Keywords
Adult; Choristoma; Intestinal Obstruction; Intussusception; Jejunum; Ultrasonography
Abbreviations
HP: heterotopic pancreas
INTRODUCTION
Intussusception is defined as the telescoping of a segment of the gastrointestinal tract into an adjacent one. In children this ranks as the most common cause of obstruction and is almost invariably idiopathic. In adults, intussusception is rare accounting for approximately 0.1% of hospital admissions and around 10% of all intussusceptions. In ninety percent of adult cases, a demonstrable cause can be found.
The presence of heterotopic pancreas (HP) is unusual but not rare with an estimated incidence of 0.2% of upper abdominal operations. HP occurs predominantly in the stomach, duodenum and proximal jejunum.
Lesions sited more distally in the distal jejunum and ileum is more rare and generally asymptomatic. Intussusception caused by HP is exceptionally rare.
We report a case of chronic recurrent abdominal pain and subsequent subacute bowel obstruction caused by HP and its successful surgical management.
CASE REPORT
A 27-year-old lady was referred to the gastroenterology clinic for further evaluation of a three-year history of intermittent abdominal pain, borborygmi and alternating bowel habit. Her general practitioner had managed her until recently with antispasmodic medication on the basis of a presumed diagnosis of irritable bowel syndrome.
She described colicky central abdominal pain lasting up to 5 hours per episode in association with alternating bowel habit symptoms, which had worsened over the last nine months to the point where her daily activities were being disrupted and she had at times vomited. Clinical examination was unremarkable.
Initial blood tests included normal full blood count, biochemistry, folate, vitamin B12 and erythrocytes sedimentation rate (ESR). An ultrasound examination was performed to exclude a biliary or bowel cause for her symptoms (Figure 1). The ultrasound examination revealed a loop of abnormal bowel in the pelvis extending to the right iliac fossa over which it was noted that the patient experienced marked tenderness from the ultrasound probe. It contained concentric rings of high and low echogenicity, highly suggestive of a small bowel intussusception. No proximal dilatation was noted. On the basis of this she was referred for laparotomy.
Figure 1. Ultrasound appearance of small bowel
intussusception. Note concentric rings of alternating
echogenicity that are pathonemonic of intussusception.
At laparotomy a long area of jejuno-jejunal intussusception was noted. An enterotomy confirmed the presence of an ulcerated polyp (60x40x35 mm), which was excised and sent for histology. The intussusception was excised and a primary anastamosis performed. Twelve months later, the patient remains symptom free.
Histological examination of the polyp (Figure 2) revealed thick irregular bundles of displaced smooth muscle tissue within which were entwined ductular mucinous and pancreatic exocrine acinar tissue. The histological profile was typical of pancreatic heterotopia.
Figure 2. Histology revealing thick irregular bundles
of displaced smooth muscle tissue within which were
entwined ductular mucinous and pancreatic exocrine
acinar tissue (typical of pancreatic heterotopia). (H&E
stain, magnification x40)
DISCUSSION
Intussusception is primarily a disease of children with only about 5% of cases occurring in adults [1]. An underlying pathological process is usually identifiable in over 90% of cases in adults (compared to an idiopathic cause in the majority of paediatric cases) [2].
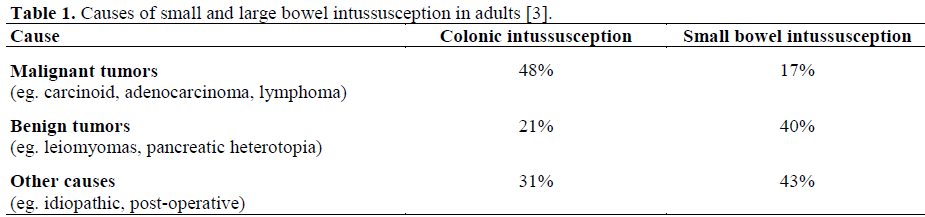
Felix et al. has published the most comprehensive review on intussusception, with more than 1,200 cases from 11 series [3]. Fifty-five percent of cases occur within the small bowel with 45% in the large bowel. Malignant tumours produced nearly half the cases of colonic intussusception. In contrast, predominantly benign tumours caused small bowel intussusceptions. The causes of intussusception are summarised in Table 1. Others have reported similar statistics although Agha reported nearly 60% of malignant small bowel tumours as a cause of intussusception in a small cohort of 25 patients [4]. Postoperative intussusception in adults is also usually rare, albeit that there are several anecdotal case reports. Other reported causes of adult intussusception include Meckels diverticulum, coeliac disease, lymphoma, adenocarcinoma, carcinoid and idiopathic [3, 5, 6].
