Keywords
Endosonography; Neuroendocrine Tumors; Pancreatectomy
Abbreviations
HDRBC: heat-damaged red blood cell; IPAS: intrapancreatic accessory spleen; ITP: idiopathic thrombocytopenic purpura; SPECT: single photon emission computed tomography; SPIO: superparamagnetic iron oxide
INTRODUCTION
Ectopic accessory splenic tissue can be found anywhere along the splenic vessels, in the wall of the jejunum, in the mesentery, in the greater omentum, in the pelvis or the left scrotum. Though rarely noticed radiologically, it is relatively common, occurring in approximately 10% of the population according to autopsy studies. Accessory spleens are located at or near the splenic hilum in 80% of the cases. In the remainder of the cases it occurs either in the pancreatic tail or close to it [1, 2]. Accessory spleens usually pose no clinical threat and the radiologic findings of the currently advanced imaging techniques are helpful diagnostic tools for avoiding surgery [3]. The only safe diagnostic method is direct sampling, unless it falsely yields pancreatic islet cells, as in our case. In this report we analyze the case of a surgically treated intrapancreatic accessory spleen (IPAS) which radiologically and cytologically mimicked a neuroendocrine pancreatic tumor.
CASE REPORT
A 60-year-old Caucasian male was referred to our clinic for further evaluation and treatment of an incidental solitary mass, in the body of the pancreas, mimicking an endocrine tumor. In a routine check-up, the patient had a slight elevation of the carbohydrate antigen (CA) 19-9 to 40 U/mL (reference range: 0-37 U/mL). Contrast spiral computed tomography (CT) showed a round homogeneous lesion, 1.2 cm in diameter, located in the upper part of the pancreatic body (Figure 1).
Figure 1. Post contrast CT depicting a small enhancing lesion in the
body of the pancreas. Arrows show the lesion.
Contrast magnetic resonance imaging (MRI) disclosed a round, well-defined mass, 1 cm in diameter, with low signal intensity on T1-weighted images, heterogeneous lesion enhancement during the arterial phase on gadolinium-enhanced T1-weighted images and hyperintensity on fat-saturated T2-weighted images (Figure 2).
Figure 2. MRI T2W (a.) and T1W (b.) images show a hyperintense
lesion in the body of the pancreas (arrows).
Endoscopic ultrasonography (EUS) showed a welldelineated nodule, about 1.2 cm in size, relatively homogeneous with well-defined and smooth margins, increased blood supply and mixed echogenicity. These attributes were compatible with a neuroendocrine tumor. The mass was located in the body of the pancreas, directly peripherally to the celiac trunk and between the pancreatic duct and the gastric wall. No regional lymph nodes or other pathological findings were noted.
An EUS-guided fine needle aspiration (FNA) biopsy resulted in cell clusters of various size, immunopositive for chromogranin, glucagon, gastrin and somatostatin and with a Ki-67 proliferation index less than 2%; these findings were morphologically and immunohistochemically characteristic of a neuroendocrine neoplasm (Figure 3).
Figure 3. a. Uniform small cells (cell block, H&E, x100). b. Positive
chromogranin cell staining (cell block, immunohistochemistry,
x400).
Whole body 111indium-octreotide scintigraphy was negative for somatostatin receptors.
laboratory tests did not reveal any abnormal findings nor were there any tumor markers such as carcinoembryonic antigen (CEA), alpha-fetoprotein (AFP) and CA 19-9 (15 U/mL). Serum levels of glucagon, gastrin and somatostatin were reported as 77.2 pg/mL (reference range: 30-210 pg/mL), 20 pg/mL (reference range: 0-110 pg/mL) and 19.3 pg/mL (reference range: 5-27 pg/mL) respectively. To rule out multiple endocrine neoplasia type 1 syndrome (MEN-1), the following serum hormone levels were measured: parathormone (PTH) intact (82.4 pg/mL; reference range: 15-65 pg/mL), triiodothyronine (T3: 0.9 ng/mL; reference range: 0.7-1.5 ng/mL), thyroxine (T4: 7.4 μg/dL; reference range: 4.5- 12 μg/dL), thyroid stimulating hormone (TSH: 1.8 μIU/mL; reference range: 0.4-4.5 μIU/mL), free thyroxine index, (FTI: 9.7μg/dL; reference range: 6.3- 12.4μg/dL). Pituitary MRI was unremarkable.
