Keywords
Cholecystectomy; Pancreatitis; Recurrence
Abbreviations
CT computed tomography; ERCP endoscopic
retrograde cholangiopancreatography; MRCP magnetic resonance
cholangiopancreaticography
INTRODUCTION
The etiology and common pathogenesis of acute
pancreatitis were investigated for centuries. The potential
pathogenetic theories are controversial; mostly due to
biliary or non-biliary factors, and also can be idiopathic
which occur due to unknown reasons. Biliary pathologies
are 80-90% reason of acute pancreatitis. Among these;
the most common cause is the gallstone impacting the
confluence at the distal common bile duct and pancreatic
duct [1, 2]. In the studies done about biliary pancreatitis; it has been noticed that biliary stones are seen with a
percentage of 88% in radiologic and fecaloid tests of the
patients. Modern life style and dietary habits increase
the incidence of cholelithiasis [3]. Patient history,
physical examination, laboratory tests and radiologic
studies are used to make the diagnosis of acute biliary
pancreatitis. Conservative approach, surgery, endoscopy
and interventional radiology are the main choices used
in the treatment. Acute biliary pancreatitis has a clinical
course varying from a mild attack, which usually subsets
in a few days to a severe clinic with local (pseudocyst,
phlegmon, abscess, necrosis) and systemic (Multiple
organ failure, disseminated intravascular coagulation,
acute respiratory distress syndrome, etc.) complications,
and even sometimes leading to death, which require long
periods of hospital stay [4].
Laparoscopic cholecystectomy is the gold standard
approach to prevent acute biliary pancreatitis attacks. The
authors usually suggest surgery when the clinic of acute
biliary pancreatitis subsets and liver enzymes start to
decrease [5].
In this study; we evaluated the patients with the
clinic of acute biliary pancreatitis whom have a history of
cholecystectomy because of cholelithiasis. Patients having
history of cholecystectomy should be examined more
carefully compared to the ones without cholecystectomy.
MATERIAL AND METHOD
We performed a retrospective analysis of acute biliary
pancreatitis (ABP) patients at the Istanbul Faculty of
Medicine, Department of General Surgery from January
2012 to December 2015. During this period, 246 patients
with acute biliary pancreatitis were identified. Thirtyone
patients who had previously had cholecystectomy
from these patients were included in the study. All clinical
records were retrospectively reviewed. Acute biliary
pancreatitis was diagnosed with elevated serum and
urinary amylase level and biliary pain.
Oral intake was stopped after diagnosis. Analgesic
therapy had been ordered. Informed consent was obtained
from all participants, and study followed the guidelines of
the Declaration of Helsinki. Study protocol was approved
by institutional ethics committee.
The patients having calculus in the biliary tract without
cholecystectomy history (cholecystocholedocholithiazis)
and the ones with known biliary calculus who have a
record of pancreatitis attack after cholecystectomy had
been included in the study. In the most updated studies;
the appropriate time to make cholecystectomy after acute
cholecystitis attack has been stated as in the following
three days or after six weeks. In our study, we discussed
the clinical course of the patients who undergone
cholesystectomy at different time intervals (Figure 1).
Figure 1. Normal appearance of ductus choledochus on MRCP after cholecystectomy (left) Calculi detected in the bile duct on MRCP after cholecystectomy
(right).
Malignancy, history of trauma, enfection and alcohol
induced pancreatitis, hyperlipoproteinemia, congenital
pancreas anomally (pancreatic divisum etc.) and
hyperlipidemia are excluded from the study.
All patients were viewed by USG at the
admission. Hepatobiliary USG was a helpful tool on
determining to prefer MRCP (Magnetic Resonance
Cholangiopancreatiography). Patients having high levels
of cholestatic enzymes (ALP, GGT, and Billirubins) above
the normal range were screened with MRCP to rule out any
calculus, or other obstructive lesion in the biliary tract.
Oral contrast enhanced abdominal angiographic
computerized tomography (CT) was preferred for the
patients having Ranson value above three, or with
increasing values of white blood cells (WBC) and C-reactive
protein (CRP) (Figure 2).
Figure 2. Thirty three year-old woman with acute biliary pancreatitis who underwent extracting stones from the common bile duct with ERCP after cholecystectomy.
