirubin, amylase, lipase, carbohydrate deficient transferrin, vitamin D, vitamin A, vitamin E, albumin, prealbumin, total proteins and cholesterol.
Ethics
The study was approved by the National Medical Ethics Committee of the Republic of Slovenia (number 121/01/12 on February, 2nd 2012).
Statistical Methods
The data are shown as numerous (%) and the mean ± standard deviation.
RESULTS
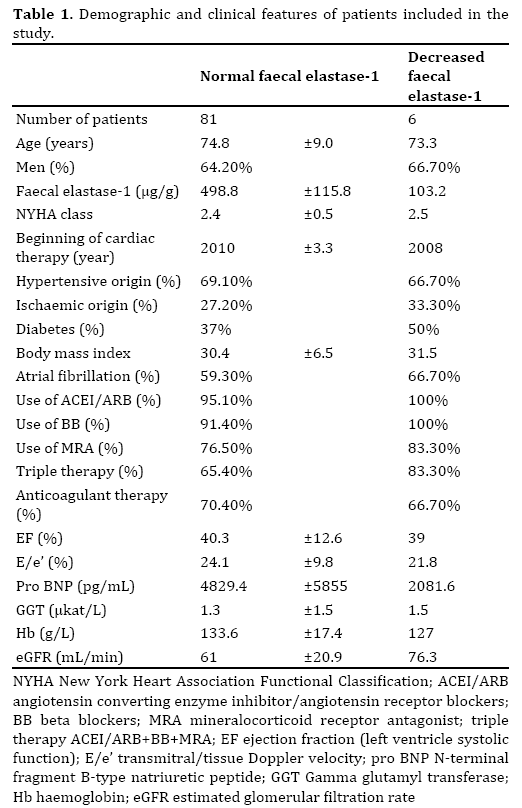
In total, 87 patients were included in the study; there were 56 (64.4%) males and 31 (35.6%) females, and the mean age was 74.7±8.9 years (range 48-90).There were 54 patients with NYHA II and 33 patients with NYHA III CHF. The mean time from confirmation of CHF to inclusion in the study was 4.0±3.3 years. PEI was diagnosed in six (6.9%) patients as follows: severe PEI was diagnosed in three (3.45%) patients, and mild PEI in three (3.45%) patients. None of the patients with PEI had classic clinical gastrointestinal symptoms of PEI (Table 1).
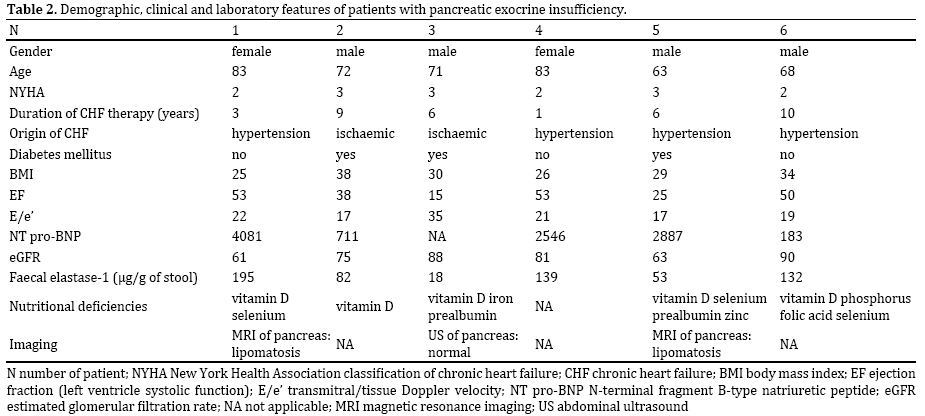
In all of the tested patients with PEI, nutritional serum markers were decreased (vitamin D, selenium, phosphorus, zinc, folic acid and prealbumin). An MRI of pancreas was advised for all of the patients with PEI; two patients agreed to MRI examination (three patients declined all radiological imaging, and one requested an abdominal ultrasound).
DISCUSSION
The FE level was low in six (6.9 %) patients, suggesting that PEI as a result of decreased splanchnic circulation is possible in CHF patients.