On the basis of the above results, a nonfunctioning endocrine tumor was suspected and a distal pancreatectomy with splenectomy was performed. The surgical specimen contained a round, welldemarcated, smooth, dark-red nodule, 1 cm in diameter, surrounded by pancreatic tissue. No other lesions were identified grossly, following meticulous sectioning. Microscopically, the nodule had the structure of a spleen. Thus, the mass was diagnosed as an IPAS (Figures 4 and 5). Eight lymph nodes, identified at the splenic hilum, were benign.
Figure 4. Intrapancreatic spleen (H&E, x100). Arrow shows the wall
of the lesion.
Figure 5. Spleen, white and red pulp (H&E, x100).
DISCUSSION
Ectopic splenic tissue can be classified in two categories: splenosis due to autotransplantation of splenic tissue (usually after splenectomy) and accessory spleens which constitute congenital foci of healthy splenic tissue separated from the main body of the spleen [3]. Embryologically, the spleen is derived from mesenchymal tissue which lies between the layers of the dorsal mesogastrium. During the 6th through the 8th weeks of life, the spleen is in close proximity to the most cephalad extension of the mesonephros [4]. After splenorenal fusion, an accessory spleen may be found pararenally and retroperitoneally or it may descend into the pelvis or scrotum [5]. On gross examination, an IPAS is usually surrounded by a fibrotic capsule which separates it from the adjacent pancreatic parenchyma. Its histology is similar to the orthotopic spleen [6]. Lesions or processes regarding the spleen, such as hemosiderosis, leukemia, lymphoma and hypersplenism can affect accessory splenic tissue. Thus, a careful search for accessory spleens should be considered in the differential diagnosis of nodular densities demonstrated by radiologic study of the pancreas [7].
The existence of an IPAS should be considered when a pancreatic mass has the CT densities and/or MRI signal intensities similar to those of the spleen, on the precontrast and contrast-enhanced images of all imaging modalities. In particular, inhomogeneous enhancement of an IPAS in its early phases may be a diagnostic clue. Angiographic demonstration of a splenic blood supply could be helpful in excluding a pancreatic or an adrenal tumor [3, 8].
Differential diagnosis for intra- and peri-pancreatic accessory spleens might include pancreatic neuroendocrine tumors, lymphoepithelial cysts, lymphomas, hypervascular metastases, solid pseudopapillary tumors and pancreatic adenocarcinomas [9]. Currently, there are no clinical or radiographic criteria for the diagnosis or differentiation of an IPAS from a malignancy [10].