Ranson and Balthazar scores are determined at the time
of admission. Patients are classified according to revised
Atlanta classification system as mild, moderate or severe.
Patients aged who were diagnosed with necrotizing
pancreatitis, primary sclerosing cholangitis, pseudocysts,
non-biliary pancreatitis, intrahepatic lithiasis, primary
biliary cirrhosis, gall bladder and biliary duct tumors, or
drug-induced pancreatitis; and those who did not accept
undergoing an operation were excluded from the study.
Patients were evaluated according to differences in
age, gender, cholecystectomy history, blood tests results,
morbidity-mortality rates, invasive procedures done and
the average length of hospital stays.
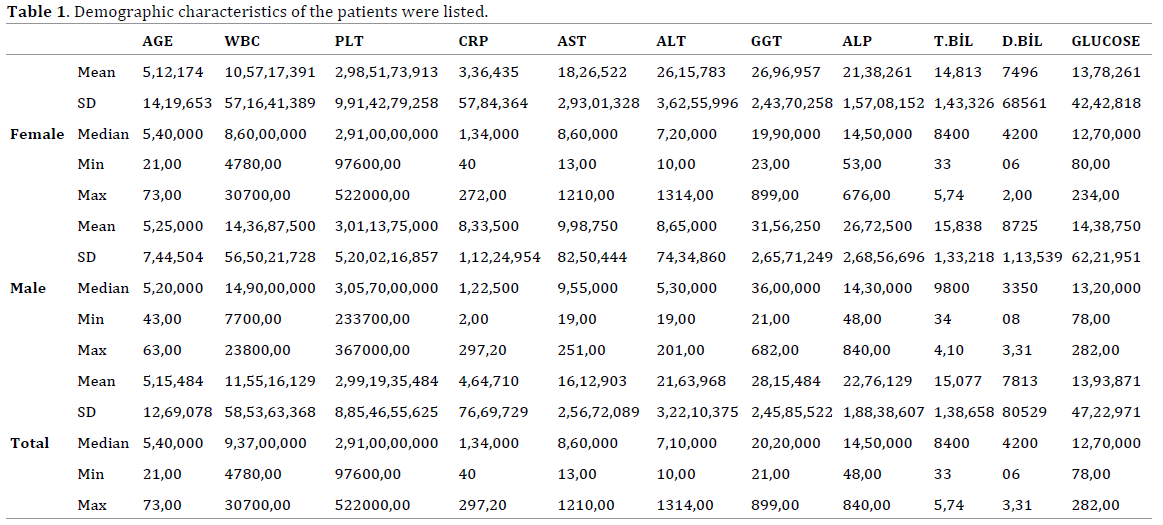
RESULTS
Thirty-one patients were enrolled in the study. Median
age was 51.5 (21-73). There were eight men (median age:
52.5 (43-63)) and 24 women (median age: 51.2 (21-73))
(Table 1).
There was no pathologic finding in abdominal USG
of 20 patients. In 11 patients; indirect findings of biliary
pancreatitis were detected as choledocholithiasis, dilated
choledochus, dilated wirsung and dilatation of intra-extra hepatic biliary tree. Twenty-three patients were screened
with MRCP. Biliary calculus and dilatation had been
detected ın 17 of these patients. Biliary tract was normal
in six of these patients.
Two patients having a Ranson score above three and
increasing values of WBC and CRP had been viewed with
oral contrast enhanced angiographic abdominal CT at
the time of admission. One patient had been screened
with CT due to high WBC and CRP levels, and edematous
pancreatitis was detected. CT was performed to the other
patient due to the contraindication of MRI screening, and
choledocholitiazis and bile duct dilatation was observed.
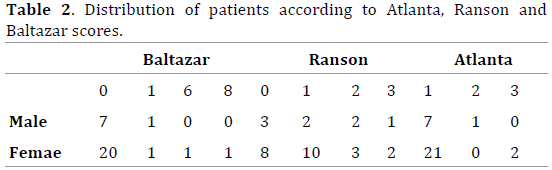
Average Ranson score calculated was 1. For revised
Atlanta scoring system, 28 of the patients were evaluated
as mild, one as moderate, and two of them were severe.