Klob first described the histological appearance of a heterotopic pancreas in 1859 [7]. The estimated occurrence of heterotopic pancreas is one per 500 upper abdominal operations and up to 5% of autopsy cases [8, 9]. The embryological derivation of heterotopic pancreas is well described [10]. The pancreas is formed from several primitive endodermal evaginations of the primitive duodenal wall. The dorsal diverticulum becomes the body and tail and the ventral portion the head of the pancreas. If one or more of these evaginations remain within the wall of the bowel then these can be carried as longitudinal growth of the intestine continues, leading to ectopic tissue anywhere from the stomach (most common) to the jejunum or ileum (least common). In the latter, HP is usually associated with a Meckel's diverticulum.
Although there are conflicting reports in the literature, approximately half of cases of small bowel HP are asymptomatic [8]. Intussusception caused by HP is rare but has been described previously [8, 11, 12]. Most adult series that have described this complication have noted HP to be located within the ileum where the concomitant existence of a Meckel’s diverticulum is thought to exacerbate the ability of the HP tissue as a lead point for the intussusception. In contrast to this, our report of a jejunojejunal intussusception by HP illustrates an exceptionally rare cause of small bowel obstruction in the adult. As in this case, it appears that only lesions greater than 15 mm become symptomatic [8, 13]. In adults, successful management of intussusception from any cause will invariably involve resection of the lead-point tissue and at times, segmental resection of the involved intestine (as in this case). Surgical resection is often recommended for large bowel intussusception in view of the higher rates of malignancy. This possibility should also be borne in mind in cases of small bowel intussusception despite a reported lower incidence.
In summary, HP remains a rare cause of small bowel obstruction. Its management remains no different to that of intussusception from any cause and the possibility of malignant disease should always be remembered when planning surgery.
Acknowledgments
We thank Dr F Musa for his help in converting histopathology slides into digital images for this paper
References
- Intussusception in infants and adults. Surg Gynecol Obstet 1967; 124:99-105. [PMID 6015799]
- Adult intussusception. AmFam Physician 1993; 47:447-52. [PMID 8430597]
- Adult intussusception; case report of recurrent intussusception and review of the literature. Am J Surg 1976; 131:758-61. [PMID 937658]
- Intussusception in adults. AJR Am J Roentgenol 1986; 146:527-31. [PMID 3484870]
- Adult intussusception. Am J Surg 2003; 186:75-6. [PMID 12842754]
- Intussusception in adults. Review of 160 cases. Am J Surg 1971; 121:531-5. [PMID 5557762]
- Pancreas accessorium. Zeitschrift der Kaiserl. Königl.Gesellschaft der Aerztezu Wien 1859; 15:732.
- The clinical significance of heterotopic pancreas in the gastrointestinal tract. Br J Surg 1981; 68:384-7. [PMID 7237066]
- Pancreatic heterotopia. Review of the literature and reports of 41 authenticated surgical cases, of which 25 were clinically significant. Surg Gynecol Obstet 1946; 82:527-42.
- Aberrant pancreas in the gastric wall. Radiology 1963; 81:107-11. [PMID 14022897]
- Small-bowel obstruction caused by heterotopic pancreas in an adult. Am Surg 1989; 55:503-4. [PMID 2764398]
- Isolated heterotopic pancreas causing intussusception. Eur J Pediatr Surg 2000; 10:197-200. [PMID 10982052]
- Pancreatic heterotopia as a cause of an acute abdomen. Clin Pediatr (Phila) 1986; 25:466-8. [PMID 3742930]