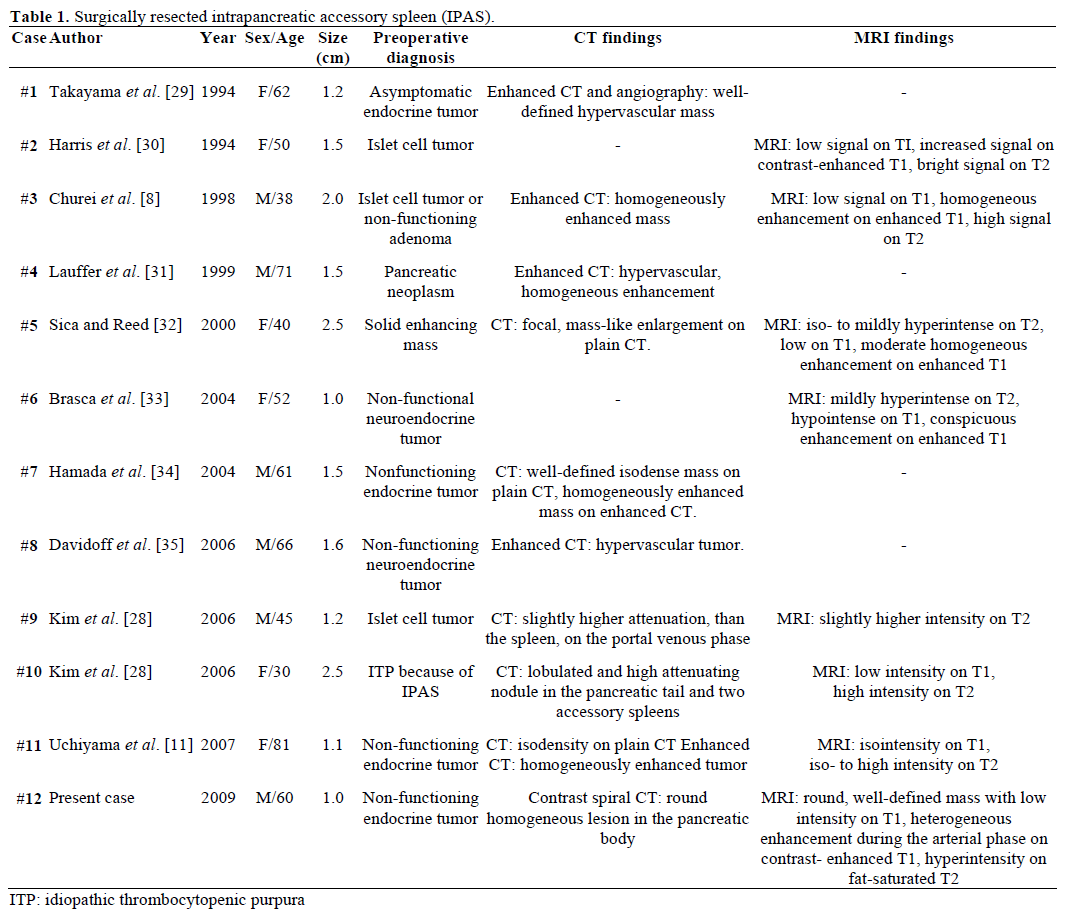
The Radiological findings and preoperative diagnosis of the referred, surgically resected and pathologically confirmed IPAS are summarized in Table 1. Most cases were initially considered to be nonfunctioning endocrine tumors or islet cell tumors and only one in twelve cases was conclusively diagnosed preoperatively as an IPAS after unsuccessful repetitive surgical treatment for idiopathic thrombocytopenic purpura (ITP). The size ranged from 1.0 to 2.5 cm, with a mean value of 1.55 cm [11]. Non-functioning endocrine tumors account for 15-41% of endocrine pancreatic tumors and the rate of their malignant transformation is 62-92%, depending on the type of tumor [12, 13]. Total tumor resection is the ultimate predictor of long-term survival, independently of size, location, histological differentiation, lymph node involvement and other parameters [14].
Since no cut-off size has been established to differentiate between malignant and benign nonfunctioning neuroendocrine tumors of the pancreas, it has been suggested that all such tumors greater than 1 cm should be excised if the patient is a good candidate for surgery [15].
On gray-scale baseline ultrasound, an IPAS is usually seen as a round or oval mass with a mildly echogenic and homogeneous texture, surrounded by a highamplitude interface and showing enhancement behind the lesion. On color or power Doppler ultrasound, a characteristic blood supply (representing the vascular hilum entering the mass), has been reported to offer a 90% sensitivity in the diagnosis of an IPAS [16]. In contrast-enhanced ultrasonography (CEUS) using Levovist® (Schering, Berlin, Germany), an IPAS shows inhomogeneous enhancement in the early vascular phase, enhancement similar to that of spleen during the postvascular phase and prolonged enhancement in the hepatosplenic parenchymal phase [17].