Additionally, the clinical significance of PEI was assessed in this study by using a complete laboratory serum nutritional panel. None of the PEI positive patients had typical symptoms, such as abdominal pain, bloating, steatorrhoea and weight loss, which are traditionally the most important criteria for diagnosis and monitoring treatment success [6]. At least one serological nutritional marker was below the lower limit of normal in all of the tested patients (Table 2), which confirms the importance of maldigestion, malnutrition and serum nutritional markers in PEI [7, 8]. Previous studies have shown the importance and clinical significance of the serum nutritional status in patients with chronic pancreatitis (CP) [7, 8]; however, we demonstrated, as well, low serological nutritional markers in patients with PEI without radiological signs of CP. In three of six patients with PEI, radiological imaging was performed (three patients declined), showing fatty infiltration of the pancreas without any diagnostic criteria for chronic pancreatitis. The biggest limitation of present study is the absence of control group of patients. Considering that we have done just a pilot study, we must emphasize that only further studies with age and gendermatched patients in control group can definitely confirm or reject our hypothesis.
Numerous direct pancreatic function tests have been used in the past for the diagnosis of PEI, including the secretin-pancreozymin test, endoscopic secretin test and Lundh test [1]. Over the last 25 years, FE became a suitable method for non-invasive diagnosis of PEI with high specificity and sensitivity, particularly for a severe form of PEI (<100 μg/g). It is now recommended as the first step in pancreatic exocrine function diagnostics [1, 6]. Additionally, the use of FE-1 as a diagnostic tool could be a limitation factor in the study because of its lower sensitivity for mild and moderate PEI, which is a common problem with all non-invasive diagnostic methods. Secretin magnetic retrograde cholangiopancreatography (sMRCP), which is currently used in routine clinical practice, could be useful for a definitive determination of pancreatic morphology and exocrine function in this group of patients.
A study on patients with cardiac cachexia in which PEI might play an important role would be interesting.
CONCLUSIONS
Our study confirmed that PEI could develop in a low percentage of patients with CHF. None of the six patients with PEI had classical clinical signs of PEI; however, all of the patients had lowered serum nutritional markers. Further studies are necessary for a better understanding of the possible connection between these two conditions.
CONTRIBUTORS: VM, TM and TB designed the study and drafted the manuscript; VM, MA, PSS and KKM recruited the patients; SR performed the radiological imaging. All of the authors wrote the manuscript and approved the final version.
ETHICS APPROVAL: The study was approved by the National Medical Ethics Committee of the Republic of Slovenia (number 121/01/12 on February 2nd, 2012).
Conflict of Interest
The authors declare that they have no competing interests.
References
- Löhr JM. Exocrine pancreatic insufficiency, 2nd edition. Bremen: UNI-MED, 2010.
- Krack A, Sharma R, Figulla HR, Anker SD. The importance of the gastrointestinal system in the pathogenesis of heart failure. Eur J Heart Fail 2005; 26:2368-74. [PMID: 15980032]
- Bonal C, Herrera PL. Genes controlling pancreas ontogeny. Int J Dev Biol 2008; 52:823-835. [PMID: 18956314]
- Nyman LR, Wells S, Head WS, McCaughey M, Ford E, Brissova M et al. Real-time, multidimensional in vivo imaging used to investigate blood flow in mouse pancreatic islets. J Clin Invest 2008; 118:3790-7. [PMID: 18846254]
- Ralevic V. Splanchnic circulatory physiology. Hepatogastroenterology 1999; 46:1409-13. [PMID: 10431701]
- Löser C, Möllgaard, Fölsch UR. Faecal elastase 1: a novel, highly sensitive and specific tubeless pancreatic function test. Gut 1996; 39:580-6. [PMID: 8944569]
- Lindkvist B, Dominguez-Munoz JE, Luaces-Regueira M, Castineiras-Alvarino M, Nieto-Garcia L, Iglesias-Garcia J. Serum nutritional markers for prediction of pancreatic exocrine insufficiency in chronic pancreatitis. Pancreatology 2012; 12:305-10. [PMID: 22898630]
- Dominguez-Munoz JE, Iglesias-Garcia J. Oral pancreatic enzyme substitution therapy in chronic pancreatitis: is clinical response an appropriate marker for evaluation of therapeutic efficacy? JOP 2010; 11:158-62. [PMID: 20208327]