In two of the severe cases, necrosis was seen on the CT
scan, and edematous pancreatitis was found in one of the moderate case. Average Balthazar score found for the mild
cases were 0, moderate ones; 0, and for the severe cases as
seven (Table 2).
Ten of the patients had once a history of ERCP, three
others had twice ERCP record. ERCP was performed to
19 patients (61%) whom were considered as mechanical
obstruction radiologically and clinically. Stone extraction
from common bile duct was performed in 12 patients
during the ERCP procedure. No stone was detected in seven
patients. Decision to perform ERCP was made according to
clinical course (cholestatic enzyme levels) and radiologic
screenings of the patients (Abdominal USG and MRCP).
ERCP was performed for three of the patients because of
elevated cholestatic enzymes and bilirubin levels although
radiologically the biliary tract was normal. Severely
infected necrotizing pancreatitis had occurred in two of the
patients and it was fatal due to sepsis and multiple organ failure in these patients. Percutaneous drainage procedure
was performed to one patient after a collection was
detected in the gall bladder bed. Average length of hospital
stay was 4-5 days (1-13 days). There was no correlation
among CRP levels, necrosis and clinical severity. There has
been confirmed a time interval ranging from a few days
to years between the time of cholecystectomy and first
recurrence of biliary pancreatitis.
DISCUSSION
Accurate patient history and essential physical
examination have paramount importance in reaching the
diagnosis of pancreatitis. The patient must be questioned
about a possible biliary colic history. The patients mostly
complain with severe epigastric pain radiating to the back.
This is usually accompanied by abdominal distension
(could be secondary to intraperitoneal collection) with
nausea and vomiting [6].
Bile stone occurrence depends various etiologies as
the amount of bile salts within bile and cholesterol ratio,
the balance between the factors that stimulate micelle
formation and the ones that prevent it, and infectious
pathologies [7]. Bile duct stones are still the leading reason
of acute recurrent pancreatitis in cholecystectomized
patients. During cholecystectomy; sometimes stones
missed in biliary tract and they cause to cystic duct stump
or intrahepatic litiazis. Especially the stones, which occur
after ERCP and sfincterotomy, have a high prevalence.
In our study; we evaluated the rates of recurrent
biliary pancreatitis seen in patients who had history of
cholecystectomy before. It is discussed if cholecystectomy
is a factor in reducing the prevalence of recurrent
pancreatitis.
Liver function tests and bilirubin levels seen in normal
range for patients having acute biliary pancreatitis.
Considering that, these patients must be evaluated more
carefully. To prevent the calculi remain in the biliary
tract, preoperative cholangiography is preferred during
cholecystectomy. By this, the calculi in the biliary tract can
be spotted and it becomes possible to make intervention
during the operation. Stone extraction can be made by
the exploration of the cystic duct and common bile duct,
and the function of sphincter of Oddi can be preserved
[8, 9]. To apply this procedure, there should be enough
equipment and the surgery team should have the necessary
experience needed. In our study; 13 patients (42%) were
diagnosed as mechanical icterus, findings of cholangitis
were observed in two patients (6%). On the other hand, in
some these patients neither radiologically nor with ERCP,
calculi had been seen. Cholestatic values had been found
above normal limits with biochemical tests.
The usage of intraoperative cholangiography in
every patient is not a cost effective approach. Besides
that, intraoperative cholangiography is not predictive in
detecting small stones and the secondary calculi, which
can occur after the operation. Also, it might be unnecessary
to perform intervention for ones that pass sphincter of
Oddi. Intraoperative cholangiography can be used in
selected cases, which have a doubt about calculi in the preoperative
radiological view of the biliary tract.
Cholecystectomy is suggested to decrease the risk of
acute biliary pancreatitis in patients who have known
calculi in the gall bladder and clinically symptomatic. In
studies done with large patient populations, it has been
seen that early time cholecystectomies (In three days after
the clinic had begun, or six weeks later) after the local or
systemic complications of biliary pancreatitis residue, the
recurrences were seen much less. By this, complication
rate (Biliary colic, choledocholitiazis, cholangitis and
recurrent pancreatitis) which occur due to calculi in the
biliary tract decreases [10].