Findings at EUS include a round-to-oval lesion with sharp regular margins and homogenous echo texture, ranging from hypo- to hyper-echoic [18]. EUS-guided FNA cytology reveals a population of predominantly small lymphocytes and a mixed inflammatory infiltrate representing white pulp. A conspicuous vascular component comprised of thin-walled blood vessels representing the splenic sinuses is also observed.. These sinuses are well-visualized on cell block sections. Interestingly, the plump splenic sinus endothelial cells characteristically immunostain for CD8, which is more commonly recognized as a T-cell marker. Staining appears to be specific, because systemic endothelial cells and hemangiomas are negative for CD8 [19, 20, 21]. In cases where FNA of the accessory spleen yields only lymphocytes, without other splenic elements, flow cytometry and immunohistochemistry can be employed to exclude a lymphoproliferative disorder, including Hodgkin’s lymphoma, even if a definitive diagnosis of accessory spleen cannot be confirmed [22, 23]. Schreiner et al. reported three cases of IPAS being diagnosed by EUSguided FNA biopsy [24]. In our case, probably due to sampling of islet cell clusters from the adjacent pancreatic parenchyma, the same procedure was indicative of a neuroendocrine tumor, leading to surgical overtreatment.
A similar false positive EUS-FNA, in which a pancreatic splenic nodule was mistaken for an islet cell tumor has also been reported by Ardengh et al. [25]. In general, EUS-FNA has a high (80-90%) sensitivity and specificity for pancreatic neuroendocrine tumors although its accuracy for such tumors is considered to be lower than that for pancreatic adenocarcinoma [26]. In order to minimize diagnostic errors, EUS-FNA of small neuroendocrine tumors should be performed by experienced endoscopist and cytopathologic assessment should be combined with immunohistochemistry [25].
99mTechnetium heat-damaged red blood cells (99mTc- HDRBC) scintigraphy, combined with single photon emission computed tomography (SPECT), is a highly sensitive and specific method for detection of splenic tissue, since up to 90% of the injected HDRBCs are trapped by this tissue [27]. Although scintigraphy allows selective splenic visualization with an excellent spleen-to-liver ratio, splenic visualization is still difficult in conditions in which minimally functioning splenic tissue is present, as in cases of accessory spleens [8]. Furthermore, scintigraphy, even with SPECT, offers inferior spatial resolution compared to other cross-sectional imaging modalities such as CT or MRI. Therefore, scintigraphy is frequently used in conjunction with other cross-sectional imaging techniques. Moreover, superparamagnetic iron oxide (SPIO)-enhanced MRI is reported as an excellent alternative to 99mTc-HDRBC scintigraphy, when an IPAS has a signal drop similar to that of the spleen. In addition to the referred signal drop, another difference between IPASs and hypervascular pancreatic neoplasms is the heterogeneous enhancement on arterial phase CT scan [28].
Accessory spleens may need surgical treatment when they mimic lymphadenopathies or tumors, or when they become symptomatic due to torsion, spontaneous rupture, hemorrhage or cyst formation. All functional splenic tissue should also be removed for the treatment of hematologic disorders such as ITP.
In conclusion, modern imaging techniques will probably lead to an increasing number of intrapancreatic accessory spleens being discovered in the future, posing significant diagnostic and therapeutic challenges. In such cases all non-invasive diagnostic means should be used in order to obviate unnecessary surgical procedures and decrease overall patient morbidity [3].
Conflict of interest
The authors have no potential conflicts of interest
References
- Halpert B, Gyorkey F. Lesions observed in accessory spleens of 311 patients. Am J Clin Pathol 1959; 32:165-8. [PMID 13670140]
- Halpert B, Alden ZA. Accessory spleens in or at the tail of the pancreas: A survey of 2,700 additional necropsies. Arch Pathol 1964; 77:652-4. [PMID 14130052]
- Kim SH, Lee JM, Han JK, Lee JY, Kim KW, Cho KC, Choi BI. Intrapancreatic accessory spleen: findings on MR Imaging, CT, US and scintigraphy, and the pathologic analysis. Korean J Radiol 2008; 9:162-74. [PMID 18385564]
- Moore K. The developing human. Philadelphia: Saunders, 1986: 225-8.
- Weiand G, Mangold G. Accessory spleen in the pancreatic tail -- a neglected entity? A contribution to embryology, topography and pathology of ectopic splenic tissue. Chirurg 2003; 74:1170-7. [PMID 14673541]
- Davidson ED, Campbell WG, Hersh T. Epidermoid splenic cyst occurring in an intrapancreatic accessory spleen. Dig Dis Sci 1980; 25:964-7. [PMID 7449592]
- Landry ML, Sarma DP. Accessory spleen in the head of the pancreas. Hum Pathol 1989; 20:497. [PMID 2707804]
- Churei H, Inoue H, Nakajo M. Intrapancreatic accessory spleen: case report. Abdom Imaging 1998; 23:191-3. [PMID 9516514]
- Hayward I, Mindelzun RE, Jeffrey RB. Intrapancreatic accessory spleen mimicking pancreatic mass on CT. J Comput Assist Tomogr 1992; 16:984-5. [PMID 1430454]
- Smith CD, Behrns KE, van Heerden JA, Sarr MG. Radical pancreatoduodenectomy for misdiagnosed pancreatic mass. Br J Surg 1994; 81:585-9. [PMID 7911387]
- Uchiyama S, Chijiiwa K, Hiyoshi M, Ohuchida J, Imamura N, Nagano M, et al. Intrapancreatic accessory spleen mimicking endocrine tumor of the pancreas: case report and review of the literature. J Gastrointest Surg 2008; 12:1471-3. [PMID 17929107]
- Eriksson B, Oberg K. PPomas and nonfunctioning endocrine pancreatic tumors: Clinical presentation, diagnosis, and advances in management. In: Mignon M, Jensen RT, eds. Endocrine Tumors of the Pancreas: Recent Advances in Research and Management. Frontiers of Gastrointestinal Research. Basel, Switzerland: Karger, 1995: 208-222.
- Oberg K, Eriksson B. Endocrine tumours of the pancreas. Best Pract Res Clin Gastroenterol 2005; 19:753-81. [PMID 16253899]
- Chung JC, Choi DW, Jo SH, Heo JS, Choi SH, Kim YI. Malignant nonfunctioning endocrine tumors of the pancreas: predictive factors for survival after surgical treatment. World J Surg 2007; 31:579-85. [PMID 17219270]
- Dralle H, Krohn SL, Karges W, Boehm BO, Brauckhoff M, Gimm O. Surgery of resectable nonfunctioning neuroendocrine pancreatic tumors. World J Surg 2004; 28:1248-60. [PMID 15517487]
- Subramanyam BR, Balthazar EJ, Horii SC. Sonography of the accessory spleen. AJR Am J Roentgenol 1984; 143:47-9. [PMID 6610329]
- Kim SH, Lee JM, Lee JY, Han JK, Choi BI. Contrast-enhanced sonography of intrapancreatic accessory spleen in six patients. AJR Am J Roentgenol 2007; 188:422-8. [PMID 17242251]
- Barawi M, Bekal P, Gress F. Accessory spleen: a potential cause of misdiagnosis at EUS. Gastrointest Endosc 2000; 52:769-72. [PMID 11115915]
- Syed S, Zaharopoulos P. Thoracic splenosis diagnosed by fineneedle aspiration cytology: a case report. Diagn Cytopathol 2001; 25:321-4. [PMID 11747224]
- Carlson BR, McQueen S, Kimbrell F, Humphreys S, Gentry HL, Esbenshade A. Thoracic splenosis. Diagnosis of a case by fine needle aspiration cytology. Acta Cytol 1988; 32:91-3. [PMID 2447727]
- Kraus MD. Splenic histology and histopathology: an update. Semin Diagn Pathol 2003; 20:84-93. [PMID 12945932]