Sphincterotomy with stone extraction procedure done
with ERCP is the gold standard approach for the calculis in
the common biliary duct. It is not preferred for acute biliary
pancreatitis cases with mild clinic, but can be helpful for
the ones which have associated cholangitis clinic and not
suitable for cholecystectomy [11].
When these two different approaches compared;
ERCP is not superior to cholecystectomy on the long term
to decrease the rates of biliary recurrences, addition
to that it must not be preferred unless necessary [12].
Some of the patients who underwent cholecystectomy
with acute biliary pancreatitis undergo pancreatitis after
cholecystectomy and it is important that patients in such
a risk group can be determined in advance. In our study,
although the number of patients was low it is shown that
patients with previous history of ERCP, or those with high
cholestasis exacerbations in first pancreatitis attack were
in the risky group. Cholecystectomy alone is not enough to
prevent pancreatitis in patients in such a risky group.
CONCLUSION
In our study, it has been stated that only
cholecystectomy, does not prevent the risk of pancreatitis
occurrence completely. Because of that, it must evaluated
in all different aspects such as; clinical course (age, any
other known diseases, previous attacks), ultrasonography
of the biliary tract and MRCP if necessary, and must act
accordingly. Considering the variable periods of time
between each attack, prospective randomized studies
having longer observation times with higher patient
populations are needed.
Conflict of Interest
The authors have declared that no competing interests
exist.
References
- Wang GJ, Gao CF, Wei D, Wang C, Ding SQ. Acute pancreatitis: Etiology
and common pathogenesis. World J Gastroenterol 2009; 15:1427–1430.
[PMID: 19322914]
- Liu CL, Lo CM, Fan ST. Acute biliary pancreatitis: diagnosis and
management. World J Surg 1997; 21:149-54. [PMID: 8995070]
- Cremer A, Arvanitakis M. Diagnosis and management of bile stone
disease and its complications. Minerva Gastroenterol Dietol 2016;
62:103-29. [PMID: 26771377]
- Nesvaderani M, Eslick GD, Cox MR. Acute pancreatitis: update on
management. Med J Aust 2015; 202:420-3. [PMID: 25929504]
- A-Cienfuegos J, Rotellar F. Cholecystectomy in mild acute biliary
pancreatitis: the sooner; the better. Rev Esp Enferm Dig 2016; 108:115-6.
[PMID: 26857120]
- Cappell MS. Acute pancreatitis: etiology, clinical presentation, diagnosis,
and therapy. Med Clin N Am 2008; 92:889–923. [PMID: 18570947]
- European Association for the Study of the Liver. EASL Clinical Practice
Guidelines on the prevention, diagnosis and treatment of gallstones. J
Hepatol 2016; 65:146-81. [PMID: 27085810]
- Halawani HM, Tamim H, Khalifeh F, Mailhac A, Jamali FR. Impact
of intraoperative cholangiography on postoperative morbidity and
readmission: analysis of the NSQIP database. Surg Endosc 2016; 30:5395-
5403. [PMID: 27105616]
- Verma S, Wichmann MW, Gunning T, Beukes E, Maddern G.
Intraoperative cholangiogram during laparoscopic cholecystectomy: A
clinical trial in rural setting. Aust J Rural Health 2016; 24:415-421. [PMID:
27087573]
- Bouwense SA, Besselink MG, van Brunschot S, Bakker OJ, van
Santvoort HC, Schepers NJ, et al. Pancreatitis of biliary origin, optimal
timing of cholecystectomy (PONCHO trial): study protocol for a
randomized controlled trial. Trials 2012; 13:225. [PMID: 23181667]
- Bang KB, Kim HJ, Cho YK, Jeon WK. Does endoscopic sphincterotomy
and/or cholecystectomy reduce recurrence rate of acute biliary
pancreatitis? Korean J Gastroenterol 2015; 65:297-305. [PMID:
25998976]
- Easler JJ, Sherman S. Endoscopic Retrograde
Cholangiopancreatography for the Management of Common Bile Duct
Stones and Gallstone Pancreatitis. Gastrointest Endosc Clin N Am 2015;
25:657-75. [PMID: 26431596]