- Renne G, Coci A, Biraghi T, Schmid C. Fine needle aspiration of thoracic splenosis. A case report. Acta Cytol 1999; 43:492-4. [PMID 10349388]
- Pugh JL, Jhala NC, Eloubeidi MA, Chhieng DC, Eltoum IA, Crowe DR, et al. Diagnosis of deep-seated lymphoma and leukemia by endoscopic ultrasound-guided fine-needle aspiration biopsy. Am J Clin Pathol 2006; 125:703-9. [PMID 16707371]
- Schreiner AM, Mansoor A, Faigel DO, Morgan TK. Intrapancreatic accessory spleen: mimic of pancreatic endocrine tumor diagnosed by endoscopic ultrasound-guided fine-needle aspiration biopsy. Diagn Cytopathol 2008; 36:262-5. [PMID 18335556]
- Ardengh JC, de Paulo GA, Ferrari AP. EUS-guided FNA in the diagnosis of pancreatic neuroendocrine tumors before surgery. Gastrointest Endosc 2004; 60:378-84. [PMID 15332027]
- Voss M, Hammel P, Molas G, Palazzo L, Dancour A, O'Toole D, et al. Value of endoscopic ultrasound guided fine needle aspiration biopsy in the diagnosis of solid pancreatic masses. Gut 2000; 46:244-9. [PMID 10644320]
- Ota T, Tei M, Yoshioka A, Mizuno M, Watanabe S, Seki M, et al. Intrapancreatic accessory spleen diagnosed by technetium-99m heat-damaged red blood cell SPECT. J Nucl Med 1997; 38:494-5. [PMID 9074546]
- Kim SH, Lee JM, Han JK, Lee JY, Kang WJ, Jang JY, et al. MDCT and superparamagnetic iron oxide (SPIO)-enhanced MR findings of intrapancreatic accessory spleen in seven patients. Eur Radiol 2006; 16:1887-97. [PMID 16547707]
- Takayama T, Shimada K, Inoue K, Wakao F, Yamamoto J, Kosuge T. Intrapancreatic accessory spleen. Lancet. 1994; 344:957- 8. [PMID 7934372]
- Harris GN, Kase DJ, Bradnock H, Mckinley MJ. Accessory spleen causing a mass in the tail of the pancreas: MR imaging findings. AJR Am J Roentgenol 1994; 163:1120-1. [PMID 7976887]
- Läuffer JM, Baer HU, Maurer CA, Wagner M, Zimmermann A, Büchler MW. Intrapancreatic accessory spleen.A rare cause of pancreatic mass. Int J Pancreatol 1999; 25:65-8. [PMID 10211424]
- Sica GT, Reed MF. Intrapancreatic accessory spleen. Radiology 2000; 217:134-7. [PMID 11012435]
- Brasca LE, Zanello A, De Gaspari A, De Cobelli F, Zerbi A, Fazio F, Del Maschio A. Intrapancreatic accessory spleen mimicking a neuroendocrine tumor: magnetic resonance findings and possible diagnostic role of different nuclear medicine tests. Eur Radiol. 2004; 14:1322-3. [PMID 14615901]
- Hamada T, Isaji S, Mizuno S, Tabata M, Yamagiwa K, Yokoi H, Uemoto S. Laparoscopic spleen-preserving pancreatic tail resection for an intrapancreatic accessory spleen mimicking a nonfunctioning endocrine tumor: report of a case. Surg Today 2004; 34:878-81. [PMID 15449162]
- Davidoff S, Fernandes A, Sideridis K, Gecelter G, Bragdon J, Bank S. Clinical challenges and images in GI. Intrapancreatic accessory spleen mimicking nonfunctioning neuroendocrine tumor. Gastroenterology 2006; 131:350, 689. [PMID 16938927]





